Article Text

Abstract
Background Expiratory flow limitation and lung hyperinflation promote cardiocirculatory perturbations that might impair O2 delivery to locomotor muscles in patients with chronic obstructive pulmonary disease (COPD). The hypothesis that decreases in lung hyperinflation after the inhalation of bronchodilators would improve skeletal muscle oxygenation during exercise was tested.
Methods Twelve non- or mildly hypoxaemic males (forced expiratory volume in 1 s (FEV1)=38.5±12.9% predicted; Pao2>60 mm Hg) underwent constant work rate cycle ergometer exercise tests (70–80% peak) to the limit of tolerance (Tlim) after inhaled bronchodilators (salbutamol plus ipratropium) or placebo. Muscle (de)oxygenation (∼fractional O2 extraction) was determined in the vastus lateralis by changes (Δ) in the deoxyhaemoglobin/myoglobin signal ([HHb]) from near-infrared spectroscopy, and cardiac output (QT) was monitored by impedance cardiography.
Results Bronchodilators reduced lung hyperinflation and increased Tlim compared with placebo (454±131 s vs 321±140 s, respectively; p<0.05). On-exercise kinetics of QT and pulmonary O2 uptake
Conclusions Decreases in operating lung volumes after the inhalation of bronchodilators are associated with faster ‘central’ cardiovascular adjustments to high-intensity exercise with beneficial consequences on muscle oxygenation in patients with moderate to severe COPD.
- Bronchodilator
- chronic obstructive pulmonary disease
- exercise tolerance
- oxygen consumption
- respiratory mechanics
Statistics from Altmetric.com
- Bronchodilator
- chronic obstructive pulmonary disease
- exercise tolerance
- oxygen consumption
- respiratory mechanics
Introduction
Exercise intolerance is a multifactorial construct in patients with chronic obstructive pulmonary disease (COPD).1–3 In fact, recent studies from our laboratory suggest that expiratory flow limitation and lung hyperinflation are related to sluggish central cardiovascular adjustments at the onset of exercise which might impair the balance between O2 delivery (QO2) and uptake
In the present study, therefore, we aimed to investigate the effects of acute inhalation of a combination of a short-acting β2-adrenoceptor agonist (salbutamol sulfate) and a short-acting anticholinergic (ipratropium bromide) on key determinants of QO2 and
Methods
Subjects
Twelve males with moderate to severe, stable COPD (forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) <0.7 and postbronchodilator FEV1<60% predicted), and resting Pao2>60 mm Hg, volunteered to participate in the study. Patients were recruited from the COPD Outpatients Clinic of the Sao Paulo Hospital (Brazil), a University-based teaching hospital. Subjects were free of echo Doppler cardiographic evidence of severe pulmonary hypertension and left ventricular dysfunction. No patient has ever been enrolled in a pulmonary rehabilitation programme. All participants signed a written informed consent form. The study protocol was approved by the Institutional Medical Ethics Committee.
Study protocol
This was a double-blinded, placebo-controlled crossover study. After determination of peak
Measurements
Pulmonary function tests
Spirometry, single-breath lung diffusing capacity, static lung volumes by body plethysmography and arterial blood gases were measured at baseline. Recorded values were compared with those predicted for the adult Brazilian population.8 9
Exercise tests
Standard metabolic and ventilatory responses were measured breath-by-breath using a calibrated, computer-based system (CardiO2 System, Medical Graphics, St Paul, Minnesota, USA). A period of 3 min unloaded exercise preceded the imposition of the selected work rate. Serial inspiratory capacity (IC, litres) manoeuvres were performed during the test. Assuming that total lung capacity (TLC) remains constant during exercise, IC manoeuvres provide an estimate of end-expiratory lung volume.10
Skeletal muscle oxygenation
Skeletal muscle oxygenation profiles of the left vastus lateralis were evaluated with a commercially available NIRS system (Hamamatsu NIRO 200, Hamamatsu Photonics KK, Japan). The (deoxyhemoglobin (Hb)/myoglobin (Mb) signal ([HHb], μM/cm) during exercise has been considered a proxy of fractional O2 extraction in the microcirculation, reflecting the balance between O2 delivery and utilisation11 12—that is,
Central haemodynamics
Cardiac output (QT, l/min) and stroke volume (SV, ml) were measured throughout the constant work rate test using impedance cardiography (PhysioFlow PF-0, Manatec Biomedical, Macheren, France).13 This methodology is different from previously used impedance systems as its algorithm does not require basal thoracic impedance measurement (Z0). Considering, however, the controversy on the accuracy of the system in providing reliable absolute values of SV in patients with COPD,14 15 exercise haemodynamic data were also expressed as ‘Δ’ from baseline. Additional information on response characteristics and system validation are detailed in the supplement online.
Kinetics analysis
The breath-by-breath
where b and p refer to baseline unloaded cycling and primary component, respectively; A, TD and τ are the amplitude, time delay and time constant of the exponential response. For
Statistical analysis
Statistical analysis was performed using SPSS 15.0. We planned to evaluate 12 patients based on our previous results in a similar transversal and crossover study with heliox in patients with COPD.5 Paired t test was used to contrast within-subject exercise responses with the exception of symptom scores (Wilcoxon signed-rank test). A one-way repeated measures analysis of variance (ANOVA) was used to compare Δ[HHb] at quartiles of isotime—that is, the shortest Tlim between the two interventions on a given subject. Pearson product–moment correlation was used to assess the level of association between continuous variables. The level of statistical significance was set at p<0.05 for all tests.
Results
Subject characteristics and maximum exercise capacity
On average, patients had severe airflow obstruction and lung diffusing capacity for carbon monoxide (DLCO) impairment with increased static lung volumes and normal arterial blood gases at rest (table 1). All patients showed reduced maximal exercise capacity (peak
Resting characteristics and responses to incremental exercise (n=12)
Effects of bronchodilators on pulmonary function and exercise tolerance
Treatment with bronchodilators increased FEV1 and IC compared with placebo (1.30±0.50 litres vs 1.17±0.56 litres and 2.28±0.83 litres vs 1.89±0.73 litres, respectively; p<0.001 for both comparisons). The criteria for a ‘positive’ bronchodilator response (FEV1 change ≥12% and 200 ml)21 were obtained in 7/12 patients, with FEV1 increases being closely related to changes in FVC.
The subjects exercised at 53±10 W. Exercise tolerance (Tlim) was improved after treatment with bronchodilators (321±140 s vs 454±131 s, for placebo and bronchodilators, respectively; p=0.01). Increases in pre-exercise IC were significantly related to Δ (bronchodilators–placebo) TLim (r=0.72 (95% CI 0.31 to 0.91); p=0.04). As previously described,13 increases in IC during exercise were accompanied by larger tidal and inspiratory reserve volumes and lower dyspnoea scores at isotime (table 2). In contrast, there were no significant effects of bronchodilators on mean Spo2 values (table 2), and improvements in Spo2 >3% at isotime were found in only 3/12 patients. Similarly, there were no significant between-interventions differences in the cardiovascular responses at the individual isotime (table 2).
Isotime values of selected physiological and perceptual responses during high-intensity, constant work rate exercise after placebo or bronchodilators (n=12)
Kinetics response to exercise
Treatment with bronchodilators accelerated the central haemodynamic responses at the onset of exercise (t1/2QT= 75.9±10.3 s vs 58.9±18.9 s (p=0.02), t1/2HR= 78.2±13.0 s vs 62.5 ±15.5 s (p=0.03), t1/2SV=51.0±8.1 s vs 40.6±10.3 s (p=0.02) for placebo and bronchodilators, respectively). In relation to the
Comparative effects of inhaled placebo vs bronchodilators (BDs) on selected parameters of the kinetics of pulmonary oxygen uptake  and deoxyhaemoglobin (Δ[HHb]) in the vastus lateralis at the onset of high-intensity, constant work rate exercise (n= 12)
and deoxyhaemoglobin (Δ[HHb]) in the vastus lateralis at the onset of high-intensity, constant work rate exercise (n= 12)
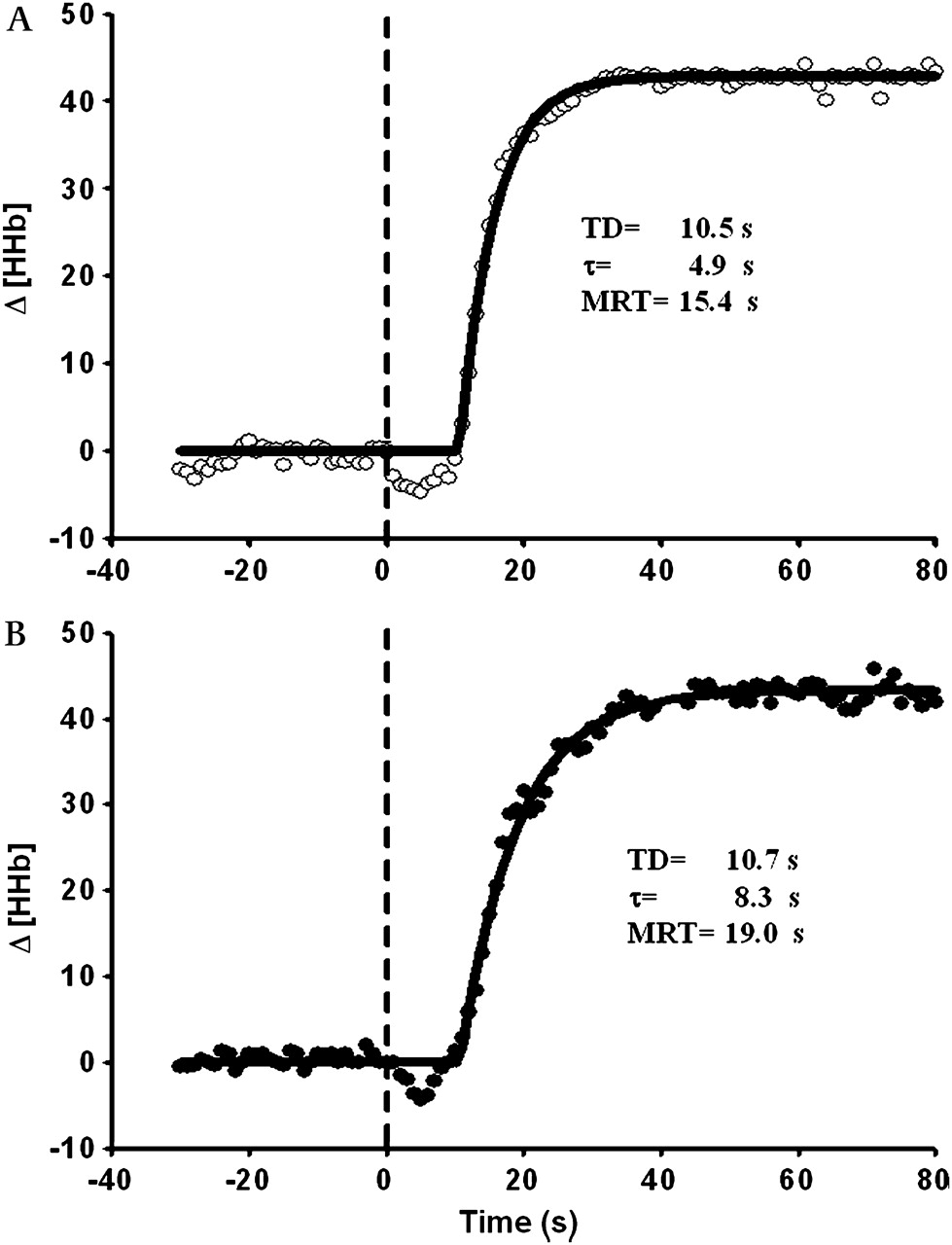
Bronchodilators slowed the kinetics of leg muscle deoxygenation compared with placebo (figure 1, table 3), despite no significant effects on baseline Δ[HHb] (3±15 μM/cm vs 2±13 μM/cm; p=0.83). Therefore, τΔ[HHb] postbronchodilators was, on average, twofold the postplacebo value (table 3). Consequently, the τ-

Comparative effects of inhaled placebo (A) and bronchodilators (B) on changes in deoxyhaemoglobin (Δ[HHb] by near-infrared spectroscopy) in the vastus lateralis in a patient with severe COPD. Note that bronchodilation was associated with slower Δ[HHb] adjustments. These data are consistent with improved microvascular O2 delivery to the peripheral muscles after bronchodilation. TD, time delay; τ, time constant; MRT, mean response time.
Interestingly, the decrease in lung hyperinflation (ie, higher IC) was significantly related to faster QT (figure 2A) and

Increases in inspiratory capacity (IC) with inhaled bronchodilators (Δ=bronchodilator–placebo) were associated with faster cardiac output (QT) kinetics (A) and larger decrements in τ- /MRT-[HHb]) (B). Collectively, these data suggest that improvement in central cardiovascular adjustments after reduction in the operating lung volumes with inhaled bronchodilators (A) led to faster dynamics of microvascular O2 delivery (B). t1/2, half-time; τ, time constant; MRT, mean response time;
/MRT-[HHb]) (B). Collectively, these data suggest that improvement in central cardiovascular adjustments after reduction in the operating lung volumes with inhaled bronchodilators (A) led to faster dynamics of microvascular O2 delivery (B). t1/2, half-time; τ, time constant; MRT, mean response time;  , oxygen uptake; [HHb], deoxyhaemoglobin by near-infrared spectroscopy.
, oxygen uptake; [HHb], deoxyhaemoglobin by near-infrared spectroscopy.
Muscle oxygenation and leg effort scores at steady-state exercise
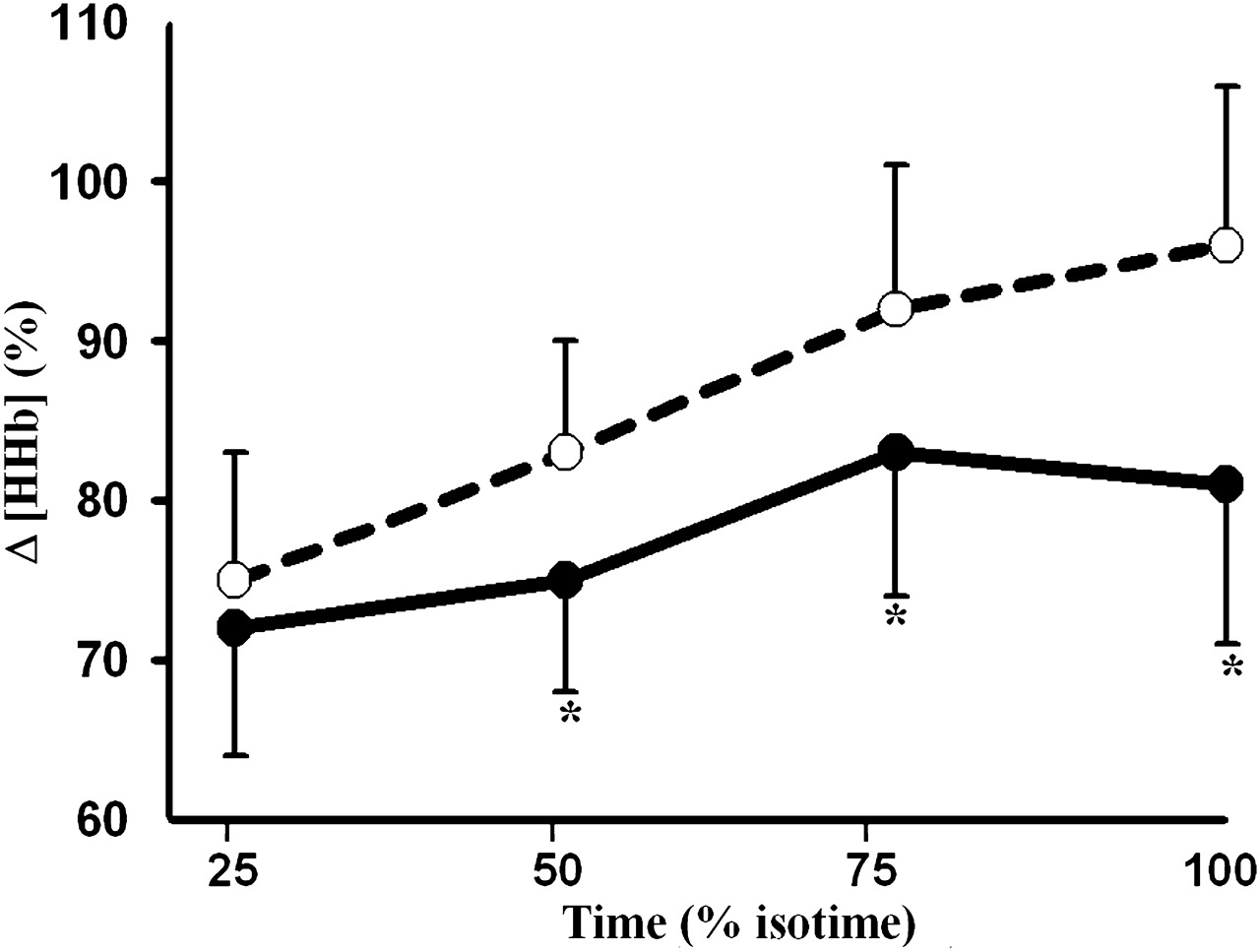
The amplitude of Δ[HHb] after the initial ‘fast’ response was significantly reduced with bronchodilators compared with placebo (185±115 μM/cm vs 153±108 μM/cm; p=0.009), remaining lower throughout exercise (figure 3). Δ[HHb] at isotime was significantly related to larger postbronchodilator increases in IC (r=−0.82 (95% CI −0.62 to −0.94); p=0.01) and improvements in Tlim (r=−0.80 (95% CI=−0.54 to −0.92); p=0.01). Leg effort scores at isotime were also lower after active treatment compared with placebo (table 2) and they were marginally related to changes in Tlim (r=−0.53; p=0.08).
{kind=link}
{kind=link}
{kind=link}
Effects of inhaled bronchodilators (filled symbols) and placebo (open symbols) on skeletal muscle deoxyhaemoglobin (Δ[HHb], % of maximal value obtained on a previous leg occlusion) in the vastus lateralis at standardised time points during high-intensity exercise. Isotime, the shortest exercise test between the two interventions on a given subject. Values are mean and standard error.
Discussion
This seems to constitute the first study to investigate the effects of inhaled bronchodilators on the determinants of (estimated) microvascular O2 delivery (QO2) and utilisation (phase II pulmonary
Interpreting the kinetics of muscle oxygenation during exercise
NIRS is a non-invasive technique that allows continuous measurement of key determinants of peripheral muscle oxygenation during exercise. The time course of Δ[HHb] reflects the local balance between QO2 and
In some specific circumstances, this pattern of response is further complicated by a transient ‘overshoot’ in Δ[HHb],25–27 indicating an increase in fractional O2 extraction above the steady-state level due to impaired phase II blood flow relative to muscle
Effects of bronchodilators on leg O2 delivery
The present study provides novel evidence that alleviation of airflow obstruction after pharmacological bronchodilation, with consequent reductions in lung hyperinflation (table 2), resulted in slower kinetics and lower amplitude of muscle deoxygenation (table 3 and figure 3, respectively). In addition, bronchodilators lessened or eliminated the ‘overshoots’ in Δ[HHb], further indicating that muscle oxygenation improved after active treatment. Although the precise mechanism(s) leading to enhanced leg oxygenation could not be determined in this non-invasive study, it is noteworthy that active treatment accelerated the kinetics of the ‘central’ haemodynamic adjustments to exercise. In this context, a decrease in the operating lung volumes might have been associated with increased reliance of parasympathetic control of HR,26 an effect that could be related to less airways compression27 and lower pulmonary arterial pressure.28 Reduction in air trapping and expiratory positive pleural pressure may have increased venous return, decreased pulmonary vascular resistance and lessened the compression of the left ventricle by the overfilled right ventricle.29 As there was a close association between faster QT kinetics and reductions in τ-
Other potential mechanisms for the faster on-exercise dynamics of QT and improved muscle oxygenation are related to the pharmacological properties of the bronchodilators. Although the limited available evidence suggests that inhaled bronchodilators have few haemodynamic effects during exercise in patients with COPD,6 28 their role in modulating skeletal muscle blood flow at the exercise transient in animals is still controversial.31 Additional studies, therefore, are warranted to address this specific issue in patients with COPD.
Interestingly, Δ[HHb] remained lower during steady-state exercise after the inhalation of bronchodilators (figure 3) despite no significant increases in QT or Spo2 (table 2). This finding raises the intriguing hypothesis that alleviation of the respiratory muscle work with bronchodilators may have redirected a fraction of the QT from these muscles back to the appendicular muscles. In fact, we previously reported that respiratory muscle unloading by proportional assisted ventilation increased microvascular QO2 at the same QT, suggesting improved perfusion due to blood flow redistribution from respiratory to working peripheral muscles.18 Further studies are needed to apportion the role of lower operating lung volumes and improved muscle oxygenation in enhancing exercise tolerance in patients with COPD.
Study limitations
Constant work rate exercise tests at 70–80% peak have been recognised as the most sensitive testing modality to unravel the functional benefits of bronchodilators.32 However, our findings may not be relevant to milder exercise intensities where lower ventilatory requirements may decrease, or even abolish, the beneficial effects of bronchodilators on muscle deoxygenation. We also recognise that the use of cycling instead of walking may have contributed to magnify the positive effects of bronchodilation on exercise tolerance, as contractile fatigue33 and the sense of leg effort34 are more relevant contributors to decrease exercise capacity in the former modality. It should also be acknowledged that our non-hypercapnic patients with advanced COPD were severely hyperinflated and they presented with substantial reductions in DLCO (table 1)—that is, a disease profile more compatible with the emphysematous subtype. Consequently, our results should be cautiously extrapolated to other COPD phenotypes. Finally, most of the correlation coefficients had wide confidence intervals, a likely consequence of the small sample size. Therefore, it is advisable that these specific results be confirmed in larger studies.
Conclusions
The present study showed that administration of inhaled short-acting bronchodilators to reduce lung hyperinflation slowed the dynamics and reduced the amplitude of muscle deoxygenation during high-intensity cycling exercise in patients with moderate to severe COPD. Considering that these findings were associated with faster on-exercise kinetics of QT and the ‘metabolic’ phase of pulmonary
Acknowledgments
The authors would like to thank all colleagues from the Pulmonary Function and Clinical Exercise Physiology Unit (Division of Respiratory Diseases, Federal University of Sao Paulo (UNIFESP), Brazil) for their friendly collaboration. More importantly, however, they are indebted to the patients for their effort and enthusiastic cooperation throughout the study.
References
Supplementary materials
Web Only Data thx.2009.120857
Files in this Data Supplement:
Footnotes
Linked articles 135129
Funding DCB was suppported by a Doctoral Research Fellowship from Coordenadoria de Aperfeiçoamento do Pessoal de Nível Superior (CAPES), Brazil. GRC was suppported by a Postdoctoral Research Fellowship from Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), Brazil. JAN is an Investigator of the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazil. The study was supported by a Research Grant from FAPESP, Brazil.
Competing interests None.
Ethics approval This study was conducted with the approval of the Institutional Medical Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.