





Abstract
Burkholderia cepacia is a plant phytogen and is known as a hardy and versatile organism.
Over the past two decades it has emerged as a pathogen in the cystic fibrosis (CF) community, with devastating effects. Pulmonary colonisation can lead to an accelerated decline in lung function. In some cases, it causes a rapid and progressive pneumonic illness termed “cepacia syndrome”, which is untreatable and fatal.
B. cepacia is inherently resistant to multiple antibiotics and highly transmissible and virulent strains have been identified. CF patients colonised with the organism have to be segregated from their peers to try to prevent cross-infection.
However, the pathogenicity of B. cepacia is not limited to CF. Other groups, such as individuals with chronic granulomatous disease and immunocompromised patients are vulnerable and it has caused disease in healthy individuals. However, the agricultural and petrochemical industries are attempting to exploit properties of B. cepacia for use as a biopesticide and biodegradation agent.
This article provides an up to date review of clinically based literature on the Burkholderia cepacia complex, highlighting clinical management issues for both cystic fibrosis and non-cystic fibrosis patients. The article also addresses the potential conflict between medicine and agriculture on plans to reintroduce strains of Burkholderia cepacia back into the environment.
- agricultural industry
- Burkholderia cepacia
- cystic fibrosis
- petrochemical industry
- pulmonary colonisation
The worst thing that can happen to a physician working in a cystic fibrosis (CF) centre is to be confronted with a report from the microbiologist identifying Burkholderia cepacia for the first time in the sputum of a CF patient. The clinician then must inform the patient that they are infected with a transmissible organism that can potentially shorten survival by a decade 1. The consequences for the CF patient are clearly much worse. Socially, they will be segregated from their peers. Clinically, it is likely that their disease will accelerate with increasing morbidity and mortality. Currently, eligibility for lung transplantation is a subject for debate and controversy 2. It is recognized that a significant number of B. cepacia patients have a poor outcome following transplantation 2, 3.
Although the percentage of CF patients in a CF centre infected with B. cepacia is small, the literature output has increased exponentially over the last five years. The main thrust of these papers has concentrated upon taxonomy and microbial classification. This article will cover current knowledge of these areas, concentrating on their impact on clinical management of B. cepacia positive patients.
Hospitals are being increasingly recognised as dangerous places for cross-infection, either between patients or from the hospital environment. Nosocomial infections can occur, potentially with multidrug-resistant organisms, including methicillin-resistant Staphylococcus aureus, Enterococcus, Pseudomonas and sometimes Aspergillus species. B. cepacia can now be added to this list, following recent reports describing the organism cross-infecting non-CF hospitalised patients with resultant morbidity 4. The impact of this knowledge is discussed for both hospitalised CF and non-CF patients.
B. cepacia is also a biopesticide and has potential use for protecting crops. This environmental application is an area of potential conflict between the agriculturalists and scientists, as to whether a human pathogen should be placed in the environment 5. The beneficial uses of B. cepacia outside the medical field are discussed.
Historical
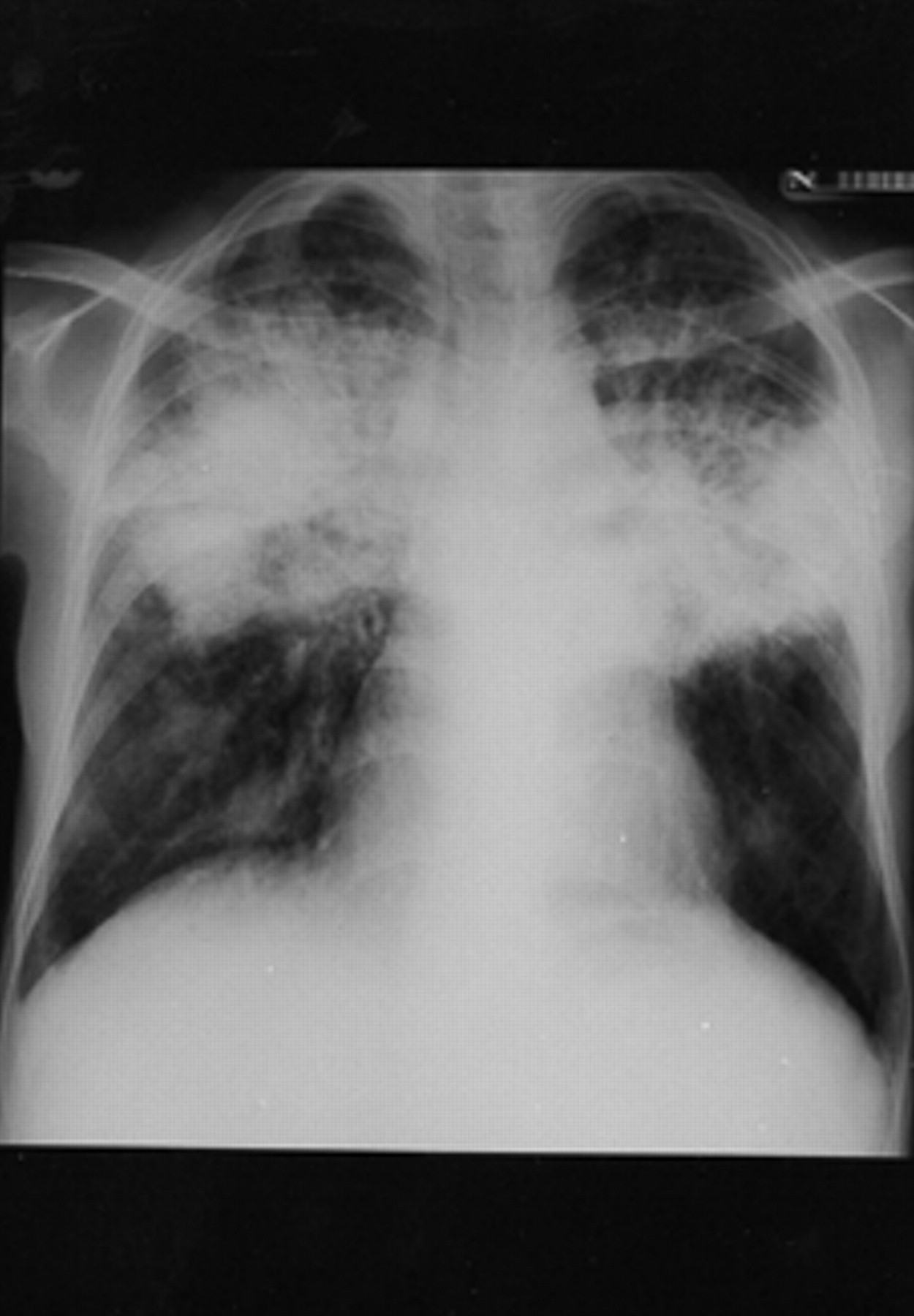
The organism, a gram-negative motile rod, was first described by Burkholder 6 in 1950 as a plant pathogen and a cause of onion rot (fig. 1⇓). Although hospital outbreaks in non-CF patients had been previously described, it was not until the early 1980s that an increasing incidence and prevalence of B. cepacia isolates were noted in North American CF centres 7, 8. These reports also described an increased morbidity and mortality in those patients infected with B. cepacia. In particular, the authors described “cepacia syndrome”, when patients succumbed rapidly to a pneumonic illness with high temperatures and respiratory failure unlike any clinical situation found with other CF pathogens (fig. 2⇓). The reduction of incidence by one centre using strict infection control measures suggested that person-to-person transmission was the main factor for cross-infection 9. The proof of cross infection occurring both in hospitals and in the community was established in seminal papers by LiPuma and coworkers 10, 11 and Govan et al. 12, which showed patients shared the same strain of organism. It is against this background of knowledge that an enormous amount of research has been undertaken in the last decade into the microbiology of B. cepacia and how this information can be translated into therapeutic benefit for CF patients infected with B. cepacia.
Microbiology and taxonomy
B. cepacia has various characteristics that set it aside from other CF pathogens. It is highly transmissible, has inherent resistance to multiple antibiotics and is associated with greater virulence; it is these combined factors which make the management of B. cepacia patients so difficult. The organism has an unusually large genetic make up with a total DNA content greater than 7 megabases and as many as three megabase-sized replicons 13. This large genetic make up accounts for its microbiological versatility.
Because of the high rate of cross-infection with B. cepacia and associated virulence it has become increasingly important to correctly identify the organism. It is accurate to say that a large CF centre is crucially dependent upon the quality of its microbiology service. B. cepacia can be difficult to isolate. There are established media and laboratory protocols for the culture and identification of B. cepacia 14. However, unequivocal identification of B. cepacia by commercial systems can present difficulties as existing selective media can support the growth of other gram-negative bacilli, such as Alcaligenes xylosoxidans, Stenotrophomonas maltophilia and Comamonas acidovorans. It is crucial that the laboratory uses established techniques and that the results are valid, reproducible and reliable. Inaccuracies, delay in microbiological diagnosis and the production of false positive and equally false negative results can have devastating clinical consequences. An unidentified B. cepacia positive patient will remain in the general CF clinic, continuing to pose a risk of cross-infection to other patients. A recently developed new selective medium has increased the level of identification of B. cepacia isolates 15. This naturally raises concerns that in a large CF clinic there may be unidentified B. cepacia colonisation of some patients.
Difficulties in accurately identifying B. cepacia and the realisation that there are different B. cepacia organisms (now known as the B. cepacia complex) has led to the development of molecular taxonomic analyses which place different B. cepacia strains into groups known as genomovars. Initially, Vandamme 16 used molecular techniques to analyse whole cell proteins and DNA-DNA hybridizations to separate isolates simply identified as B. cepacia into four new Burkholderia species. Currently, on the basis of identifying new strains of B. cepacia there are now seven genomovar groups. An excellent review of the different groups has recently been published 17. However, having separated the B. cepacia complex into genomovars, one has to ask whether this information is clinically useful. Does genomovar placement influence clinical practice. The main questions one asks when a patient becomes infected with B. cepacia is how virulent is the organism for that patient and is it transmissible to other patients? Currently that question is unanswered by genomovar status, but the most transmissible and virulent B. cepacia pathogens are placed in genomovar III. However transmissibility and virulence are not the same thing. Burkholderia gladioli, also a member of the Burkholderia species and supposedly nontransmissible, is difficult to separate from B. cepacia 18 and yet can cause gross thoracic and extra thoracic disease (fig. 3⇓). The B. cepacia strain responsible for the first described UK case of the “cepacia syndrome” in a young girl did not carry the cable pilus gene and did not transfer to her sibling 19. Basically, genomovar status is a useful template to categorise organisms that make up the B. cepacia complex. However, the most clinically damaging pathogens are increasingly grouped in genomovar III which does not necessarily translate into useful clinical information in the CF clinic.
Virulence and transmissibility
An enormous amount of research has been undertaken to define those virulence factors, expressed by B. cepacia, which interact with the host, and account for the greater morbidity and mortality associated with this pathogen. Amongst many laboratory defined virulence factors, endotoxin has been clearly shown to have a role in the pathogenesis of B. cepacia infection. Lipopolysaccharide from clinical isolates has endotoxin activity and the capacity to induce tumour necrosis factor-alpha (TNF-α) levels over nine times more than endotoxin extracted from Pseudomonas aeruginosa 20. This conforms to the evidence that CF infected B. cepacia patients, when compared with P. aeruginosa colonised patients, have an up-regulated inflammatory response when measuring plasma neutrophil elastase 21. Elegant microbiological studies in transgenic mice showed that nearly 70% of CF mice exposed to B. cepacia died from a more severe-bronchopulmonary infection than control animals 22. Nitric oxide (NO) and hydrogen peroxide are important bacteriocidal mediators in lung defence against B. cepacia 23. Inducible NO synthetase is deficient in the bronchial epithelium of CF patients. The lack of NO in the lungs of CF patients may contribute to their susceptibility to B. cepacia as a pulmonary pathogen.
One does not have to look very hard to observe that the clinical decline is overall greater for B. cepacia than P. aeruginosa infected patients. There is an accelerated decline in spirometry and nutritional status (the two main survival prognostic factors), with patients dying a decade earlier than their peers 24, 25. The organism can also cause prolonged temperatures and a terminal disease (“cepacia syndrome”), characterised by a confluent bronchopneumonia and septicaemia which can result in death over a period of days rather than months, and is unlike any clinical situation seen with P. aeruginosa. It would appear that CF patients therefore have either an exaggerated or defective response to infection with B. cepacia, which is much greater than those patients infected with P. aeruginosa. B. cepacia, when it infects non-CF patients, can produce severe disease. However, these patients are often clinically compromised and once their primary disease is treated they can eradicate B. cepacia.
Awareness of the increasing number of CF patients acquiring B. cepacia in CF clinics in North America led to the appreciation that the organism was cross infecting between patients 7, 8. More recent work has shown that transmissibilty is strain dependent and different typing systems have defined an epidemic strain with a strong transatlantic lineage 12, 26–28. This epidemic strain is identified by two markers, the cable pilus gene and a conserved 1.4kbp DNA fragment. There are other, well described transmissible strains of B. cepacia 29, but it is the epidemic strain known as ET (Edinburgh/Toronto) 12 which has caused the most concern, due to its apparently greater virulence. It has an almost total resistance to antibiotics and is strongly associated with the “cepacia syndrome”. This has been highlighted in a recent report when the epidemic ET12 strain was transmitted to five CF patients with other strains of B. cepacia 30. Four of the five CF patients cross-infected with the epidemic strain died, three from the lethal “cepacia syndrome”. It is now recommended practice to segregate CF patients in cepacia clinics by their strain pattern 31. In the Manchester Adult CF Unit, the incidence of B. cepacia increased with the emergence of the epidemic ET12 strain (fig. 4⇓). A policy of partial segregation failed, and it was not until a strict segregation policy was introduced that the annual incidence rate of B. cepacia fell. The introduction of this policy has further increased the feeling of isolation in CF patients infected with B. cepacia. Of concern, but not discussed in the literature is whether all cross- infecting strains of B. cepacia have been identified. In the Manchester adult CF unit there are approximately 20 patients who have a B. cepacia without an identifiable strain marker. Do they all harbour their own specific B. cepacia pathogen which does not pose a threat to other CF B. cepacia positive patients, or is it like the CF gene where new mutations are frequently being identified?
Clinical care of cystic fibrosis patients infected with Burkholderia cepacia
Care of CF patients is best delivered from a CF centre and is associated with better nutritional status and spirometry 32. However, there is a greater risk for cross-infection with B. cepacia at a CF centre. Despite the implementation of stringent segregation policies, it is unavoidable that CF patients will sometimes meet by chance, for instance in lifts, the hospital shop or inadvertently at outpatient appointments for different medical disciplines, such as obstetrics, gastroenterology and general surgery. B. cepacia positive CF patients should have the same clinical service as non-cepacia patients. As inpatients, they should have their own rooms, but on a separate ward. They should attend a specific cepacia outpatient clinic, with appointment times further designed to allow segregation by strain pattern.
Attention should be paid to nutrition. Intervention with nasogastric or gastrostomy feeding should be introduced early if there is difficulty in sustaining weight. Sustained temperatures (usually sputum load related) with an infective exacerbation are common and symptomatically distressing. Very high dose aspirin (1.5 g q.i.d.) is often useful until antibiotics reduce sputum load. However, sometimes temperatures are related to extensive pneumonic consolidation rather than B. cepacia sputum load. Antibiotic therapy needs to be extremely aggressive; triple antibiotic combinations are more likely than double antibiotic combinations to be bactericidal against B. cepacia 33. Intravenous septrin also has some benefit. Oral antibiotics can include combinations of ciprofloxacin, rifampicin, chloramphenicol and minocycline. There are, however, no clinical trials validating these regimes. Additionally there is concern about the unpredictable but common occurrence of antagonism (growth of an organism when a third antibiotic is added to a bactericidal combination of two antibiotics). The development of the cepacia syndrome (or “necrotizing cepacia”), characterised by a sustained temperature and confluent chest radiograph shadowing, signals a currently untreatable clinical situation. The Manchester Adult CF Unit has used immunomodulatory agents such as methylprednisolone, immunoglobulins and cyclosporin as part of the treatment regime for patients with cepacia syndrome; these have occasionally improved the situation, but only for a few days.
The most difficult clinical situation is planning transplantation for CF patients infected with B. cepacia 2, 34. In times of increasing organ donor shortage and reports of a 75% mortality rate in B. cepacia patients following transplantation there has been increasing reluctance to list these patients 3, 34. One option may be to list them earlier in a more stable state but it can be argued ethically (or legally) that every patient has the right to be considered for transplantation if there is some chance of benefit 35. Although there are reports of a high mortality rate for B. cepacia positive patients post-transplantation 3, 36, there are other studies which show benefit or no difference in survival terms for B. cepacia positive and B. cepacia negative patients 36, 37.
Infection with Burkholderia cepacia without cystic fibrosis
The pathogenicity of B. cepacia is not limited to individuals with CF. Another vulnerable group are patients with chronic granulomatous disease in whom infection with B. cepacia has been associated with a fatal outcome 38, 39. B. cepacia has been recognised as causing fatal disease in healthy individuals 40, 41. In hospitals, B. cepacia has been found to contaminate antiseptics, disinfectants, nebuliser solution, and dextrose solution 42–44. Contamination of a nebuliser solution resulted in patients becoming infected with B.cepacia and contamination of a dextrose infusion solution resulted in seven patients developing B. cepacia septicaemia. These reports over the last decade highlight the opportunistic nature of B. cepacia and its occasional ability to contaminate the hospital environment and infect immunocompromised and more rarely, healthy individuals.
However, of greater concern are two recent reports demonstrating cross-infection of epidemic B. cepacia from CF patients to non-CF individuals. The first case describes a mother developing severe bronchiectasis having been infected by her CF B. cepacia positive child 45. This case is extremely unusual but raises the concern, although small, that carers of CF patients are not entirely free from risk of cross-infection with virulent pathogens. Of considerable concern is a recent report describing cross-infection by a single dominant clone of B. cepacia between patients with and without cystic fibrosis 4. Isolates of B. cepacia were obtained from sputum (228), intravenous catheters (11), urine (10), wounds (10) and other miscellaneous sites (11) from 245 critically ill non-CF patients on intensive care units. In the same hospital 23 CF patients had isolates for B. cepacia. Although the hospital had isolation policies for B. cepacia positive CF individuals, this policy did not apply to B. cepacia positive non-CF patients who were in the same ward as other B. cepacia negative CF patients. CF patients with B. cepacia did not always follow the segregation rules. Thus B. cepacia cross-infected both ways between both groups of CF and non-CF patients. This report strongly supports a practice of segregating both CF and non-CF patients infected with B. cepacia. All these reports highlight the risk B. cepacia poses to all hospital patients and sometimes patients in the community.
Agricultural role of Burkholderia cepacia?
As detailed in this review, B. cepacia is a human pathogen. However, it is also a powerful pesticide and can eliminate many soil-borne plant pathogens 5. It also plays a potential role as a biofertiliser for rice cultivated in low acidic, low fertile soils. It is not surprising that patents are being sought by the agricultural lobby for different strains of B. cepacia which can be used to enhance crop yields. Furthermore, scientists are also exploiting the diverse metabolic properties of B. cepacia to develop it as an agent for use in the bioremediation of contaminated environmental sites. The potential economic and ecological benefits are considerable. Widespread use would however, increase human exposure. Recently, evidence of a clonal relationship between one strain of B. cepacia causing onion rot and another isolated from respiratory secretions of a CF patient has been obtained, suggesting the same clone can be present in both types of niche (environmental and human pathogen) 46. In addition, Burkholderia isolates have recently been cultured from rhizospheres in maize and wheat; taxonomic studies have identified these isolates as belonging in B. cepacia genomovar III. Although the virulence of environmental B. cepacia genomovar III isolates has yet to be determined, the most damaging B. cepacia human pathogens are all found in this particular genomovar group.
As stated earlier, B. cepacia has a large and complex genome. If B. cepacia strains were placed back deliberately into the environment there is the potential risk of horizontal gene transfer with, perhaps, the evolution of more virulent human pathogens. Recently insertion sequences within Burkholderia pseudomallei have been identified in B. cepacia, including an isolate belonging to the epidemic strain. It is currently impossible to identify strains of B. cepacia that can be used safely in agriculture, without causing a hazard to human health. This is clearly an area for conflict of interest between medicine and agriculture.
Conclusion
This review has concentrated on current areas of interest regarding Burkholderia cepacia. Interest in this area is highlighted by the increase in publications by physicians and scientists, with over 700 articles published in the last decade. Although the effect upon cystic fibrosis patients has been devastating, it has also damaged non-cystic fibrosis patients and is causing conflict between medicine and agriculture. This difficult and versatile pathogen is likely to continue to cause problems over the next decade.
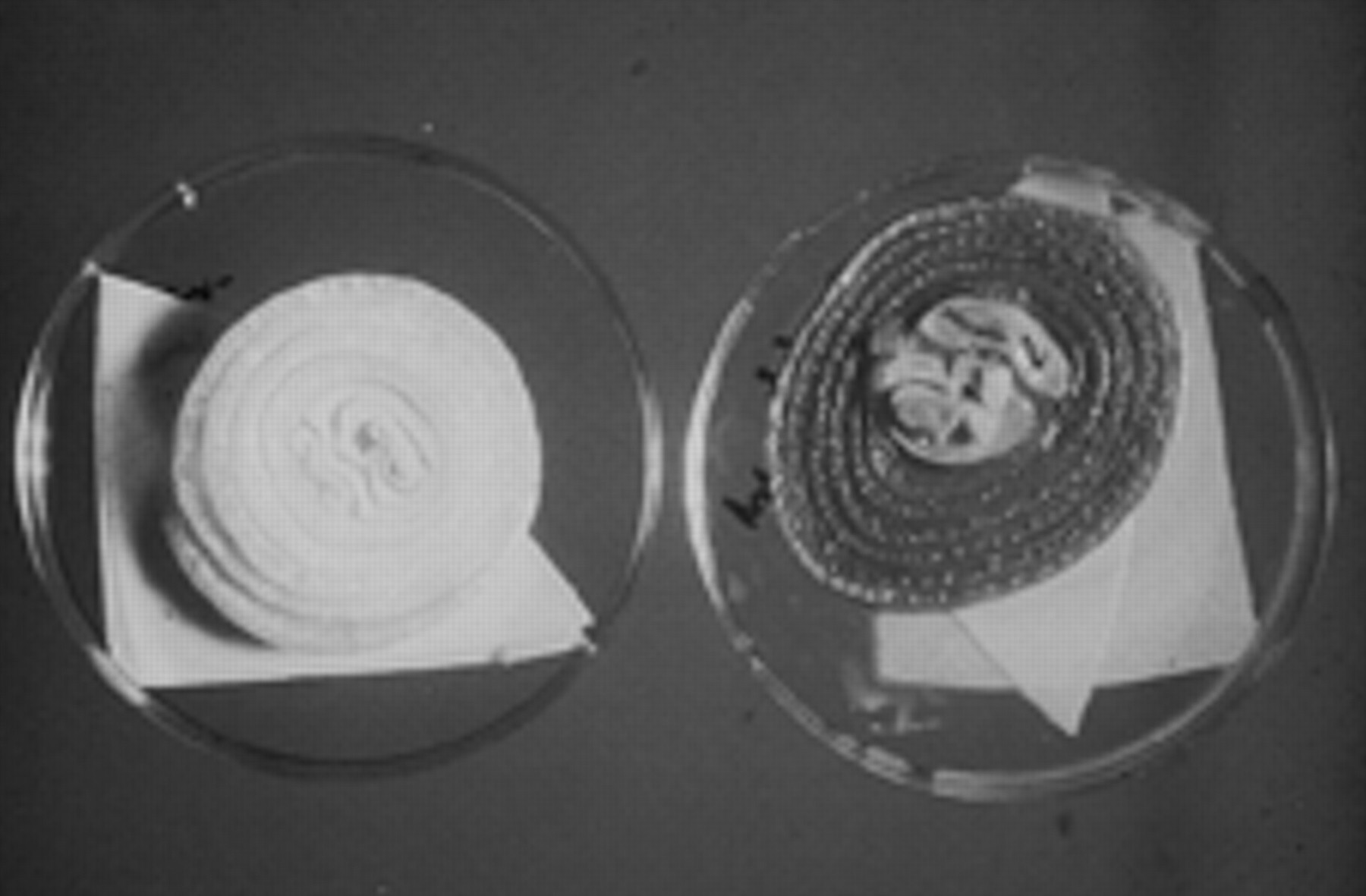
Two onions; the onoin on the right of the photograph has been inoculated with Burkholderia cepacia, causing onion rot.

Chest radiograph showing typical appearances of the cepacia syndrome.

Surgical incision and exploration of a Burkholderia gladioli leg abscess.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidence (new cases; □) and prevalence (total
cases;  ) for Burkholderia cepacia in the Manchester Adult
Cyctic Fibrosis (CF) Unit 1983–2000. From 1991–1992,
the ET12 epidemic strain was identified in B. cepacia isolates in
the Manchester unit and the incidence rate for B. cepacia increased.
A partial segregation policy for B. cepacia positive and B. cepacia negative CF patients was introduced in the unit in 1992, with a subsequent
fall in the incidence rate for 1993. However, the incidence rate increased
again in 1994, demonstrating failure of the policy of partial segregation.
It was following the introduction of a strict segregation policy for B. cepacia positive and B.cepacia negative CF patients in 1994
that the incidence rate for B. cepacia fell and has remained low.
The continuing fall in prevalence of B. cepacia on the Manchester
Unit is in relation to both a lower incidence rate and is also a reflection
of the virulence of the organism as a pathogen in the CF community, with decreased
survivla rates for CF patients colonised by B. cepacia.
) for Burkholderia cepacia in the Manchester Adult
Cyctic Fibrosis (CF) Unit 1983–2000. From 1991–1992,
the ET12 epidemic strain was identified in B. cepacia isolates in
the Manchester unit and the incidence rate for B. cepacia increased.
A partial segregation policy for B. cepacia positive and B. cepacia negative CF patients was introduced in the unit in 1992, with a subsequent
fall in the incidence rate for 1993. However, the incidence rate increased
again in 1994, demonstrating failure of the policy of partial segregation.
It was following the introduction of a strict segregation policy for B. cepacia positive and B.cepacia negative CF patients in 1994
that the incidence rate for B. cepacia fell and has remained low.
The continuing fall in prevalence of B. cepacia on the Manchester
Unit is in relation to both a lower incidence rate and is also a reflection
of the virulence of the organism as a pathogen in the CF community, with decreased
survivla rates for CF patients colonised by B. cepacia.
Footnotes
↵Previous articles in this series: No. 1: M.R. Hammerschlag. Chlamydia pneumoniae and the lung. Eur Respir J 2000; 16: 1001–1007. No. 2: S. Ewig, H. Scha«fer, A. Torres. Severity assessment in community acquired pneumonia. Eur Respir J 2000; 16: 1193–1201. No. 3: L.P. Nicod, J-C. Pache, N. Howarth. Fungal infections in transplant recipients. Eur Respir J 2001; 17: 133–140.
- Received April 5, 2000.
- Accepted April 27, 2000.
- © ERS Journals Ltd
References









