





Abstract
Although pulmonary thromboendarterectomy is an effective modality for the treatment of chronic thromboembolic pulmonary hypertension (CTEPH), the mortality in patients with severe haemodynamic disease is still high. Recently it was reported that fractional pulse pressure (pulmonary arterial pulse pressure/mean pulmonary arterial pressure) was higher in CTEPH than in primary pulmonary hypertension (PPH). It was hypothesized that fractional pulse pressure might be low in CTEPH with inaccessible distal thrombi and/or secondary pulmonary hypertensive change, resulting to the high operative mortality.
To determine the influence of fractional pulse pressure to the outcome of surgery, 32 patients with CTEPH who had thromboendarterectomy between 1985 and 1998 were studied. Pulmonary haemodynamics and fractional pulse pressure were compared between survivors (n=26) and nonsurvivors (n=6) postoperatively. Those parameters in PPH (n=18) and large vessel pulmonary arteritis (n=6) were also analysed.
Fractional pulse pressure in CTEPH (1.23±0.21) was significantly higher than in PPH (0.93±0.22; p=0.0017) and lower than in pulmonary arteritis (1.69±0.32; p=0.03). Fractional pulse pressure in survivors (1.26±0.21) was significantly higher than in nonsurvivors (1.06±0.16; p=0.03). Fractional pulse pressure is a significant predictor for mortality in patients with high pulmonary vascular resistance >1100 dynes·sec·cm−5.
To conclude fractional pulse pressure in addition to pulmonary vascular resistance might be useful in predicting for the outcome of surgery, especially in patients with severe haemodynamic impairment.
- chronic thromboembolic pulmonary hypertension
- prognosis
- pulmonary hypertension
- pulmonary thromboendarterectomy
- pulse pressure
This study was supported in part by a Research Grant for intractable Diseases from the ministry of Health and Welfare, Japan.
Although pulmonary thromboendarterectomy is an effective modality for the treatment of chronic thromboembolic pulmonary hypertension (CTEPH) 1–15, the mortality in patients with high pulmonary vascular resistance is still high 8, 9. The inability to reduce pulmonary vascular resistance is a major risk factor associated with high mortality 4, 9.
Chronic pulmonary hypertension of any origin frequently results in pathological change in the proximal (elastic) and distal (resistive) pulmonary vasculature. The obstruction or significant stenosis of large pulmonary artery increased pulse pressure (systolic pressure-diastolic pressure) as well as characteristic impedance, and reduced wave reflection 16, 17. Grant et al. 16 reported that the degree of the right ventricular hypertrophy was dependent on the increase in pulse pressure rather than the increase in mean pulmonary arterial pressure 16, 18. However, primary pulmonary hypertension (PPH) and CTEPH generally induce severe haemodynamic disturbances in accordance to the increase of pulmonary vascular resistance or mean pulmonary arterial pressure compared to unilateral pulmonary arterial occlusion. Consideration of both impedance (i.e. the opposition to the pulsatile components of flow) and pulmonary vascular resistance (i.e. the opposition to the mean components of flow) are required to evaluate the right ventricular afterload, and these two measurements among pulmonary hypertensive diseases are thought to be different because of the different location of involved lesions in pulmonary arterial trees.
Recently it was reported that the pulsatility as the ratio of pulse pressure to mean pressure (i.e. fractional pulse pressure of the pulmonary artery: PPf) in CTEPH was larger than in PPH, because of the difference of involved pathology 19. They hypothesized and explained their findings in the following way. In CTEPH, thrombi obstruct the proximal arteries preferentially (i.e. from the main pulmonary artery to segmental arteries). Therefore, it is likely that the thrombi attached to the proximal arteries mechanically stiffen the arterial wall and increase proximal resistance without comparably increasing peripheral arterial resistance. In contrast, PPH primarily involves peripheral segment of pulmonary arterial trees. The vascular change in PPH would increase peripheral arterial resistance. Increases in stiffness and resistance in the proximal arteries would increase pulse pressure, whereas those in peripheral arteries increase mean arterial pressure.
It is hypothesized that PPf might be low in CTEPH with inaccessible distal thrombi and/or secondary pulmonary hypertensive changes 20, resulting to the high operative mortality.
In the present report, the influence of PPf on the outcome of surgery in CTEPH was retrospecitvely investigated, and the usefulness of PPf in the differential diagnosis between CTEPH and other pulmonary hypertensive diseases (PPH and large vessel pulmonary arteritis with central pulmonary arterial stenosis 21–25) was reassessed.
Patients and methods
A total of 32 patients with CTEPH (22 females, 10 males; mean±sd age 51±13, range 22–73) were operated on between April 1985 and March 1998 at Chiba University Hospital. CTEPH was defined as mean pulmonary arterial pressure (mean Ppa) ≥25 mmHg with a mean pulmonary arterial wedge pressure <12 mmHg in patients who had dyspnoea on exertion for a duration of >6 months. In addition, lung perfusion scans were required to show segmental or larger defect concomitant with normal ventilation scan study. Finally, thromboembolic obstruction was confirmed by pulmonary angiography 26.
The selection criteria for pulmonary thromboendarterectomy were slightly modified from those defined by Moser et al. 3. The criteria were as follows 9: 1) mean Ppa ≥30 mmHg, resulting in calculated pulmonary vascular resistance (PVR) >300 dynes·sec·cm−5 even after oral anticoagulant therapy for >6 months; 2) dyspnoea on exertion according to Fletcher and Hugh-Jones classification (H-J) 27 ≥grade 3; 3) thrombi defined as accessible to current surgical technique (main, lobar, segmental arteries); 4) the absence of severe associated disease.
During the same period, 18 patients were diagnosed as PPH (13 females, five males; mean age 37±11 yrs, range 16–64), and six patients (five females, one male; mean age 53±10 yrs, range 38–67) were diagnosed as large vessel pulmonary arteritis with central pulmonary arterial stenosis. PPH was defined as mean Ppa ≥25 mmHg with mean pulmonary wedge pressure <12 mmHg. Other possible aetiologies of pulmonary hypertension, such as mitral valve diseases, congenital heart failure, left ventricular failure, collagen vascular disease, and portal hypertension were excluded. In addition, lung perfusion scans were required to show normal or small patchy perfusion defects without larger than segmental defects concomitant with normal ventilation scans. Six patients with large vessel pulmonary arteritis were confirmed by pulmonary angiograms with the findings of central (main or lobar) arterial stenosis. Of that group, three patients were associated with Takayasu's arteritis with systemic arterial involvement 23–25 and the remaining three patients were thought to have idiopathic isolated pulmonary arteritis without any systemic arterial involvement 18, 19.
Measurement of haemodynamic variables
Haemodynamic variables were measured in supine position while breathing room air. After venous access was achieved via internal jugular vein, right-side heart catheterization was performed using a fluid-filled system that included a balloon-tipped, flow-directed catheter (7.5 F Swan-Ganz catheter). Transducers were positioned at the mid-axillary line and zeroed at atmospheric pressure. The measurement of pulmonary arterial pressure was performed in the pulmonary arterial trunk proximal to stenotic lesions by thrombi or vasculitis. Six waves including three waves at end-expiration were recorded. A hard copy was made of the pressure tracing using a chart recorder at a paper speed of 50 mm·s−1. Cardiac output (Q') was measured in triplicate by the thermodilution technique. Cardiac index (CI) was calculated as Q' divided by body surface area. PVR was calculated conventionally as the ratio of the difference between mean Ppa and pulmonary wedge pressure to Q'.
Fractional pulse pressure
As shown in figure 1⇓, the pulsatility as the ratio of pulse pressure to mean Ppa (fractional pulse pressure: PPf) was characterized according to those by Nakayama et al. 19, while mean Ppa was calculated by the integration from the pressure wave at a sampling rate of 250 points per second. Three waves at end-expiration were used for calculating PPf.

Schematic representation of waveform. Fractional pulse pressure (PPf) is calculated as PPf=pulse pressure/mean Ppa and is indicated by the dashed vertical line. PPf is the ratio of pulse pressure to mean pulmonary arterial pressure (═) according to Nakayama et al. 19.
Pulmonary thromboendarterectomy
In 16 cases, a lateral thoracotomy 9–14 to one lung was used, which contained the dominant thrombus judged by ventilation-perfusion scans and pulmonary arteriogram.
In 16 cases, a median sternotomy with the use of deep hypothermia and circulatory arrest 1–10 was used. Although 14 patients were endarterectomized bilaterally, the remaining two patients were endarterectomized unilaterally, because thrombi on the contralateral side were located too distal 9, 15.
As for the period of time, 14 patients (three with median sternotomy; 11 with lateral thoracotomy) were operated on between 1986 and 1991, and 18 (thirteen with median sternotomy; five with lateral thoracotomy) were operated from 1992.
In all patients, inferior vena cava filters were placed postoperatively unless a previous interruptive procedure had been done.
Analysis
PPf and cardiorespiratory variables were compared between CTEPH, PPH and pulmonary arteritis to reassess the usefulness of this parameter for the differential diagnosis of pulmonary hypertensive diseases. In CTEPH who had pulmonary thromboendarterectomy, PPf, other preoperative parameters, and operative approach were compared between survivors and nonsurvivors who died within 30 days after surgery. In the limited patients with high PVR (>1,100 dynes·sec·cm−5), those parameters were also compared between survivors and nonsurvivors. To know whether PPf is a better predictor for mortality than PVR or not, correlation coefficient between them was calculated, and if it was not significant, both were included in the multivariate logistic regression analysis for operative mortality.
Statistical analysis
Values are presented as means±sd. Comparisons of three groups (CTEPH, PPH, pulmonary arteritis) were performed by a nonparametric Kruskal-Wallis analysis of variance with Sheffe's test for multiple comparisons. Comparisons between survivors and nonsurvivors were made using a Mann-Whitney U-test and Chi-squared test, as appropriate. A p<0.05 was taken as statistically significant.
Results
The cardiorespiratory variables of three groups are shown in table 1⇓. The mean age in PPH was younger than in CTEPH or pulmonary arteritis. Arterial oxygen tension (Pa,O2) in CTEPH was lower than in others, while arterial carbon dioxide tension (Pa,CO2) in CTEPH and PPH was lower than in pulmonary arteritis. Mean and diastolic Ppa, and PVR in CTEPH were lower than in PPH, while systolic Ppa, and CI in CTEPH were similar to in PPH. Systolic, mean, diastolic Ppa and PVR in pulmonary arteritis were significantly lower than in others.
Comparison of cardiorespiratory data
Illustrated in figure 2⇓ are the examples of waveforms and angiographic findings of pulmonary artery for PPH, pulmonary arteritis, CTEPH (survivors, nonsurvivors). The waveforms between PPH and pulmonary arteritis were different, and PPf in PPH (0.59) was lower than in pulmonary arteritis (1.72). The angiogram in pulmonary arteritis showed complete obstruction of the right main pulmonary artery and stenosis of the left lower branch, while the angiogram in PPH showed marked pruning of the distal vessels.
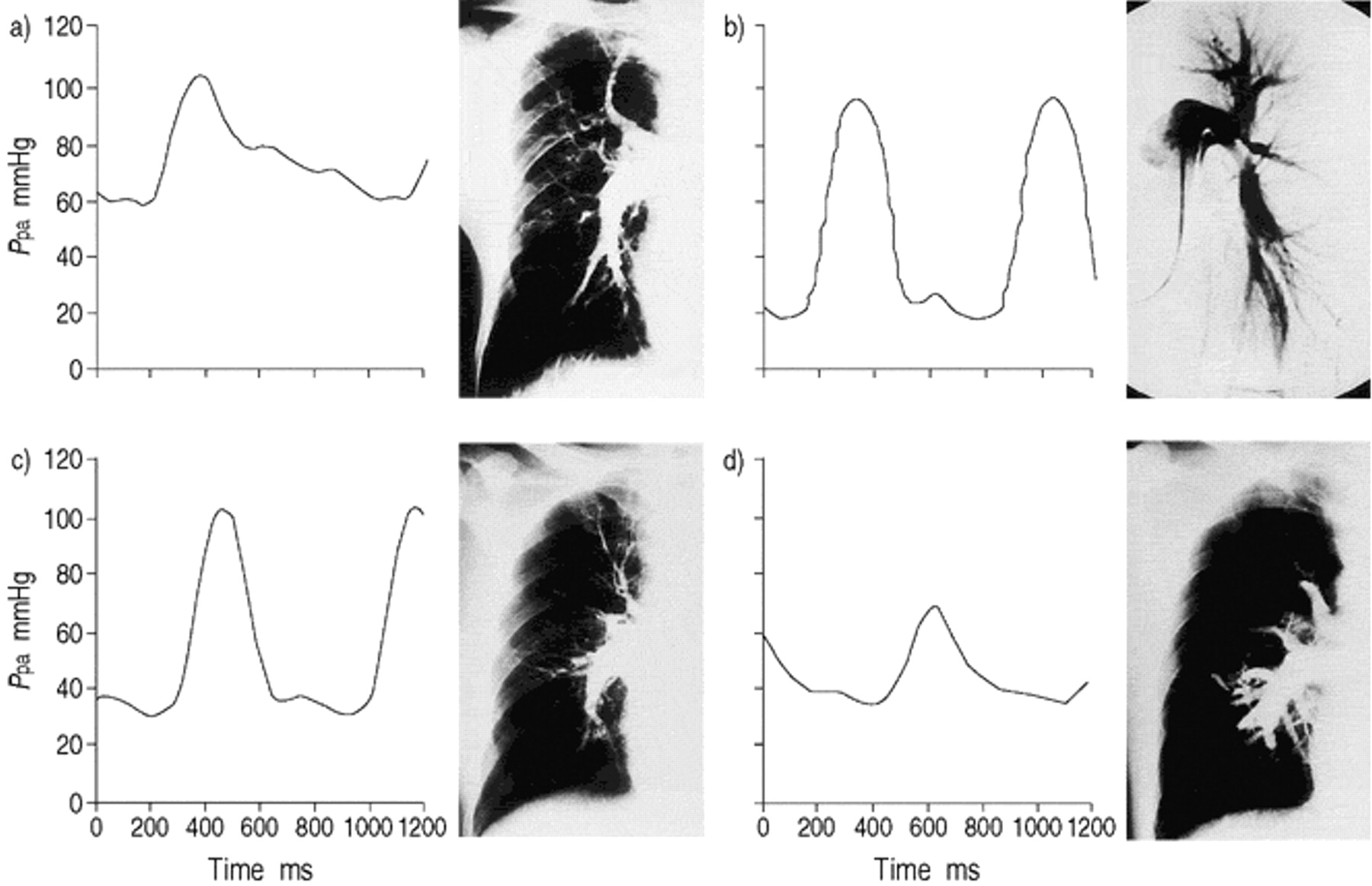
The examples of waveforms and angiographic findings. a) Primary pulmonary hypertension: mean pulmonary arterial pressure (Ppa)=74 mmHg, pulmonary vascular resistance (PVR)=2460 dynes·sec·cm−5, fractional pulse pressure (PPf)=0.59. Marked pruning of the distal vessels was noted while the perfusion scan showed small patchy perfusion defects. b) Pulmonary arteritis: mean Ppa=44 mmHg, PVR=433 dynes·sec·cm−5, PPf=1.72. Complete obstruction of the right main pulmonary artery and stenosis of the left lower branch was observed. c) chronic thromboembolic pulmonary hypertension (CTEPH) (survivor): mean Ppa=50 mmHg, PVR=918 dynes· sec·cm−5, PPf=1.42. The proximal sites of thrombi were in lobar arteries. d) CTEPH (nonsurvivors): mean Ppa=44 mmHg, PVR=953 dynes·sec·cm−5, PPf=0.77. The thrombi were mostly located in segmental or subsegmental arteries.
As shown in table 1⇑ and figure 3⇓, mean value of PPf in CTEPH (1.23±0.21) was significantly (p=0.017) higher than in PPH (0.93±0.22) and significantly (p= 0.033) lower than in pulmonary arteritis (1.69±0.32). The distribution of PPfs in CTEPH was wide and overlapped with the distribution of PPfs in PPH.

Comparison of fractional pulse pressure (PPf) between primary pulmonary hypertension (PPH; n=18), chronic thromboembolic pulmonary hypertension (CTEPH; n=32), pulmonary arteritis. *: p=0.0017, **: p=0.033, ***: p<0.00001: Kruskal-Wallis analysis of variance with Sheffe's test for multiple comparison. Open circles: mean values; bars:±sd.
In CTEPH who had pulmonary thromboendarterectomy, 24 patients survived and their pulmonary haemodynamics significantly improved (mean Ppa preoperative: 46.1±7.8; postoperative: 28.6±8.1 mmHg, PVR preoperative: 815±270; postoperative: 377±165 dynes·sec·cm−5). Six deaths (18.8%) occurred within 30 days after surgery. The mortality for surgery was 21.5% (3/14) between 1985 and 1991, and 16.7% (3/18) from 1992. The mortality of lateral thoracotomy was 12.5%, and that of median sternotomy was 25% (table 2⇓), but preoperative mean Ppa was slightly (p=0.06) higher in median sternotomy (50±8 mmHg) than that in lateral thoracotomy (45±7). Five patients died of right heart failure postoperatively, because we could not endarterectomize distal, enough to achieve improvement of pulmonary haemodynamics. One patient died of cardiac tamponade one week after surgery.
Comparison of preoperative parameters between survivors and nonsurvivors
As shown in table 2⇑, mean right atrial pressure (mean Pra), diastolic Ppa, CI, PVR in nonsurvivors were significantly worse than in survivors. In the survivor in which proximal sites of thrombi were located in lobar arteries, waveform was similar to pulmonary arteritis, and PPf was high (fig. 2c⇑), while in the nonsurvivor in which most thrombi were located in segmental or subsegmental arteries, waveform was similar to PPH, and PPf was low (fig. 2d⇑). The PPf in survivors (1.26± 0.21) was significantly (p=0.03) higher than in nonsurvivors (1.06±0.16).
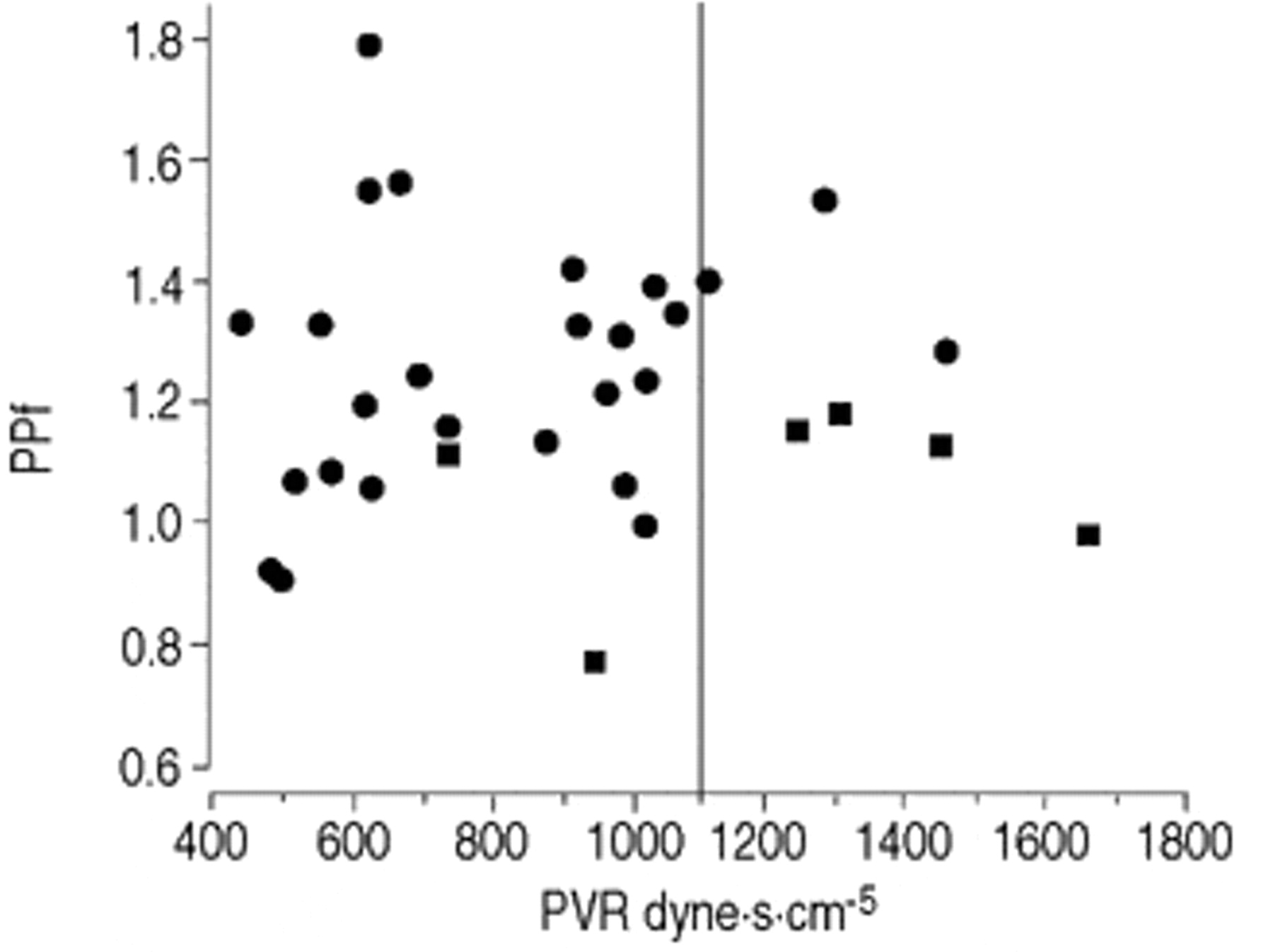
Figure 4⇓ plots PVR versus PPf referring to the outcome of surgery. According to the PVR (1100 dynes·sec·cm−5) which was previously reported to be one of predictable risk factors 8, 32 patients were divided into two groups. In patients with a high PVR (>1100 dynes·sec·cm−5) (n=7), the mortality was 57.1%, compared to 8.0% in those (n=25) with a low PVR (<1100 dynes·sec·cm−5). All nonsurvivors had PPf <1.2. PPf was not correlated with PVR (r=−0.04, ns), and both were included in the multivariate logistic regression for the analysis of mortality. Table 3⇓ shows the results of multivariate logistic regression analysis. PVR was a significant predictor (p=0.017), while PPf was marginally significant (p=0.05).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The outcome of surgery for chronic thromboembolic pulmonary hypertension (CTEPH) (pulmonary vascular resistance) versus fractional pulse pressure (PPf)). Mortality rate was 18.8%. In patient (n=7) with a high PVR (>1100 dynes·sec·cm−5), the mortality was 57.1%, compared to 8.0% in those (n=25) with a low PVR (<1100 dynes·sec·cm−5). All nonsurvivors had a low PPf (<1.2). PPf was not correlated with PVR (n=32, r= −0.04). •: survivors (n=26); ▪: nonsurvivors (n=6).
Multivariate logistic regression analysis
In the limited patients with a high PVR (>1100 dynes·sec·cm−5) the various predictors for mortality between survivors and nonsurvivors were also compared. PPf in nonsurvivors (1.11±0.09) was significantly (p=0.03) lower than in survivors (1.41±0.12). Other predictors (Pra, diastolic Ppa, CI, PVR) did not reach significance (p=0.72, 0.16, 0.16, 0.48, respectively).
Discussion
This study shows that: 1) PPf in CTEPH was significantly higher than that in PPH and significantly lower than that in pulmonary arteritis with central arterial stenosis, but the distribution of PPfs in CTEPH was wide and overlapped with PPfs in PPH. 2) PPf influenced the operative mortality and low PPf was a useful predictor for the poor outcome of surgery in patients with a high PVR >1100 dynes·sec·cm−5.
The operative mortality associated with pulmonary thromboendarterectomy has markedly decreased at University California at San Diego 5. The mortality in other institutions, however, was still high (16–23%) 7–12, 15. Severe haemodynamic disorder (PVR >1100 dynes·sec·cm−5) predicted the high operative mortality at both Illinois study 8 and the present study. The most important cause of mortality for pulmonary thromboendarterectomy is inability to reduce pulmonary arterial pressure as a result of distal disease that proves inaccessible, and/or secondary pulmonary hypertensive change 4, 9. Recently it was reported that the pulsatility as the ratio of pulse pressure to mean pressure (PPf) in CTEPH was larger than in PPH due to the difference of primary involved lesions 19. The present authors reassessed their data and hypothesized that PPf might be low in CTEPH with inaccessible distal thrombi and/or secondary pulmonary hypertensive change. Although the difference of PPf was found among various pulmonary hypertensive diseases, the most significant findings were that PPfs were widely distributed in CTEPH. PPf in addition to PVR was useful in predicting operative mortality, especially in patients with severe haemodynamic impairment. Several issues need to be considered in the interpretation of these results.
Firstly, larger PPf was shown in CTEPH compared to PPH. This is partly consistent with the results of Nakayama et al. 19. However, a clear distinction could not be shown between CTEPH and PPH by PPf, because the present data were widely distributed, in contrast to the data of Nakayama et al. 19. Both studies hypothesized that CTEPH should have stiffness or high resistance in proximal arteries, whereas PPH should have high resistance in peripheral arteries, and these differences in the primary lesions would make arterial pulse pressure relative to mean arterial pressure larger in CTEPH than in PPH. However CTEPH could have secondary hypertensive change in the peripheral artery and/or distal thrombi. The present study might have included more distal diseases, because mean PPf in CTEPH in this study is significantly lower than in Nakayama et al. 19 (1.23±0.21 and 1.41±0.20 respectively, p=0.0003, unpaired t-test).
Secondly, only PPf was used to analyse pulsatile components of right ventricular afterload. Recently Castelain et al. 28 reported that CTEPH and PPH had similar PPf using high fidelity pressure catheter. They also quantified wave reflection 16, 28–33 by measuring ti, i.e. the time between pressure upstroke and systolic inflection point (Pi); ΔP, i.e. systolic Ppa minus Pi; and augmentation index (ΔP/pulse pressure) 30 which quantifies the extent of wave reflection. They showed that CTEPH had shorter ti and higher ΔP/pulse pressure, and suggested that CTEPH had increased and anticipated wave reflection compared to PPH. The difference between two studies might arise from the difference of measurements. High-fidelity pressure catheter was not used and the wave reflection was not quantified. Although it is agreed that wave reflection is different between CTEPH and PPH, Castelain et al. 28 used small number of patients (PPH n=7, CTEPH n=7) and, mean PPf (0.97) in CTEPH was larger than PPH (0.89) in their report. In large series, PPf in CTEPH could be significantly larger than PPH, although CTEPH could not be differentiated from PPH by only PPf.
Stiffening of the proximal arteries by the thrombi and arteritis could increase characteristic impedance of the pulmonary artery. Several investigators have attributed the increase of pulse pressure to the decreased arterial compliance and increased characteristic impedance in systemic arteries 32–37. Similarly Grant and coworkers 16, 17 showed that stiffening of the pulmonary artery increased pulse pressure. It is unlikely that the reflection wave is related to increased pulse pressure in pulmonary arteritis, because in their other experiment the ensnarement of pulmonary artery increased pulse pressure and characteristic impedance, but had little effect on wave reflection 16, 18. Both increased characteristic impedance and early and increased reflection wave could accentuate pulse pressure and PPf in CTEPH.
Thirdly, low PPf was shown as the possible preoperative risk factor for pulmonary thromboendarterectomy in patients with a high PVR. Hartz et al. 8 reported that the patients with high PVR >1100 dynes·sec·cm−5 have a high likelihood of operative mortality, and perhaps should not undergo pulmonary thromboendarterectomy except at limited institutions where the operations are performed frequently. It was shown that PVR is more useful in predicting the operative mortality than PPf. However, thromboendarterectomy has been performed even in high risk patients, because the mortality of lung transplantation for pulmonary hypertension is still high 15, 38, and furthermore it has not been performed in Japan. More precise operative criteria in infrequently performed institutions are needed. It is important to accurately evaluate distal thrombi and secondary pulmonary hypertensive change. Nevertheless, it is difficult to make a precise diagnosis by angiography and even by angioscopy 6, 39. The assessment of PPf as well as angiogram could be helpful to decide the accessibility to thrombi. This study suggests that in the patient with only a few thrombi and high PVR, low PPf might be related to secondary pulmonary hypertensive change and/or distal thrombi, resulting in high operative mortality.
Finally, the most important limitation in this study is that a fluid-filled system was used to record pulmonary arterial pressure. As recorded pressures, the catheter was fluoroscopically placed to minimize catheter whip to keep that artifact at minimum. If a high fidelity pressure transducer could have been used, the recorded pressure waveform would have been more accurate. However, the authors think the fluid-filled system is simpler and easier to use than high fidelity pressure system. Considering PPf in addition to pulmonary vascular resistance and angiograms gives important and useful information for clinical differential diagnosis of pulmonary hypertensive diseases.
It has been reported that pulmonary artery impedance and pulsatile properties must be taken into consideration to understand right ventricular-pulmonary artery coupling 16, 33. The data are limited in fractional pulse pressure, but more precise assessment of pulsatile components using high-fidelity catheter as well as large series study for the influence of fractional pulse pressure to surgical outcome will be needed.
Acknowledgments
The authors thank W.W. Wagner, Jr. for helpful criticism of the manuscript.
- Received November 25, 1999.
- Accepted October 10, 2000.
- © ERS Journals Ltd
References









