Article Text

Abstract
Background In chronic respiratory failure (CRF), body composition strongly predicts survival.
Methods A prospective randomised controlled trial was undertaken in malnourished patients with CRF to evaluate the effects of 3 months of home rehabilitation on body functioning and composition. 122 patients with CRF on long-term oxygen therapy and/or non-invasive ventilation (mean (SD) age 66 (10) years, 91 men) were included from eight respiratory units; 62 were assigned to home health education (controls) and 60 to multimodal nutritional rehabilitation combining health education, oral nutritional supplements, exercise and oral testosterone for 90 days. The primary endpoint was exercise tolerance assessed by the 6-min walking test (6MWT). Secondary endpoints were body composition, quality of life after 3 months and 15-month survival.
Results Mean (SD) baseline arterial oxygen tension was 7.7 (1.2) kPa, forced expiratory volume in 1 s 31 (13)% predicted, body mass index (BMI) 21.5 (3.9) kg/m2 and fat-free mass index (FFMI) 15.5 (2.4) kg/m2. The intervention had no significant effect on 6MWT. Improvements (treatment effect) were seen in BMI (+0.56 kg/m2, 95% CI 0.18 to 0.95, p=0.004), FFMI (+0.60 kg/m2, 95% CI 0.15 to 1.05, p=0.01), haemoglobin (+9.1 g/l, 95% CI 2.5 to 15.7, p=0.008), peak workload (+7.2 W, 95% CI 3.7 to 10.6, p<0.001), quadriceps isometric force (+28.3 N, 95% CI 7.2 to 49.3, p=0.009), endurance time (+5.9 min, 95% CI 3.1 to 8.8, p<0.001) and, in women, Chronic Respiratory Questionnaire (+16.5 units, 95% CI 5.3 to 27.7, p=0.006). In a multivariate Cox analysis, only rehabilitation in a per-protocol analysis predicted survival (HR 0.27, 95% CI 0.07 to 0.95, p=0.042).
Conclusions Multimodal nutritional rehabilitation aimed at improving body composition increased exercise tolerance, quality of life in women and survival in compliant patients, supporting its incorporation in the treatment of malnourished patients with CRF.
Clinical Trial number NCT00230984.
- Chronic obstructive pulmonary disease
- long-term oxygen therapy
- nutrition
- rehabilitation
- quality of life
- COPD pharmacology
Statistics from Altmetric.com
- Chronic obstructive pulmonary disease
- long-term oxygen therapy
- nutrition
- rehabilitation
- quality of life
- COPD pharmacology
Key messages
What is the key question?
In malnourished patients with chronic respiratory failure where body composition strongly predicts survival, would home multimodal nutritional rehabilitation improve clinical outcomes?
What is the bottom line?
Home rehabilitation combining health education, oral nutritional supplements, exercise and oral testosterone improved after 3 months, body composition, exercise tolerance and, in women, quality of life and was associated with a better survival 12 months after home intervention in compliant patients.
Why read on?
It appears that none of the components alone could achieve such results, supporting incorporation of multimodal nutritional home rehabilitation in undernourished patients with chronic respiratory failure.
Introduction
Chronic respiratory failure (CRF), the final common pathway of end-stage chronic respiratory diseases, is a common condition characterised by very poor survival. Indeed, the main cause of CRF—chronic obstructive pulmonary disease (COPD)—is predicted to become the fourth most common cause of death worldwide by 2030.1 The overall median survival of patients with CRF ranges from 2 to 6 years after the initiation of domiciliary respiratory assistance, depending on both the underlying respiratory disease and malnutrition. To date, only long-term oxygen therapy (LTOT) has been shown to improve survival.2 In CRF, body mass index (BMI) is an independent determinant of death.3 4 In COPD the predictive value for survival of fat-free and muscle mass has been reported.5 6 However, meta-analyses have failed to show any benefit from nutritional support alone.7 These data have led to recommendations combining education on health, exercise training and interventions to improve body composition abnormalities.8 Although positive results were achieved in moderate to severe COPD,9 10 nutritional support combined with pulmonary rehabilitation has not been studied in CRF. Our hypothesis was that improvement in body composition by a multimodal strategy combining anabolic stimuli such as exercise, oral nutritional supplements (ONS) and testosterone would improve clinical outcomes for malnourished patients with CRF. The main objective of this randomised controlled multicentre study was to increase BMI and fat-free mass index (FFMI) in order to achieve better exercise tolerance, quality of life and survival. Such an objective fits with present guidelines, although evidence is lacking in patients with home respiratory assistance.8
Methods
Patients
Eight clinics participating in respiratory home care networks took part in the study. Inclusion criteria included age >18 years; room air arterial oxygen tension (Pao2) ≤8 kPa at initiation of home treatment; LTOT and/or home mechanical ventilation history >3 months; BMI ≤21 kg/m2 or FFMI measured by 50 kHz bioelectrical impedance analysis (BIA) <25th percentile of predicted which corresponds to FFMI <18 kg/m2 in men and <15 kg/m2 in women11 12; absence of exacerbation within 3 months before inclusion; written informed consent. Four causes of CRF were considered: COPD, bronchiectasis, restrictive disorders and mixed respiratory failure.3 13 Exclusion criteria were pulmonary hypertension, obstructive sleep apnoea syndrome, neuromuscular diseases, cystic fibrosis, any condition compromising 6-month survival, serum alanine aminotransferase (ALAT) >1.5 ULN, hormone-dependent cancer, elevated prostate-specific antigen (PSA), inability to follow a rehabilitation programme and women of childbearing age.
Experimental design
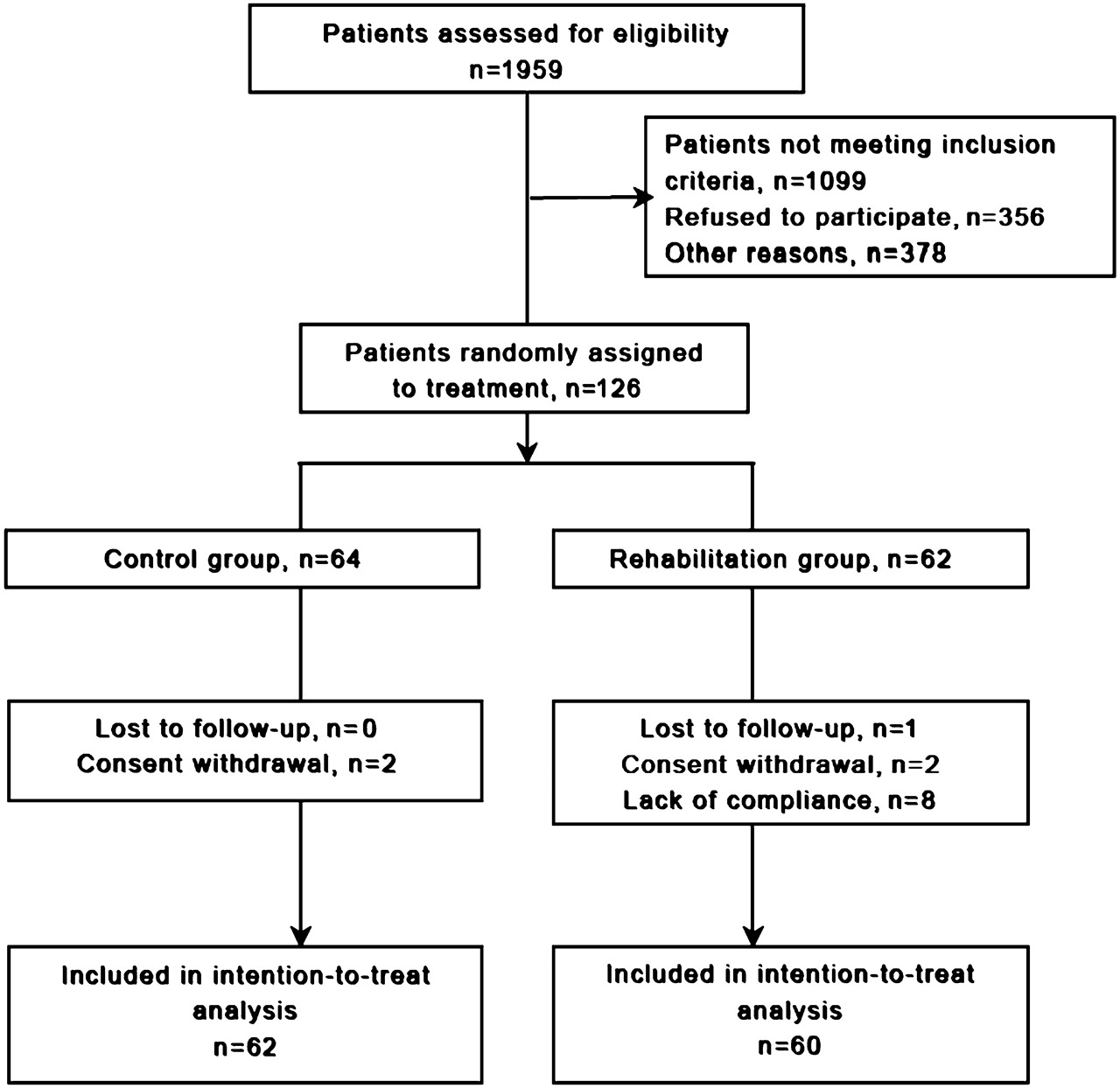
From March 2003 to March 2007, 1959 Caucasian patients were screened and 126 were randomly assigned to the home nutritional rehabilitation group (n=62) or to the control group (n=64) (figure 1). Most of the failures for inclusion were due to body composition inclusion criteria. Two patients in each group withdrew their consent. Thus, 31 women and 91 men of mean (SD) age 65.9 (9.6) years were included. Randomisation was stratified by centre and used balanced blocks of 4 or 6. The assignment of a new patient was obtained by contacting a central office where sealed numbered envelopes for each centre were secured.

Enrolment of patients and completion of study. The four patients who withdrew their consent (two in each group) were not analysed. The eight patients from the rehabilitation group who did not comply, as well as the one lost to follow-up, were retained in the intention-to-treat analysis.
Intervention
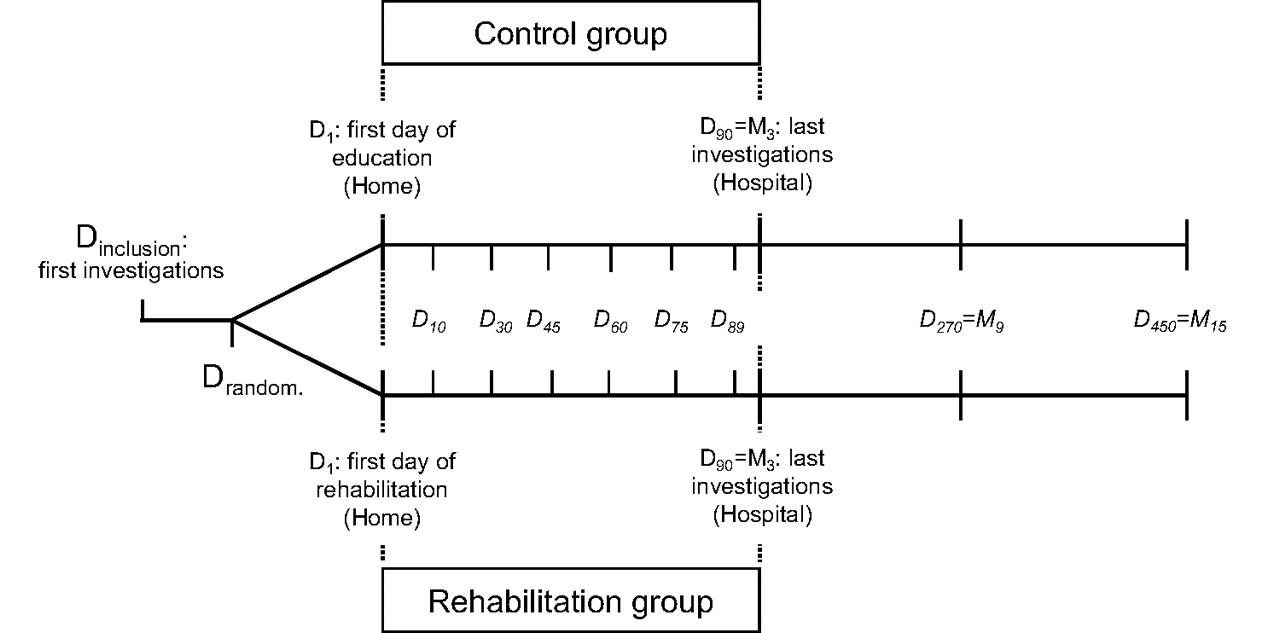
The trial interventions were performed in the patients' homes from day 0 to day 90 (figure 2). In all patients education was delivered by nurses or physiotherapists specialised in pulmonary rehabilitation during seven 2-h sessions on days 0, 10, 30, 45, 60, 75 and 89 using specific booklets (http://www.livingwellwithcopd.com). Staff members received instructions during two meetings prior to first randomisations in order to get homogenous education and training interventions in terms of content and timing. In addition, the multimodal nutritional rehabilitation group received oral testosterone undecanoate, 80 mg twice daily in men and 40 mg twice daily in women (Schering-Plough, Kenilworth, New Jersey, USA), three 120 ml ONS per day (188 kcal, protein 20%, carbohydrates 60% and lipids 20%; Respifor, Nutricia Advanced Medical Nutrition, The Netherlands),14 15 exercise training combining endurance sessions on a bicycle 3−5 times a week, started at 50% of the peak workload achieved on day 0 then increasing by 5 W increments, and segmental muscular reinforcement exercises using elastic bands. Exercise sessions three times a week were unsupervised except during the seven visits by the person responsible for education. Telephone calls once a week encouraged patients to perform exercise sessions. ONS and androgen pills were given during each fortnightly visit and both stopped on day 90. During the last visit all patients were encouraged to keep an active way of life and to combat undernutrition but no further home intervention was planned except two calls 6 months apart to get updates on health status.

Experimental design of the study. Inclusion day, randomisation day and first day of intervention were as close as possible. The intervention period lasted from day 1 to day 90, with the same evaluation on the inclusion day and day 90. Health-related events were recorded on day 270 and day 450.
Patient assessment
On the day of inclusion clinical examination, blood sampling, BIA, ECG at rest, arterial blood gases, pulmonary function tests, maximal cycle exercise capacity, specific quality of life questionnaires, 6 min walking test (6MWT), isometric quadriceps force and exercise endurance testing were performed (figure 2). During the seven home visits the safety and efficacy of exercise sessions were determined together with compliance with exercise assessed by exercise tests prior to inclusion and a written patient report of each session to assess their self-perceived tolerance of home exercise, ONS by empty can collection and androgen therapy by empty blisters. Patients in the rehabilitation group were considered as compliant if they had received at least one-third of two of the three interventions planned—that is, at least 12 exercise sessions out of 36 and/or 90 ONS out of 270 and/or 160 androgen pills out of 480 in men or 80 of 240 in women.
On day 90 the evaluation performed on the inclusion day was repeated with the investigator blind to the allocation arm. On days 270 and 450, health-related events (home-treated exacerbations, hospitalisation days, death) were recorded.
Measures
At baseline, demographic data, smoking habits, use of inhaled corticosteroids, long-acting β2 agonists and anticholinergics, oral β-blockers and statins were recorded. Serum ALAT and PSA were measured at inclusion and on day 90.
Respiratory function
Forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and arterial blood gases were measured in room air at rest.
Exercise tolerance
A 6MWT was performed according to ATS guidelines under oxygen therapy set at the same flow on days 0 and 90 and expressed as the absolute value and percentage of predicted value.16 An incremental maximal exercise test was performed on an electromagnetically-braked cycle ergometer with the patient on oxygen therapy. Exercise endurance time was measured at 55% of peak work capacity to mimic the energy needed to perform daily physical activities.
Maximum isometric quadriceps force
The maximum isometric quadriceps force was measured on the dominant leg in the sitting position using the Globus system (Globus Sport and Health Technologies LLC, West Hartford, Connecticut, USA).
Nutritional and endocrine parameters
Body composition was assessed by 50 kHz BIA according to Kyle.11 12 FFM was normalised for height (FFMI=FFM/height2). Serum albumin, transthyretin, C reactive protein and haemoglobin measurements were centralised and performed using conventional methods. Total testosterone was measured by radioimmunoassay (RIA) after extraction and chromatography, oestradiol by RIA after extraction, and luteinising hormone (LH) and follicle-stimulating hormone (FSH) by immunoradiometric assay (IRMA; Beckman Coulter, Fullerton, California, USA). Sex hormone-binding globulin (SHBG) was measured by IRMA (Cis Bio International, Saclay, France). Bioavailable testosterone was calculated taking into account total testosterone, albumin and SHBG levels.17
Statistical analysis
The sample size was estimated for an increase in 6MWT by 50 m with an SD of 100 m, a two-sided α error of 0.05 and a β error of 0.20.13 Two blinded interim analyses of 6MWT, serious adverse events and death from any cause were planned (January 2006 and 2007) to look for premature evidence of benefits in the rehabilitation versus control group, or of harm in any group. The Peto method was used with a significance level of 0.001 for each interim study to keep a final significance level of 0.05. Normality was assessed by the Shapiro–Wilk test when necessary. The primary analysis was performed according to the intention-to-treat principle. The treatment effect was calculated by between-group comparisons of the 3-month variation in parameters with regression analysis adjusted for sex, age and baseline value of the parameter, except for hormonal data and quality of life for which men and women were studied separately. Serious adverse event rates (number of events or days in hospital divided by follow-up duration) were compared between groups with the Mann–Whitney test. Survival at the end of follow-up was analysed using Kaplan–Meier curves and log-rank tests. After verification of the proportional hazards assumption, univariate Cox proportional hazard models were built to detect indicative parameters at a level of p=0.20; these were then tested to propose a multivariate Cox model. Finally, a per protocol survival analysis comparing the treated and control group was performed: patients in the rehabilitation group were analysed if they had been compliant during the 3-month intervention. This was the sole subgroup analysis performed to assess the role of minimum compliance to reach survival benefit. Statistical tests were carried out using Stata 10 (Stata Corp., College Station, Texas, USA).
Results
Baseline data
At baseline, patient characteristics (table 1) and treatments (data not shown) were similar in the two groups. Patients were mainly male ex-smokers with COPD. They presented with a severe ventilatory obstructive defect, profound hypoxaemia and moderate hypercapnia, leading to non-invasive mechanical ventilation in 35% of cases. Exercise intolerance was demonstrated by low values for 6-min walking distance (6-MWD) and peak workload. The median BMI was 21.0 kg/m2. At inclusion, FFMI in men was <18 kg/m2 in 88% of cases and in women <15 kg/m2 in 90% of cases. Serum albumin was <35 g/l in 21% of patients, transthyretin <200 mg/l in 34% and serum C reactive protein ≥5 mg/l in 61%. In men, 32% had a total testosterone level below the normal range, 51% had an increased SHBG level and 70% had decreased bioavailable testosterone. In women, 90% had elevated FSH and low oestradiol levels in line with postmenopausal status. Quality of life questionnaires showed similar values in men and women.
Baseline values in the control and multimodal nutritional rehabilitation groups
Changes in biological and clinical parameters from day 0 to day 90
The clinical and biological results are summarised in table 2. The therapeutic effects of multimodal nutritional rehabilitation on functional and nutritional parameters (table 2) comprised improvements in peak workload, quadriceps isometric force and endurance time on a bicycle, whereas the increase in 6MWD was not statistically or clinically significant. BMI, FFMI, serum transthyretin and haemoglobin increased significantly. Quality of life was improved in women but not in men. In men, testosterone therapy induced a decrease in LH, FSH and oestradiol levels (−1.5 ng/l, p=0.013; −2.4 ng/l, p=0.010; −3.8 ng/l, p=0.012, respectively). In both men and women, SHBG levels decreased in the rehabilitation group compared with controls (−12.4 ng/l, p<0.001 and −37.7 ng/l, p<0.001, respectively). In rehabilitated women but not in men, total and bioavailable testosterone levels increased. Pulmonary volumes and blood gases were unaffected.
Mean (SD) within-group differences in absolute and percentage changes from baseline for outcome variables after 3 months of multimodal nutritional rehabilitation and mean (SEM) between-group differences adjusted for sex, age and parameter value at baseline
Eight patients including three women in the rehabilitation group were non-compliant, achieving only 12.3% of exercise sessions (range 0–22.2) and taking only 11.9% (0–23.3%) of the ONS and 22.0% (0–46.7%) of the androgen tablets in women and 7.8% (0–82.0%) in men. These patients were similar to compliant patients at baseline except for BMI (mean (SD) 24.1 (0.8) vs 21.1 (0.5) in compliant patients, p=0.039). Safety-related parameters such as C reactive protein, ALAT, PSA, arterial pH and Paco2 were unaffected. The 3-month exacerbation rates were slightly higher in the rehabilitation group than in controls (0.36 (range 0–3.33) vs 0.14 (0–2.22), p=0.045) but did not influence the hospitalisation rates for respiratory illness (4.0 (0–57) vs 2.7 (0–60) days, p=0.073) or non-respiratory events (0.3 (0–8.9) vs 2.0 (0–49) days, p=0.21).
Day 90 to day 450 follow-up
The exacerbation rate (0.18 (range 0–1.11) vs 0.16 (0–1.39), p=0.61) as well as hospitalisation rates for respiratory (3.1 (0–28.6) vs 2.3 (0–17.0) days, p=0.67) and non-respiratory (1.5 (0–73) vs 0.3 (0–12.8) days, p=0.90) events were similar in the two groups. Six of the 60 patients assigned to rehabilitation and 12 of the 62 controls died (figure 3, intention-to-treat analysis, p=0.15). Respiratory failure was the cause of death in two rehabilitated and seven control patients.

{kind=link}
{kind=link}
{kind=link}
Intention-to-treat (upper) and per-protocol (lower) analyses of survival. In the intention-to-treat analysis all 60 patients in the rehabilitation group were studied. In the per-protocol analysis the 52 compliant patients were retained. Compliance was defined as having received at least 30% of two of the three treatments (exercise, oral nutritional supplements and oral testosterone undecanoate) during the 3-month intervention.
After exclusion of non-compliant patients, only three deaths were reported among the 52 rehabilitated patients. Thus, in per protocol analysis, survival was significantly improved in rehabilitated patients compared with controls (log-rank test, p=0.03). In all patients univariate Cox analysis showed that 15-month survival was related to age (p=0.053), baseline values of FFMI (p=0.054), albumin (p=0.137), Pao2 (p=0.039), 6MWD (p=0.011), peak workload (p=0.094), exercise endurance time (p=0.025) and belonging to the rehabilitation group (p=0.163). In per-protocol multivariate univariate Cox regression and per protocol analysis (table 3), after verification of the proportional hazards assumption, baseline values of FFMI, FEV1/FVC, albumin, Pao2, 6MWD, peak workload, exercise endurance and belonging to the rehabilitation group had a p value of <0.20 and were tested in backward multivariable models adjusted for gender and age. In the final model adjusted for gender, age and baseline endurance time, belonging to the rehabilitation group appeared to be the only independent predictor of survival (HR 0.287, 95% CI 0.08 to 0.95, p=0.042).
Per-protocol univariate and multivariate analyses of survival with Cox proportional hazards regression models
Discussion
This is the first study to confirm the working hypothesis that improving body mass and composition significantly improves muscle function and quality of life in malnourished patients with CRF. Three-month multimodal nutritional rehabilitation resulted in increased BMI and FFMI together with serum transthyretin and haemoglobin. These nutritional improvements were associated with better muscle functioning, quality of life and 15-month survival in per protocol analysis, but we failed to reach our primary outcome of a clinically significant increase in 6MWT.
In COPD, little benefit can be expected from nutritional supplements given alone except in a recent randomised control trial based on dietary counselling and food fortification resulting in a sustained weight gain and improved quality of life.7 20 In CRF, no data on nutritional interventions are available. In this context, American Thoracic Society/European Respiratory Society guidelines propose a multimodal approach to address the systemic dimension of chronic respiratory diseases.8 A few pioneer groups have shown the potential of combining either exercise plus androgens21 22 or exercise plus nutritional supplements.3 10 23 This study showed significant improvement in clinical outcomes by combining ONS, androgen therapy and exercise in CRF. It also confirmed the efficacy and safety of home-based intervention.24
The doses of testosterone used were those recommended for physiological substitution in cases of acquired hypogonadism. The rationale for the choice of nutritional supplements was the presentation in low-volume and high-calorie packs which has been reported to increase patient compliance,14 and the high carbohydrate/fat ratio which has been demonstrated to be preferable in hypoxic conditions resulting in less dyspnoea in patients with COPD at rest and during exercise.15
At baseline, patients exhibited features of a poor prognosis as indicated by low BMI,3 4 25 FFMI,5 6 serum albumin and transthyretin, systemic inflammation,3 very severe obstructive airflow pattern, chronic hypoxia and carbon dioxide retention.2–4 After rehabilitation body weight increased by 1.5 kg, in contrast with the known risk of weight loss in rehabilitation without an increase in energy intake. Such an improvement in body mass, mainly related to an increase in FFM (+1.73 kg), resulted in an improvement in peak workload which compared favourably with data obtained in emphysematous patients undergoing surgical volume reduction.26 The improvement in both FFM and exercise tolerance, which has not previously been reported with nutritional intervention alone, is probably related to the combination of three anabolic stimuli. In contrast to the results of the National Emphysema Therapy Trial study, the increase in 6MWD was not significant in our series. It is known that 6MWD is more demanding in terms of oxygen requirements than the bicycle submaximal endurance test. The discrepancy between the two studies can be explained by the ability of surgery—but not rehabilitation—to correct the severe mechanical disadvantage due to static and dynamic hyperinflation in patients in GOLD stage IV included in our study. Data from these two studies reinforce the benefit of intervening at both the systemic and pulmonary levels.8
As previously reported, 70% of men presented with low bioavailable testosterone.27 Oral testosterone undecanoate is known to induce a transient increase in plasma testosterone and then a decrease in plasma FSH and LH.28 Concordantly, morning total and bioavailable testosterone levels were unaffected by the treatment. Conversely, in postmenopausal women with very low endogenous testosterone production, hormonal treatment resulted in higher testosterone levels.
The observed improvement in quality of life can be explained by the increase in peak workload, muscle performance, nutritional status20 and haemoglobin levels. Nevertheless, the improvement in quality of life was only significant in women. This gender effect was independent of respiratory deficiency, nutritional status or compliance with therapies (data not shown). This may be explained by a stronger effect of hormonal treatment in women.
Multimodal nutritional rehabilitation resulted in a slight increase in exacerbation rate during the 3-month intervention period but not in the follow-up period, similar to the Intercom study.10 This increase in the reported exacerbation rate during rehabilitation may be explained by improved detection.
In the per protocol analysis but not in the intention-to-treat analysis, 15-month survival was improved by multimodal nutritional rehabilitation. In very severe COPD the medical options shown to modify survival are limited to LTOT.2 Neither inhaled corticosteroids and long-acting β2 agonists nor long-acting parasympathicolytic bronchodilators have shown a significant advantage.29 30 Surgical lung volume reduction can offer survival benefits but only to highly selected patients with heterogeneous emphysema.26 In the present study, multivariate Cox analysis confirmed the impact of nutritional rehabilitation on survival. Taken together, these data strongly suggest that multimodal nutritional rehabilitation is able to improve body composition and to confer survival benefit.
One limitation of this study is that the experimental design did not allow us to define the specific effect of each component of rehabilitation. Indeed, chronic diseases including chronic respiratory diseases share a common phenotype characterised by a high prevalence of anorexia, inactivity, inflammation, oxidative stress, insulin resistance and hypogonadism resulting in sarcopenia.31 No study of an integrated approach to muscle wasting is available in malnourished patients with CRF. In patients with COPD isolated interventions such as nutritional support or exercise training are unable to improve exercise tolerance and body composition or survival. There is a growing body of evidence showing the potential of combining nutritional and exercise training in COPD,9 10 23 32 even though data are lacking in end-stage disease.32 The present study, conducted in patients with more advanced COPD, does not make it possible to analyse the specific effect of associating male hormone supplementation with such a management strategy. Because of the additive effects of exercise and nutritional support, on the one hand, and of exercise and androgens on the other, it appeared to be of interest to combine nutritional support, exercise and an anabolic hormone in order to achieve an improvement in muscle mass and function.33 Previous reports on the use of testosterone therapy in selected patients with COPD of mean age 63–67 years and without cardiovascular disease, as in this study, did not mention significant adverse effects.21–23 Cardiovascular events associated with testosterone intervention were reported in a study by Basaria et al of 209 men with a mean age of 74 years and a high prevalence of hypertension, diabetes, hyperlipidaemia and obesity.34 The patients in our series were younger (mean age 65 years), undernourished and without cardiovascular abnormalities at incremental maximal exercise testing. Moreover, changes in serum testosterone during treatment were much more pronounced in the study by Basaria et al. Taken together, these data in disabled patients with COPD suggest that replacement doses of androgens can be safely administered in carefully selected and monitored patients.
In conclusion, in malnourished patients with CRF a 3-month home intervention aimed at increasing FFMI resulted in clear benefits in terms of body composition, exercise tolerance and, in women, of quality of life at 3 months. Moreover, per-protocol analysis showed that survival measured 1 year after completion of the intervention was significantly improved. Such a multimodal approach appears to be a new therapeutic option capable of reducing mortality in patients with CRF in the community. Although its effect on survival needs to be confirmed in larger series with a longer follow-up period, the results obtained in the present study support the incorporation of multimodal nutritional rehabilitation in the long-term management of malnourished patients with CRF.
Acknowledgments
The authors thank Charles Auffray for insightful discussions and Erwan Floch, Alastair Forbes and Daniel Veale for English corrections.
References
Footnotes
See Editorial, p 935
CMP and NJC contributed equally to this study.
↵* IRAD2 Investigators (1) Grenoble, France: CHU Michallon (C Pison, B Wuyam, E Maclet, I Vivodtzev, R Guzun), Inserm Grenoble Centre d'Investigation Clinique 03 (D Abry, N Henquin, JL Cracowski), AGIR à Dom (F Putod, JC Borel, AS Michallet); (2) Poitiers, France: CHU, Hôpital de La Milétrie (F Caron, JC Meurice, ML Adoun, J Augustin); (3) Saint-Etienne, France: CHU Nord (I. Court-Fortune, F Costes, B Januel, M Charles); (4) Limoges, France: CHU du Cluzeau-Dupuytren (B Melloni, MT Antonini, JC Desport, JM Ribardière, F Dalmay), ALAIR-AVD (P Samptiaux, V Arnold, P Dzugan, E Marchaisseau), Centre MGEN Ste Feyre (S Jeandeau, H Triki); (5) Montpellier, France: CHU Arnaud de Villeneuve (L Meziane, M Hayot, P Godard, C Préfaut); (6) Paris, France: CHU La Pitié Salpêtrière (J. Gonzalez-Bermejo, T Similowski, C Straus, E Dalmolin, E Cornu); (7) Rouen, France: CHU Bois Guillaume (LC Molano, C Tardif, A Cuvelier, JF Muir), ADIR (J Dupuis); (8) Genève, Switzerland: Hôpitaux Universitaires de Genève (C Pichard, JP Janssens). Centralised biological analysis centre: Lyon, France: Hôpital E Herriot (H Lejeune, C Lombard, B Claustrat, F Touraine).
Funding The study was investigator driven. Funds came from academic sources (Programme Hospitalier de Recherche Clinique National, Direction Interrégionale de la Recherche Clinique Rhône-Alpes Auvergne), public foundations (Nutrition 2000Plus), associations (Association Nationale pour les Traitements à Domicile, les Innovations et la Recherche-ANTADIR, AGIRàDom) and pharmaceutical sources (Nutricia Advanced Medical Nutrition, The Netherlands, France; Organon-Schering-Plough, Kenilworth, NJ, USA). The sponsors did not place any restrictions on the academic authors regarding the design and interpretation of the study, or statements made in the final manuscript.
Competing interests CP received financial support as research grants and consulting fees from Abbott, Baxter, B Braun, Cosmed, Fresenius-Kabi, Nestle, Novartis, Nutricia-Numico, Pfizer, Solvay; CMP and NJC from Nutricia Danone for honoraria and travel grants.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Comité consultatif de protection des personnes se prêtant aux recherches biomédicales de Grenoble.
Provenance and peer review Not commissioned; externally peer reviewed.