Article Text

Abstract
Background: Non-tuberculous mycobacterial lung disease, most commonly caused by Mycobacterium avium infection, tends to show variable disease progression, and significant disease predictors have not been adequately established.
Methods: Variable numbers of tandem repeats (VNTR) were evaluated in 16 mycobacterial interspersed repetitive unit (MIRU) loci from M avium isolates cultured from respiratory specimens obtained from 2005 to 2007. Specifically, the association between VNTR profiles and disease progression was assessed.
Results: Among the 37 subjects who provided positive respiratory cultures for M avium during the 2005–6 period, 15 subjects were treated within 10 months following a microbiological diagnosis of progressive M avium lung disease. Nine subjects underwent long-term follow-up (>24 months) without treatment for stable M avium lung disease. Based on a neighbour-joining cluster analysis used to classify M avium-positive subjects according to the VNTR profile, subjects with progressive versus stable lung disease were found to be grouped together in distinct clusters. Further analysis using logistic regression modelling showed that disease progression was significantly associated with the genetic distance of the M avium isolate from an appropriately selected reference (age-adjusted odds ratio 1.95; 95% confidence interval 1.16 to 3.30; p = 0.01 for the most significant model). A best-fit model could be used to predict the progression of M avium lung disease when subjects from the 2005–6 period were combined with those from 2007 (p = 0.003).
Conclusion: Progressive lung disease due to M avium infection is associated with specific VNTR genotypes of M avium.
Statistics from Altmetric.com
Non-tuberculous mycobacterial (NTM) lung disease is a common chronic pulmonary pathology. NTM has attracted clinical attention owing to increases in its incidence over the past several decades in non-susceptible populations. Specifically, NTM is predominantly observed in postmenopausal women and in susceptible populations such as patients with AIDS or cystic fibrosis.1 2 3 Among the NTM species most often encountered in clinical settings, Mycobacterium avium is the most frequent and significant cause of pulmonary NTM infection.2 3 4 M avium is common in many environments including water and soil, and the diagnosis of M avium lung disease is based on clinical presentation (radiographic appearance and microbiological features).3 5
Even after a diagnosis of M avium lung disease has been established, important and unresolved questions remain regarding treatment. These questions include whether the patient requires immediate treatment with macrolide-containing multidrug therapy or whether the start of treatment can be delayed.1 2 3 While immediate therapy is recommended for fibrocavitary M avium lung disease owing to progressive lung destruction, a more prevalent form of M avium lung disease termed “nodular bronchiectatic disease” tends to show variable disease progression. For example, one patient may show indolent stable lung disease such that a potentially toxic and expensive therapy is withheld, while another patient may display a more progressive disease that warrants immediate treatment.3 6 7 8 However, there are currently no established predictors for disease progression. As a result, close pre-therapeutic follow-up may be necessary to distinguish between progressive and stable M avium lung disease.3 8
The present study evaluates whether molecular typing of M avium isolates is informative for predicting the progression of M avium lung disease. Specifically, we investigated variable numbers of tandem repeats (VNTR) in 16 mycobacterial interspersed repetitive unit (MIRU) loci in M avium clinical isolates. Our data demonstrate that specific VNTR profiles are related to the likelihood of M avium lung disease progression, thus allowing us to predict disease progression by examining the genetic divergence of M avium isolates.
Methods
Study population
The study included 37 subjects who had visited the Pulmonary Medicine Clinic of the Tohoku University Hospital, a referral hospital in Sendai, between January 2005 and December 2006. Patients who had provided respiratory cultures positive for M avium were chosen for the study. Respiratory specimens yielding positive cultures included expectorated sputum samples and bronchial washes of bronchoscopic samples. Subjects who were culture-positive for M avium were classified as having M avium lung disease based on clinical diagnostic criteria, including pulmonary symptoms and radiographic findings. Otherwise, the culture-positive subjects were classified as not having M avium lung disease. “False” positive samples may have been the result of transient infection or environmental contamination of the respiratory specimens.3 To validate the logistic regression model, we also evaluated eight subjects with lung disease that yielded positive cultures for M avium during 2007.
The clinical and microbiological factors responsible for the progression of M avium pulmonary infection were also examined. Disease progress was determined by observing patients with M avium lung disease until the start of antimycobacterial treatment (after the culture-proven diagnosis). During the observation period the patients were evaluated at least several times a year for exacerbation of pulmonary symptoms, chest radiograph features and microbiological findings. Specifically, we determined whether the condition was progressive (treatment required within 12 months of diagnosis) or stable (treatment delayed until after 12 months). Data were excluded from all analyses if unrelated death occurred during the observation period. A patient with M avium-associated hypersensitivity-like lung disease (ie, “hot tub lung”) was also excluded owing to the unique clinical features of both lung inflammation and infection.2 3 9
Mycobacterial genotyping
M avium isolates were grown on Middlebrook 7H10 agar with OADC enrichment (BD Diagnostics, Sparks, Maryland, USA) for 3–4 weeks at 37°C under 5% CO2. The mycobacterial mass was placed in a microcentrifuge tube containing 200 μl InstaGene matrix (Bio-Rad Laboratories, Hercules, California, USA) and DNA was extracted according to the manufacturer’s instructions. Using the DNA template (2 μl) and Taq DNA polymerase (1.25 U, Takara Shuzo, Kyoto, Japan), 16 MIRU loci were amplified in a total volume of 25 μl with primers specific for sequences flanking each locus (1 μM of each primer, see table S1 in the online supplement).10 11 12 13 14 15 16 The amplification profile consisted of 5 min at 95°C followed by 36 cycles of 10 s at 98°C, 30 s at 68°C and 1 min at 72°C. The polymerase chain reaction (PCR) products (5 μl) were run on a 2.5% agarose gel and stained with 0.5 μg/ml ethidium bromide. The size of each amplicon was estimated using the ChemiDoc XRS system (Bio-Rad Laboratories). The number of repeat units was determined in 16 MIRU loci (ie, the VNTR profile) for each M avium isolate.
Clustering analysis
The diversity of VNTR profiles between each set of M avium clinical isolates was assessed using the Manhattan distance. The Manhattan distance between M avium isolates Ma-x and Ma-y was calculated using the following formula:

where xn and yn are the number of repeat units in the nth MIRU locus, MATR-n. The genotypic diversity of M avium isolates was analysed using a neighbour-joining algorithm in the PHYLIP software (Version 3.67) for clustering.17 18 Branch support was determined using the bootstrap method with 1000 replicates of a randomly resampled data set. The graphic phylogenetic distribution was drawn using the NJplot software for MS Windows.19
Statistical analysis
Comparisons of clinical characteristics between study groups were performed using the Fisher exact test for categorical variables and the unpaired Student t test for continuous variables. The Manhattan distance of M avium isolates from a reference point was compared between patients with progressive disease and those with stable disease by logistic regression analysis. The results of all models are reported as age-adjusted odds ratios (ORs) with 95% confidence intervals (CI). The probability of disease progression was calculated using the logistic regression model with M avium isolate Ma-31 as the reference. The two study groups were examined using Mann-Whitney non-parametric comparison tests; p values of <0.05 were considered to be statistically significant. All analyses were performed using StatView software Version 5.0 (SAS Institute, Cary, North Carolina, USA).
Results
Characterisation of subjects
Based on sputum specimens or bronchial washes, a total of 37 M avium-positive subjects were identified from 2005–6. Data regarding demographic information, clinical types of M avium lung disease, pretreatment observation period, culture-negative period after initiating treatment and the medical history of each subject are presented in table 1 and summarised in table 2. Of the 37 subjects whose respiratory cultures were positive for M avium, 11 showed no radiographic findings (including chest CT scans) for M avium lung disease. These 11 subjects were therefore excluded from the study. The remaining 26 subjects met the clinical criteria for a diagnosis of M avium lung disease including fibrocavitary lung disease (three subjects), nodular bronchiectatic lung disease (22 subjects) and hypersensitivity-like lung disease (one subject). The proportion of patients with a medical history of pulmonary disease was higher in the group without M avium lung disease than the group with M avium lung disease. In contrast, the two groups did not differ with respect to age at positive culture or the proportion of men and women (lung disease vs no lung disease: age, p = 0.20; sex, p = 0.06; medical history, p<0.001; table 2).
Subjects with positive respiratory cultures for Mycobacterium avium
Demographic and clinical characteristics of subjects
In patients with M avium lung disease, 15 subjects were treated within 10 months of microbiological diagnosis owing to the progression of M avium lung disease and treatment was withheld for more than 24 months in nine subjects owing to stable M avium lung disease. Two subjects with M avium lung disease were excluded from the analyses owing to censored observation or unique clinical manifestations such as hypersensitivity-like lung disease. Demographic and clinical variables were similar in M avium-infected patients with progressive or stable lung disease (progressive disease vs stable disease: age, p = 0.44; sex, p = 0.12; clinical feature, p = 0.27; medical history, p = 0.99; table 2).
Genotyping and clustering analysis of M avium isolates
To assess the association between mycobacterial genotype and disease progression, we determined the VNTR profiles of each M avium isolate by evaluating the numbers of repeat units in 16 MIRU loci (fig 1A). The VNTR profiling data for 40 M avium isolates were obtained from 37 subjects; subjects 2, 13 and 22 provided respiratory specimens containing two M avium isolates with distinct VNTR profiles: Ma-2a/-2b, Ma-13a/-13b and Ma-22a/-22b, respectively (fig 1B).

Variable numbers of tandem repeats (VNTR) profiling of Mycobacterium avium clinical isolates. (A) A representative result of the VNTR profile of M avium. The genomic DNA of M avium isolated from subject 3 was amplified with primers for 16 MIRU loci (MATR-1 to MATR-16) using PCR. The PCR products were resolved on a 2.5% agarose gel with a size marker and stained with ethidium bromide. From the estimated size of the PCR product, the number of repeat units was calculated. (B) VNTR profiles of 40 clinical isolates of M avium. The numbers of tandem repeat units at 16 MIRU loci are shown for each M avium isolate. Two different M avium isolates, based on the VNTR profiles, were cultured from respiratory samples collected from subjects 2, 13 and 22 and are referred to as Ma-2a/-2b, Ma-13a/-13b and Ma-22a/-22b, respectively. Boxes of the same colour represent the same number of tandem repeats.
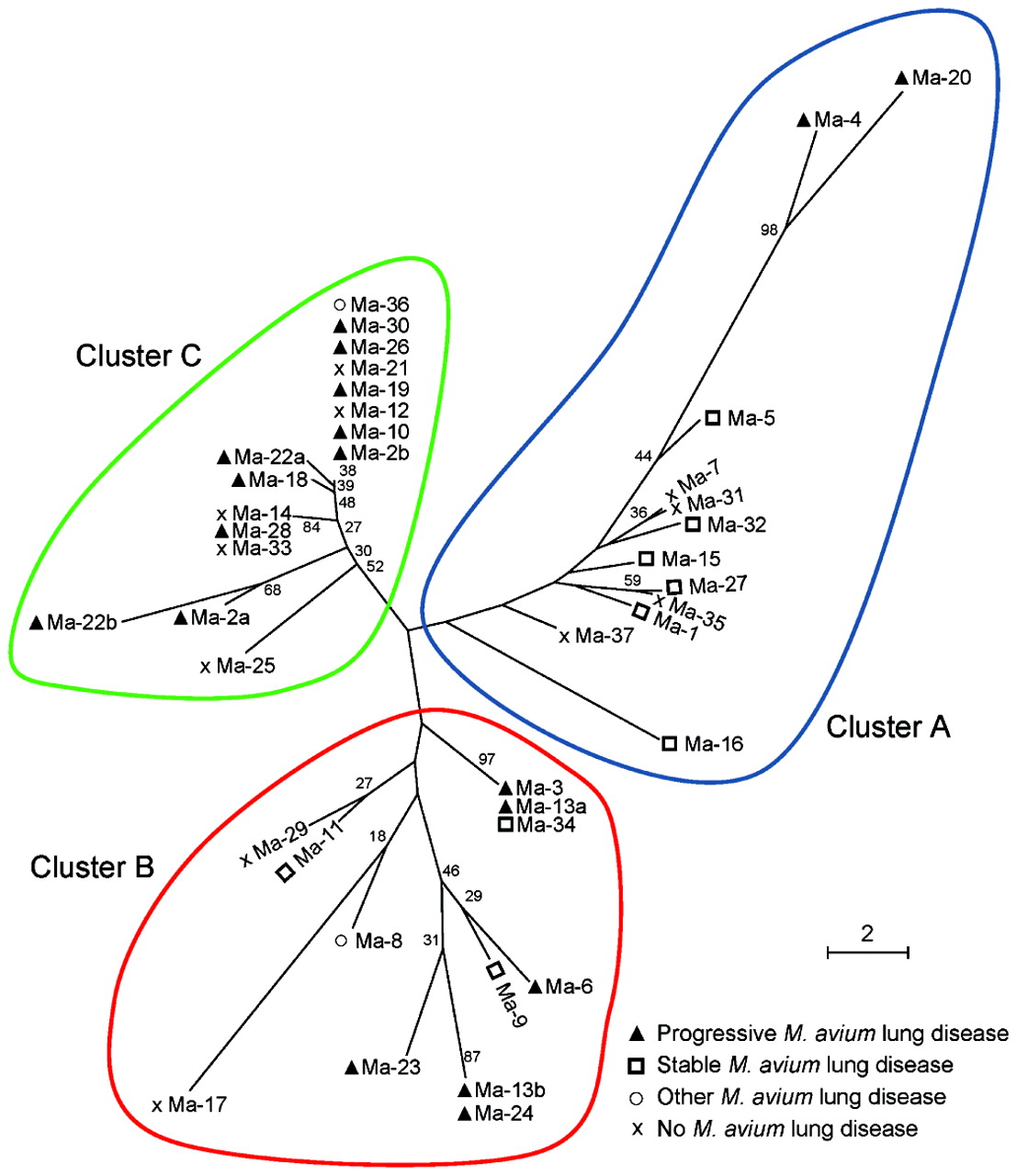
Genotypic diversity in VNTR profiles was calculated as the Manhattan distance between each pair of M avium isolates and analysed using a neighbour-joining algorithm. In the phylogenetic tree (showing relationships among VNTR profiles), M avium clinical isolates were grouped into three major clusters designated as follows: cluster A including 12 isolates, cluster B including 12 isolates and cluster C including 16 isolates (fig 2). The branches in cluster C were supported by bootstrap values of 27–84%, whereas clusters A and B were interspersed with branches of low bootstrap support (<10%). Distinct isolates cultured from one subject were located close to one another on the genotypic distribution and classified into the same cluster (ie, Ma-2a/-2b in cluster C, Ma-13a/-13b in cluster B and Ma-22a/-22b in cluster C). From these observations, all 37 subjects who provided respiratory specimens positive for M avium were assigned to one of the three VNTR clusters.

Cluster analysis of Mycobacterium avium clinical isolates based on variable numbers of tandem repeats (VNTR) profiles. Based on the VNTR profile data for 40 M avium isolates, the Manhattan distance between each pair of isolates was calculated and analysed using a neighbour-joining algorithm. The phylogenetic distribution of M avium from subjects with progressive M avium lung disease, stable M avium lung disease, other M avium lung disease and no M avium lung disease is shown as a radial dendrogram. Progressive or stable M avium lung disease is defined as described in table 2. The three major branches of M avium are designated as clusters A, B and C. Numbers along the branches denote bootstrap support as percentages of 1000 replicate data sets (shown only for values greater than 10). The scale bar indicates genetic distance.
As summarised in table 2, M avium-infected patients with progressive or stable lung disease were more likely to be grouped in cluster C or cluster A, respectively (progressive vs stable disease: cluster A, p = 0.02; cluster B, p = 0.99; cluster C, p = 0.01). Subjects without M avium lung disease did not differ significantly from those with M avium lung disease based on the VNTR profile classification (lung disease vs no lung disease: cluster A, p = 0.99; cluster B, p = 0.44; cluster C, p = 0.71; table 2). These data suggest that M avium genotypes are associated with the progression of M avium lung disease; however, isolate genotypes did not significantly predict the presence or absence of lung disease.
Risk of progression according to the genotypic diversity of M avium
The genetic relevance of mycobacteria to the clinical course of M avium lung disease allows for the use of logistic regression analysis. We selected one M avium isolate as a reference to evaluate the Manhattan distance of each M avium isolate and therefore determine the association between genotype and disease progression. Among the 40 M avium isolates examined, significant associations with progressive lung disease were found for 12 isolates including Ma-1, -5, -6, -7, -8, -9, -15, -27, -31, -32, -35 and -37 (age-adjusted ORs, 1.26–4.10; p = 0.01–0.04). In particular, the genetic distance of each M avium clinical isolate from Ma-31 was associated with the highest likelihood of disease progression (age-adjusted OR for subjects with progressive M avium lung disease vs those with stable M avium lung disease 1.95; 95% CI 1.16 to 3.30; p = 0.01).
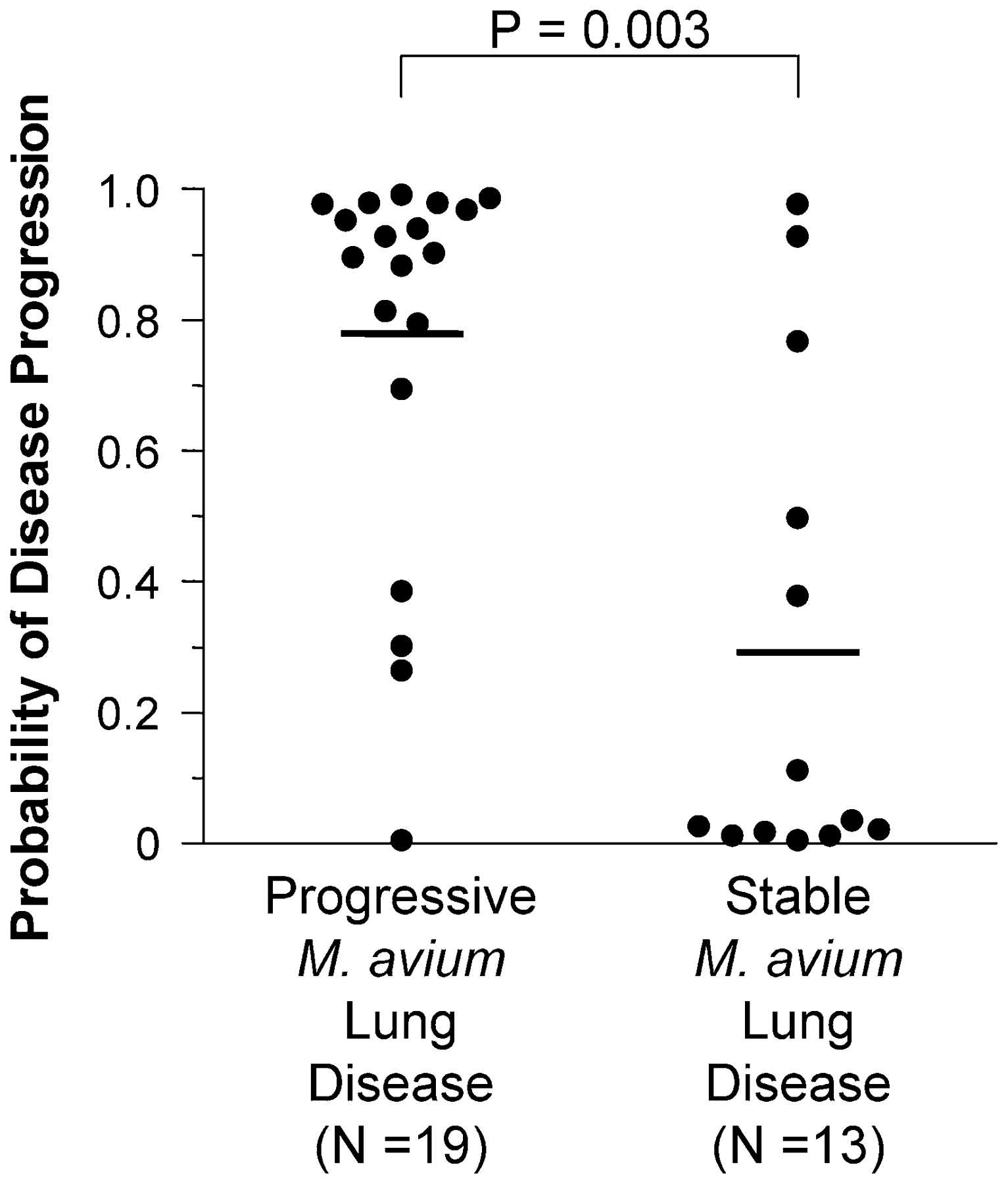
Finally, we sought to evaluate the sensitivity and specificity of the regression model using Ma-31 as a reference. The purpose of the evaluation was to assess our ability to distinguish subjects with progressive M avium lung disease from those with stable M avium lung disease. In an effort to improve the analysis, we examined additional VNTR profiles of M avium isolates obtained in 2007 from eight subjects (four subjects with progressive disease and four with stable disease), and combined the data with that of subjects sampled from 2005 to 2006 (due to small sample size). Based on the logistic regression model, we found that subjects with progressive M avium lung disease had a significantly increased probability of disease progression compared with those with stable M avium lung disease (mean (SD) 0.77 (0.19) vs 0.30 (0.38), p = 0.003; fig 3). On the basis of our criterion (probability of disease progression >0.5) for the positive prediction of progressive M avium lung disease, 15 of 19 subjects with progressive M avium lung disease were positive (sensitivity 79%) and 10 of the 13 subjects with stable M avium lung disease were negative (specificity 77%).
{kind=link}
{kind=link}
{kind=link}
Estimates of Mycobacterium avium lung disease progression. The probabilities of disease progression were calculated from the logistic regression analysis according to the Manhattan distances of M avium isolates from Ma-31. The results are shown for M avium isolates from subjects with progressive or stable M avium lung disease. Horizontal lines indicate mean values; p values were calculated using a Mann–Whitney non-parametric comparison test.
Discussion
Little is known regarding the factors that determine the clinical course of M avium lung disease. It is assumed, but not proven, that mycobacterial virulence and/or host predisposition influence disease progression.1 2 3 Based on the assumption that the progression of M avium lung disease depends, at least in part, on the M avium genotype isolated from the patient, we hypothesised that VNTR-based genotyping of M avium isolates would be a useful strategy for predicting disease progression. The observations gathered in the present study are consistent with this hypothesis. The distribution of M avium clinical isolates, as determined by VNTR profiles, demonstrates the existence of three clusters; M avium isolates from progressive lung disease and those from stable lung disease tend to be clustered differently. We then assessed the association between mycobacterial genotypes and disease progression of M avium lung disease by means of a logistic regression analysis. We found that the genetic distance calculated using Ma-31 as a reference was associated with the most significant age-adjusted ORs for disease progression. Lastly, a best-fit model was evaluated for its ability to predict the risk of disease progression in subjects with M avium lung disease.
Important issues yet to be addressed in the clinical area of NTM disease include therapeutic decisions regarding when to start treatment. Currently, no consensus exists among experts with respect to the treatment of patients with M avium lung disease, particularly the prevalent nodular bronchiectatic type. The clinical practice guidelines for NTM diseases were recently published by the American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA);3 however, this additional information has not resolved the aforementioned issues. According to the guidelines, there are complicated reasons for the lack of a consensus: (1) unlike fibrocavitary lung disease which is known to be generally progressive within a short time frame, the more predominant nodular bronchiectatic lung disease tends to show slower progression; (2) even with the more indolent bronchiectatic form of the disease, antimycobacterial treatment should be considered to prevent clinical deterioration and death; and (3) drug therapy for M avium disease involves long-term multidrug treatment (eg, 12 months or longer) with a relatively high risk of adverse drug reactions and/or toxicities, so the treatment of M avium disease seems worse than the disease for a patient with minimal symptoms and radiographic changes.3 7 8 20 21 22 23 24
It is therefore necessary to identify a clinical factor that is associated with disease progression to predict which patients with M avium lung disease are at the highest risk. In this context, it was reported that 176 of 181 patients (97%) who had two or more M avium complexes (MAC, including at least two mycobacterial species, M avium and M intracellulare) in the initial three sputum specimens collected following the onset of MAC lung disease subsequently developed new chest radiographic abnormalities.25 Although this report suggests that the frequency of positive sputum cultures for MAC is related to disease progression, the clinical value of this observation has not been conclusively established owing to substantial methodological limitations (accurate assessment of symptoms such as frequency of culture-positive sputum is often complicated in various clinical circumstances). Another study evaluated the association between MAC isolated from sputum with the prognosis of pulmonary MAC disease. This study showed that MAC serotypes could be determined using thin layer chromatography and mass spectrometry, and that patients with serotype 4 M avium pulmonary infection were generally non-responsive to antimycobacterial drug therapy. In addition, patients with serotype 4 had a poorer prognosis than patients with M avium organisms of other serotypes.26 These findings suggest the benefit of surgery for some patients whose MAC disease is selected as a drug-refractory infection by MAC serotyping. The most significant limitation to the widespread application of this method, however, is that highly sophisticated experimental techniques that are generally unfamiliar to standard clinical laboratories are required to determine MAC serotypes. In addition, several typing methods have been used to differentiate mycobacterium organisms including high-performance liquid chromatography (HPLC) of mycolic acids, restriction fragment length polymorphism (RFLP) profiling and trinucleotide repeat sequence (TRS) analysis.3 16 27 28 29 Further studies will be needed to assess the concordance between our VNTR method and another typing approach.
In the present study we found a significant association between PCR-based VNTR profiles of M avium isolates from patients with pulmonary infections and the risk of developing lung disease that requires drug treatment. These results suggest that VNTR profiles of M avium isolates, determined by the widely prevalent PCR method, may serve as a potential predictor of disease progression. The limitations of our study include the retrospective nature of the analyses and the uncertainty regarding the molecular mechanisms whereby the VNTR profile can discriminate between M avium isolates relevant to disease progression. In this regard, Hanekom et al reported that epidemiologically unrelated Mycobacterium strains may be incorrectly linked together by using the genetic distance of the VNTR profile.30 Despite these limitations, our findings provide compelling evidence that M avium genotype rather than host predisposition is contributing to the progression of pulmonary infection. Further investigation of the M avium strains isolated in progressive and stable disease, such as whole genome scanning of these strains, is warranted to identify molecular factors responsible for the increased risk of progressive M avium lung disease.
Acknowledgments
The authors thank Mitsu Takahashi and Yuko Sasaki for their assistance with VNTR profiling.
REFERENCES
Supplementary materials
Web only appendix for 64;10:901
Files in this Data Supplement:
Footnotes
Funding These studies were supported in part by the Ministry of Education, Culture, Sports, Science and Technology (Tokyo, Japan) and the Core Research for Evolutional Science and Technology Program of the Japan Science and Technology Agency (Tokyo, Japan).
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
▸ An additional table is published online only at http://thorax.bmj.com/content/vol64/issue10