Article Text

Abstract
Objective To assess the 6-month efficacy of uvulopalatopharyngoplasty (UPPP) compared with expectancy in selected patients with obstructive sleep apnoea syndrome (OSAS).
Design A prospective single-centre randomised controlled trial with two parallel arms stratified by Friedman stage and body mass index (BMI).
Participants 65 consecutive patients with moderate to severe OSAS (apnoea-hypopnoea index (AHI) ≥15 events/h sleep), BMI <36 kg/m2, Epworth sleepiness scale ≥8, Friedman stage I or II.
Intervention Surgical treatment with UPPP. The control group underwent UPPP after a delay of 6 months.
Outcomes Changes in AHI and other polysomnography parameters at baseline compared with the 6-month follow-up.
Results All patients (32 in the intervention group and 33 in the control group) completed the trial. The mean (SD) AHI in the intervention group decreased significantly (p<0.001) by 60% from 53.3 (19.7) events/h to 21.1 (16.7) events/h . In the control group the mean AHI decreased by 11% from 52.6 (21.7) events/h to 46.8 (22.8) events/h, with a significant difference between the groups (p<0.001). The mean time in the supine position and the BMI were unchanged in both groups. Subgroup analyses for Friedman stage, BMI group and tonsil size all showed significant reductions in AHI in the intervention group compared with controls. There were no severe complications after surgery.
Conclusions This trial demonstrates the efficacy of UPPP in treating selected patients with OSAS with a mean reduction in AHI of 60% compared with 11% in controls, a highly significant and clinically relevant difference between the groups.
Trial registration number NCT01659671.
- Sleep apnoea
Statistics from Altmetric.com
Key messages
What is the key question?
-
Are the respiratory events during sleep (apnoea-hypopnoea index, AHI) significantly reduced in selected patients with OSAS treated with UPPP (plus tonsillectomy) compared with expectancy for 6 months?
What is the bottom line?
-
This study shows a highly significant and clinically relevant difference in AHI reduction in favour of UPPP compared with expectancy.
Why read on?
-
This is the first randomised controlled trial of UPPP in patients with OSAS to evaluate AHI with in-laboratory polysomnography. Subgroup analyses showed that patients with small tonsils also benefit from surgery.
Introduction
The prevalence of obstructive sleep apnoea syndrome (OSAS) is approximately 4% of men and 2% of women in the USA.1 Increased morbidity and 3–4 times increased mortality in patients with severe OSAS are well documented.2–4 OSAS involves intermittent pharyngeal breathing obstruction during sleep, often with subjective daytime sleepiness as a consequence. Aetiological factors may be tonsillar hypertrophy and/or an excessively soft palatal mucosa which closes the oropharyngeal airway during inspiration. Uvulopalatopharyngoplasty (UPPP)5 was the predominant treatment for unselected patients with OSAS worldwide before continuous positive airway pressure (CPAP) devices became widely available in the 1990s. Since then, the main treatment for OSAS has been CPAP, but an increasing number of patients are also treated with a mandibular retaining device (MRD). CPAP treatment is successful when fully accepted and used by the patient. However, studies show that approximately 29–83% of patients are non-adherent to CPAP treatment for more than 4 h a night,6 and that the median compliance rate is approximately 50–77% after 1–3 years.7 ,8 Also, for MRD treatment the compliance rate is moderate at about 56% after 5 years.9
The role of UPPP has been questioned because of its possible side effects, complications and also a lack of efficacy in treating patients with OSAS.10 However, our group has published several non-randomised studies showing that UPPP may be effective and safe,11 even in the long-term perspective,12 and the pharyngeal disturbances had not increased 1 year after UPPP.13 Franklin et al14 found neither increased mortality nor an increased complication rate after UPPP compared with tonsillectomy in Sweden during 1997–2005. Methods to better select patients for UPPP have been sought. The first to predict surgical outcome was the Friedman staging system in 2002 based on tonsil size and tongue position.15 The system has subsequently been widely used in Sweden.
Randomised controlled trials (RCTs) to evaluate the efficacy of UPPP have been called for.16 Our aim was to initiate this sleep apnoea Karolinska UPPP (SKUP3) RCT in selected patients with OSAS.
Methods
Trial design
The trial was a single-centre prospective controlled trial with two parallel arms and stratified randomisation.
Participants
All patients with OSAS referred consecutively to the Oto-Rhino-Laryngology (ORL) Department, Karolinska University Hospital, Stockholm, Sweden from June 2007 to May 2011 for UPPP were possible candidates for inclusion in the study. In accordance with our clinical routine, they had previously been diagnosed and offered non-surgical treatment elsewhere, except for the patients with Friedman stage I and body mass index (BMI) <30 kg/m2 who did not have to have failed non-surgical treatment before surgery. All patients had undergone screening ambulant polygraphy prior to the first visit to a physician. They had completed the Epworth Sleepiness Scale (ESS)17 as well as a local questionnaire concerning general health, medication, BMI, tiredness and sleep patterns. Examinations by an ORL physician included nasoscopy, fibre endoscopy of the upper airways and staging of tonsil size (scale 0–4), as well as tongue position (scale 1–4), leading to the Friedman staging system: stage I (large tonsils and low tongue position), stage II (large tonsils and high tongue position or small tonsils and low tongue position), stage III (small tonsils and high tongue position).15 Patients who met the criteria for the study were invited to participate and were enrolled in the study by different physicians at the ORL department, including the researchers.
The run-in period started with a first full-night in-laboratory polysomnography (PSG) after approximately 1 month. During that recording the patients answered the questionnaires again and their weight and length were measured. Those who declared an interest in participating and met the criteria after the in-laboratory night were included in the study by randomisation.
The inclusion criteria were: (1) men and women >18 years of age; (2) apnoea-hypopnoea index (AHI) ≥15 events/h sleep (from PSG, see below); (3) ESS value ≥8; (4) marked daytime sleepiness ≥3 times a week; (5) BMI <36 kg/m2; (6) Friedman stage I or II; and (7) failure of CPAP and MRD treatment and no use of this treatment during the last 3 months. Patients with Friedman stage I and BMI <30 kg/m2 did not have to have failure of CPAP/MRD before inclusion.
The following exclusion criteria were used: (1) serious psychiatric, cardiopulmonary or neurological disease or American Society of Anesthesiologists (ASA) classification >3; (2) patients negative to surgery; (3) insufficient knowledge of Swedish; (4) nightshift workers; (5) patients who could be dangerous in traffic; (6) serious nasal congestion (could be included after local treatment); (7) previous tonsillectomy; (8) Friedman stage III; and (9) serious clinical worsening of OSAS during the study.
To increase the external validity we developed a two-centre study: the ORL outpatient clinics at Karolinska University Hospital, sites Huddinge and Solna. At the start of the study these sites were two separate clinics but were combined into one site during the study and all patients with OSAS were allocated to the Huddinge site. Subsequently, only four patients were included from the Solna site. As all four deviated from the study protocol for different reasons and because of the low statistical power at this centre, we were urged by the statisticians to exclude these patients as well as the centre itself. Accordingly, all participants in this study were recruited from the Huddinge site as a single-centre study (figure 1).

Flow of participants in single centre (June 2007 to May 2011). AHI, apnoea-hypopnoea index; ESS, Epworth Sleepiness Scale.
Intervention
Patients were randomised to receive either UPPP within 1 month or no treatment at all for 7 months. After the second evaluation with PSG the patients in the control group also had surgical treatment. All patients were instructed to maintain their weight, to avoid new medicines, and were restricted from other OSAS treatments during the study.
Surgical method of uvulopalatopharyngoplasty
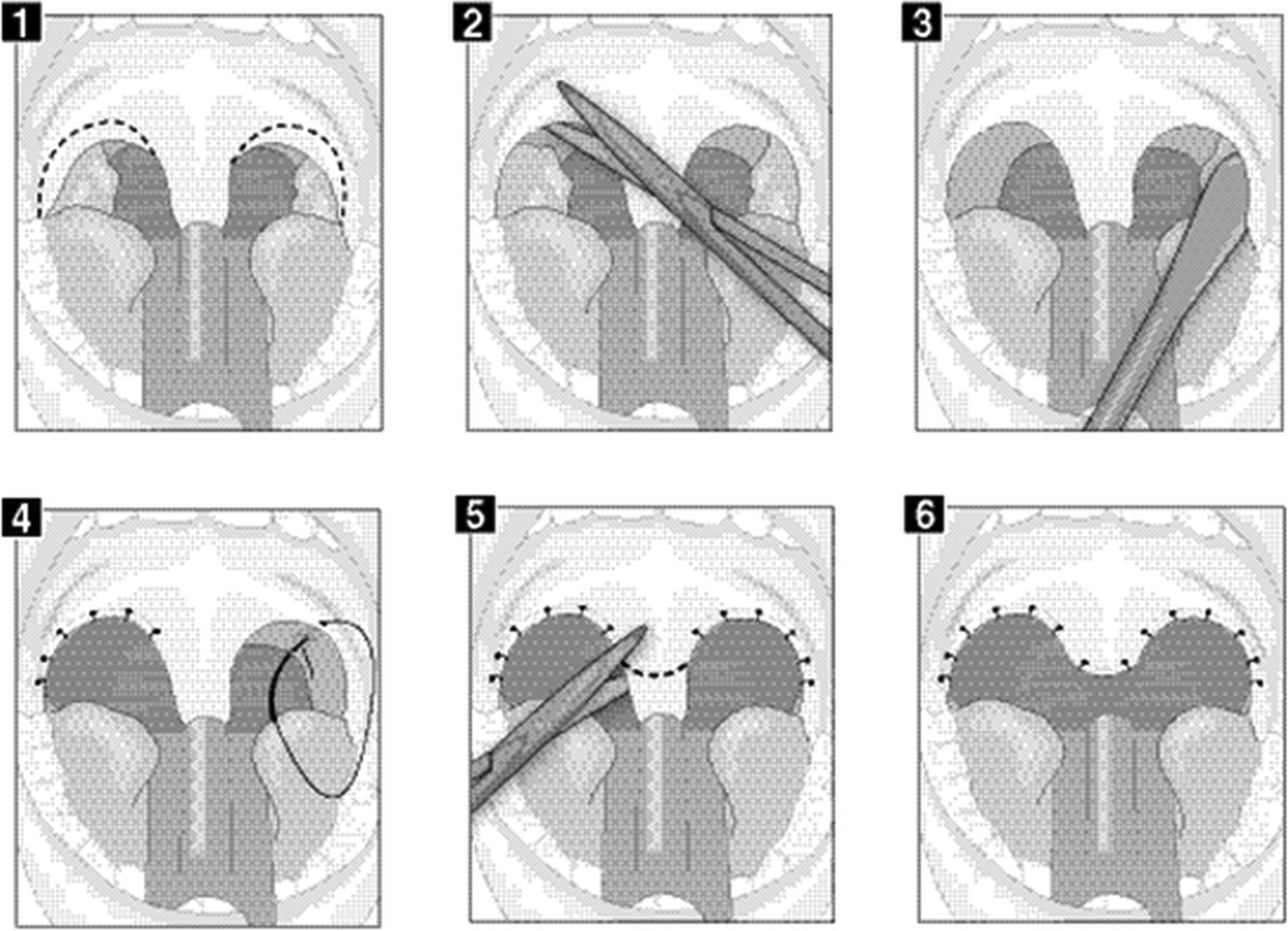
All patients underwent surgery under general anaesthesia using a nasal tube at the ORL Department of Karolinska University Hospital, site Huddinge. Local anaesthesia was administered before surgery. The surgical procedure was carried out using the cold steel technique and included tonsillectomy. The procedure had been slightly modified since our previous study11 to minimise the risk of side effects, involving excisions of the soft palatal mucosa only laterally to the uvula, which was only reduced (figure 2).
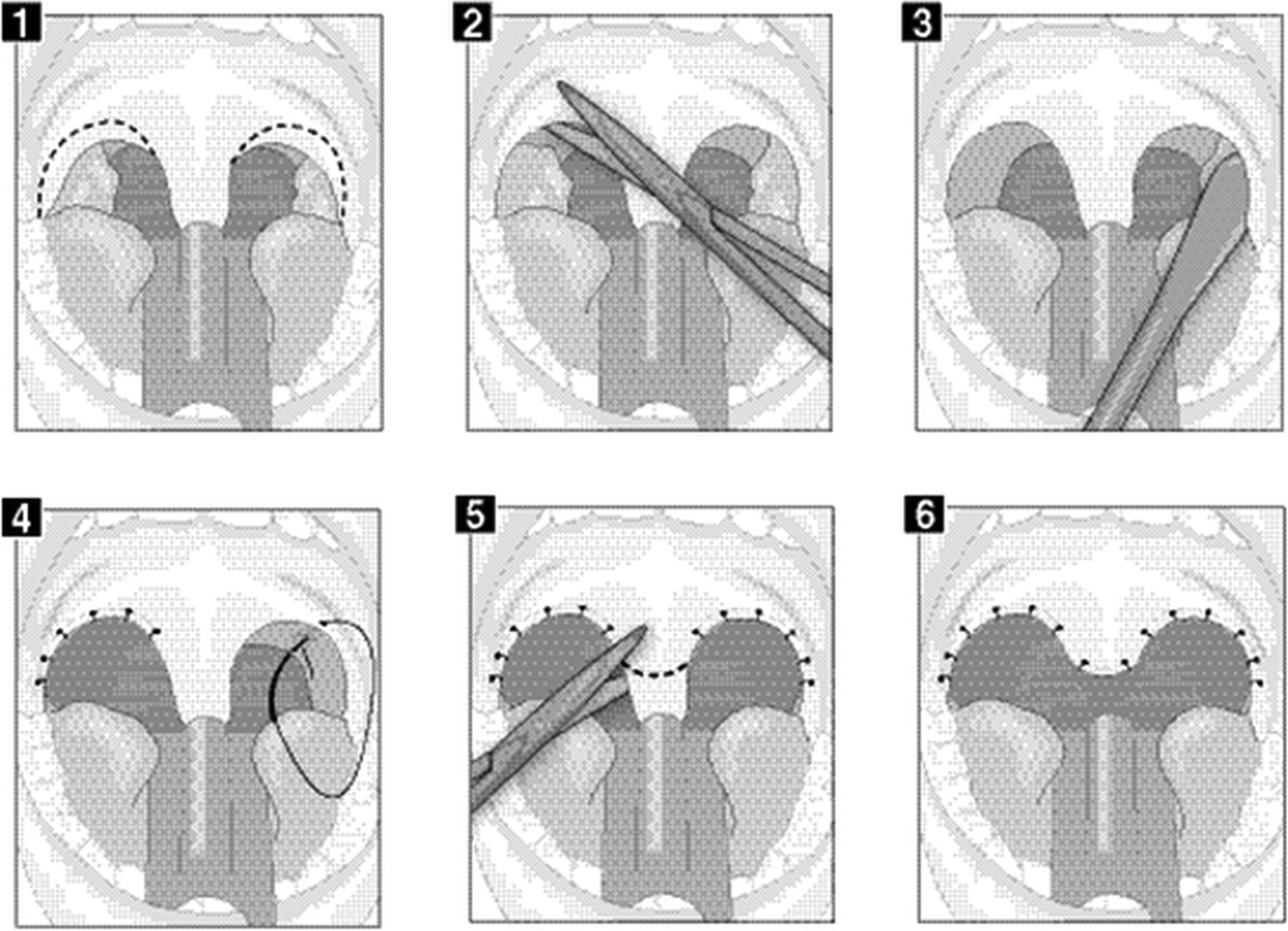
Method of uvulopalatopharyngoplasty. (1) Marked excision line laterally to the uvula. (2) Excision of the anterior tonsillar pillar 2–3 mm and the mucosa between the pillars. (3) Tonsillectomy with cold steel (Henke). (4) Single sutures (the ‘loop’ consists of needle and thread) lift up the posterior pillar, together with the palatopharyngeal muscle, to the anterior pillar, and also with suturing of the soft palatal mucosa. (5) Amputation of the uvula leaving approximately 1 cm. (6) Final result.
Safety
All the patients who underwent UPPP were included in our safety programme previously described by our group.11 Directly after extubation they were transferred to the postoperative care unit for 6–24 h observation, depending on the severity of their condition. Additionally, all patients had perioperative penicillin prophylaxis and postoperatively for 3 days. Two modifications of the safety programme were made before this study—namely, perioperative cortisone and peri- and postoperative tranexamic acid for 5 days.
Hypothesis
We hypothesised that UPPP significantly improves AHI compared with expectancy.
Primary and secondary outcomes
The primary outcome was the change in AHI measured by PSG and secondary outcomes were changes in other respiratory and sleep parameters.
Polysomnography
Respiratory and sleep parameters were measured at baseline and 6 months after intervention or expectancy by an in-laboratory full-night PSG using the same Embla technology (Flaga Medical; Reykjavik, Iceland). Measurements were interpreted manually by a single scorer who was blinded to randomisation. The patients were awakened at 06.00 h due to the sleep laboratory location in a daycare unit. Sixteen channels were recorded: EEG (sensors C3-A2, O1-A2, O2-A1, C4-A1), EOG (left and right), EMG chin and tibialis (left and right), oronasal thermistor and flowmetry, transcutaneous oxygen saturation, respiratory movements (abdomen and thorax), snoring, ECG, pulse and body position. Parameters were defined according to AASM 200718 using criteria B for hypopnoea (at least a 50% flow reduction leading to either a 3% oxygen desaturation or arousal).
Sample size
The sample size was calculated prior to the start of the study by a statistician and was based on the results from a study showing the night-to-night variability of the oxygen desaturation index (ODI) values in patients with OSAS19 and also from one of our previous studies on patients with OSAS undergoing UPPP.11 The mean (SD) difference in ODI4 values of the patients from preoperative to postoperative status within the group was 13 (17.3) events. The sample size calculation for this RCT was based on having a 90% power with an α level of 5%, and resulted in 64 patients who satisfied the criteria for the study.
Randomisation
Stratified randomisation within four strata was used. Group A: Friedman stage I and BMI <30 kg/m2; Group B: Friedman stage II and BMI <30 kg/m2; Group C: Friedman stage I and BMI 30–35.9 kg/m2; Group D: Friedman stage II and BMI 30–35.9 kg/m2. With the aid of the statisticians, the stratified randomisation was done using sealed envelopes numbered 1–60 in each of the four groups, administered in a determined order, all concealed from the researchers. All patients were assigned a study identification number and a stratification category. All written information about the patients was kept in separate folders in a locked room. The dataset was coded using the study number and category. The researchers followed Good Clinical Practice.
Seventy-one patients were randomised. During the run-in period two patients had changed one inclusion parameter: at the in-laboratory PSG visit one patient had decreased the ESS value to <8 and another had slightly increased the BMI to 36 kg/m2. This was discovered by the researchers after randomisation and both patients were excluded as they deviated from the study protocol. The four patients from the other centre were also excluded as described earlier. Subsequently, 65 randomised patients followed the study protocol and fulfilled all the criteria (figure 1).
Statistical analysis
The follow-up time is presented as median (range). Changes within groups are calculated by subtracting the outcomes of PSG 1 from those of PSG 2 and presented as mean (SD). Changes between groups are presented as mean (95% CI). Since the sample size was >30, parametric statistical analyses were used and we also checked the distribution. Paired t tests were used to compare the differences between PSG 1 and PSG 2 in each group, and unpaired t tests were used to compare the changes between the two groups. All 65 participants were analysed in the per protocol analysis. We had no drop-outs and the sensitivity analysis with intention-to- treat (ITT) was performed with the 65 patients together with the excluded patients (figure 1). Missing values for these six patients were imputed by using their baseline values +1. Also, for analyses of different subgroups, t tests were used due to normal distribution. All statistical calculations were performed using Statistica V.10.0.
Results
The baseline characteristics of the groups are presented in table 1. All 65 included patients underwent PSG 1 at baseline and PSG 2 at follow-up. The median time between them was 7.2 months (range 4.8–14.6) for the intervention group and 6.7 months (range 4.8–8.5) for the control group. There were six women in the study, and three patients with Friedman stage I and BMI <30 kg/m2 who had not failed CPAP and MRD treatment before inclusion. A total of eight different surgeons, all ORL specialists, performed the UPPP.
Baseline characteristics of the two study groups
Primary outcome
At follow-up (PSG 2) the AHI in the intervention group had significantly decreased from a mean (SD) of 53.3 (19.7) events/h sleep to 21.1 (16.7) events/h sleep (p<0.001). There was no significant change in the control group, the mean having changed from 52.6 (21.7) events/h sleep to 46.8 (22.8) events/h sleep. Three patients in the intervention group and 10 in the control group had increased AHI at PSG 2 compared with PSG 1 (figure 3). The difference between the groups was highly significant (p<0.001, table 2). The mean reduction in AHI in the intervention group was 60% compared with 11% in the control group. Success rates according to different AHI criteria are shown in table 3. Analyses of the subgroups showed that, independent of BMI group, tonsil size or Friedman stage, the differences in AHI reduction were significant in favour of the intervention group, except for tongue position 3 (table 4).
Body mass index (kg/m2) and polysomnographic parameters in polysomnography (PSG) 1 and PSG 2, and mean difference between groups
Number (%) of patients in each group with different criteria for success at polysomonography (PSG) 2
Mean apnoea-hypopnoea index (AHI) at polysomnography (PSG) 1 and PSG 2 in different subgroups and mean difference between groups

{kind=link}
{kind=link}
{kind=link}
Boxplots and lines showing the apnoea-hypopnoea index (AHI) on two different polysomnography occasions (before and after) in the intervention and control groups. Boxes represent the median, 25% and 75% values, whiskers show the non-outlier range and dots represent the outliers. p Values represent the changes within groups (paired t tests).
Secondary outcomes
There were significant reductions in the apnoea index (part of AHI) in both the intervention group (from mean 41 to 13, p<0.001, 68%) and the control group (from mean 43 to 34, p<0.05, 21%), with a highly significant difference between the groups (p<0.001). There were also significant changes in other respiratory parameters in the intervention group compared with the control group (table 2).
The percentage of sleep time in the supine position was increased from a mean of 39% to 45% in the intervention group but was unchanged in the control group at PSG 2 compared with baseline. BMI remained stable in both groups, with no change in the intervention group and an increase of 0.4 kg/m2 in the control group (table 2).
Sensitivity analysis
The ITT analysis, in which all parameters in table 2 were calculated for the 71 randomised patients for the difference between groups, did not change the results compared with the per protocol analysis with 65 patients.
Adverse effects
All 32 patients operated upon went home the day after surgery. Six of the 32 had non-serious complications. Four had prolonged duration of pain which was treated with different analgesics and two had postoperative bleeding which was treated medically. One had a night of observation in hospital 3 days after surgery. There were no serious complications or mortality. No patient was excluded owing to serious clinical impairment.
Discussion
Our main finding in this RCT was the clinically relevant and statistically significant difference in the mean reduction of AHI in favour of the UPPP intervention group compared with controls. Furthermore, UPPP significantly reduced the mean AHI after 6 months in the intervention group by 60% compared with 11% in the control group. This can be compared with figures from other centres reported in a recently published meta-analysis of 15 cohort studies after UPPP, with a mean AHI reduction of 33%.20
The reduction in the apnoea index (21%) and AHI (11%) in the control group may be caused by regression to the mean, which occurs when there is a minimum PSG value required for inclusion. Another reason for the improvement in the control group could be an increased awareness of the disease after entering the study, and we cannot exclude the possibility of minor individual changes in conservative treatment during the study. However, both the mean time in the supine position and the mean BMI were mainly stable in both groups and thus probably did not affect the results.
Other respiratory parameters (ODI3, nadir) followed the pattern and showed significant differences between the groups in favour of the intervention group, which supports the result for our primary outcome. Also, the apnoea index decreased significantly but the hypopnoea index was not reduced in the same manner. Furthermore, there was a small but significant increase in the mean respiratory effort-related arousal index after UPPP compared with the control group. These findings are in accordance with a review by Sher et al21 and could be explained by the hypothesis that UPPP only partially increases the airflow, transforming apnoea (90% flow reduction) to hypopnoea (50% reduction) and hypopnoea to a respiratory effort-related arousal (30% reduction).
A somewhat unexpected finding was that, although the respiratory parameters changed significantly in this study, we did not find significant differences between groups in other sleep parameters except for the mean arousal index. A slight improvement in the percentage of deep and/or REM sleep would have been expected in the intervention group. However, the restricted sleep time, with wake-up at 06.00 h, may have influenced these results. Furthermore, the baseline values were mainly within the normal range, thus not offering an opportunity for a large improvement. On the other hand, the mean total arousal index decreased in favour of the intervention group. Sleep fragmentation caused by arousals is considered to be the major factor in daytime symptoms.22 In the present study there were no serious complications after surgery. This may be the result of our safety programme.
The only known previous RCT of UPPP compared with expectancy is a study by Lojander et al in which 18 patients were randomised to UPPP (5 of them had an additional mandibular osteotomy) and 14 to expectancy. After 1 year the ODI4 changed significantly from 45 events/h sleep to 14 events/h sleep in the intervention group compared with a reduction from 34 events/h sleep to 23 events/h sleep in the control group, but the difference between the groups was insignificant.23 The results may be explained by the small study sample.
Our subgroup analysis showed significant differences in AHI reduction between the intervention group and controls, independently of BMI groups, tonsil size or Friedman stage. Friedman et al15 had shown in a non-randomised study that patients with stage I had an 80% success rate (defined as respiratory disturbance index ≤20 and a reduction of ≥50%) and those with stage II had a success rate of 38% after UPPP, and that a BMI <40 kg/m2 did not affect the surgical results. Our study is the first to confirm these results in an RCT and an untreated control group, thereby showing significant differences between groups despite small sample sizes in each subgroup. The finding that patients with small tonsils also may benefit from surgery is supported by our previous UPPP study of 158 patients in which tonsil size did not predict the outcome.11 This indicates that opening of the airway is mainly caused by the uplift of the soft palate and lateralisation of the posterior tonsillar pillars, and not the tonsillectomy per se. Owing to our clinical routines we did not perform drug-induced sleep endoscopy (DISE), which may have added information about the obstruction site (palatal or hypopharyngeal). A previous study of patients with a preoperative mean AHI of 29 who underwent DISE showed a success rate (defined as AHI<15) of 69% after UPPP.24 This can be compared with our success rate of 47% with similar criteria. However, our patients had a higher preoperative mean AHI of 53, which make comparisons between the two study populations difficult, although it is possible that with DISE we could have enhanced the selection of patients for UPPP and improved our success rate.
CPAP is the main treatment option for the general OSAS population, especially in moderate to severe disease. In mild to moderate disease, MRD can be an optional therapy. Furthermore, CPAP is favourable in patients with cardiovascular disease and may reduce hypertension.25 There is also evidence of decreased mortality in patients with OSAS after CPAP treatment.2 However, the efficacy of CPAP, when used properly by patients, may be hampered by a fairly low rate of adherence/compliance.6 The episodes without effective treatment mean that patients with moderate OSAS reduce AHI only by 33–48% when using CPAP 3 h per night.26 Compared with CPAP, MRD has a lower efficacy but compliance in a recent study was >80% after 3 months27 even though there are studies showing impaired compliance over time.9 When comparing different treatment options, the adherence/compliance rate must be taken into account, and for surgery it is 100%.26 ,28 Reflecting the limitations of non-surgical therapy, UPPP may be an option—at our clinic in approximately 10–15% of the patients with OSAS. However, this may vary depending on local traditions.
Strengths and weaknesses of the study
The strength of the present study is the randomised controlled design which minimises the risk of a selection bias and confounding factors. Additionally, only a single person, blinded to patient grouping, interpreted all PSGs manually. A further strength is the use of in-laboratory PSG, which is the golden standard for investigating OSAS. Also, all patients had undergone ambulatory polygraphy before the baseline in-laboratory PSG, which implies that the AHI limit of ≥15 for inclusion was valid. Furthermore, there were no drop-outs in the study, probably because we encouraged the operated patients on several occasions to complete their follow-up. The main weakness of the study is the short duration of only 6 months, but the researchers (as well as the ethical approval committee) considered it unethical to leave the patients in the control group untreated for a longer time. Six patients were also excluded after randomisation, but they were allocated to separate groups and did not affect the results.
Generalisability
The general population of adult OSAS patients in Sweden is not similar to the one in the present investigation. First, our population was at least 10–15 years younger and the majority had a BMI of <30 kg/m2, much lower than the general adult OSAS population and also compared with a population having CPAP treatment.7 ,29 Second, our study did not include patients with Friedman stage III or those with severe comorbidity or BMI ≥36 kg/m2. Furthermore, the second centre did not complete the study. On the other hand, as many as eight different surgeons performed the surgery, which means that the result is not dependent on a single surgeon.
Future research suggestions
More RCTs evaluating UPPP in order to perform meta-analyses would be desirable. Research priorities should address success factors and evaluations of respiratory parameters, side effects and mortality also in the long-term perspective. Another area of interest is how UPPP affects subjective parameters including daytime sleepiness symptoms and quality of life, as well as its impact on metabolic parameters and vigilance.
Conclusion
This single-centre RCT shows that UPPP treatment is safe and significantly more efficient than expectancy in selected patients with OSAS. We recommend that UPPP should be offered to such patients, especially those who fail with CPAP and/or MRD and would otherwise usually remain untreated.
Acknowledgments
We thank our former Head of Department, Professor Pär Stjärne, for encouraging the start of this trial and in-laboratory polysomnography; Per Olle Haraldsson for valuable advice concerning modification of the surgical technique; Leah Steinberg for interpreting all the polysomnographies; nurses Maria Axelsson, Carina Hedenström and Madeleine Gülger for valuable assistance; and our colleagues for recruiting and operating on the study patients, all at the ORL Department, Karolinska University Hospital.
References
Footnotes
-
Contributors NB, PN, ML and DF conceived the study hypothesis. NB, JB and DF did the statistical analyses. NB and DF wrote the first draft of the manuscript. PN, ML and JB provided critical input at all stages and critically reviewed and contributed to the final draft. All authors are guarantors.
-
Funding This work was partly supported by grants from the Swedish Association of Sleep Medicine and Sleep Research, the Acta Otolaryngologica Foundation and the Rosa and Emanuel Nachmansson Foundation.
-
Competing interests None.
-
Ethics approval The study was first rejected by the Swedish Regional Ethics Committee, 2007/449-31/3 and, after an appeal, approved by the Central Ethics Committee, Ö21-2007.
-
Provenance and peer review Not commissioned; externally peer reviewed.