Article Text

Abstract
Background Many patients with the obstructive sleep apnoea syndrome (OSA) travel to the mountains for recreational and professional activities while temporarily discontinuing continuous positive airway pressure (CPAP) treatment. A study was undertaken to evaluate the hypothesis that altitude would aggravate their hypoxaemia, sleep-related breathing disturbances and impair daytime performance.
Methods Thirty-four patients with OSA of median age 62 years (IQR 57–65), median apnoea/hypopnoea index (AHI) 47.5 events/h (IQR 32.4–72.8), residing at <600 m were enrolled. A crossover trial randomised for the sequence of altitude exposure was carried out: patients spent 1 day in Zurich (490 m) and 4 days in the Swiss Alps at 1860 m and 2590 m (2 days each) during which continuous positive airway pressure was discontinued. Daily evaluations included polysomnography, symptom questionnaires, physical examination and driving simulator tests.
Results Polysomnography revealed median oxygen saturations at 490 m and in the first and second nights at 1860 and 2590 m, respectively, of 94%, 90%, 90%, 86% and 87% (p<0.01 between altitudes). Corresponding median AHI were 47.5, 85.1, 74.6, 90.0 and 90.9 events/h (p<0.01 between altitudes) with ratios of central to obstructive events of 0.1, 0.8, 1.0, 1.9 and 1.9 (p<0.01 between altitudes). Tracking performance during simulated driving was significantly impaired at 2590 m compared with 490 m. Systolic blood pressure and cardiac arrhythmias were increased at altitude.
Conclusions Altitude exposure in untreated patients with OSA aggravates hypoxaemia, increases sleep-related breathing disturbances due to frequent central apnoeas/hypopnoeas, impairs driving simulator performance and induces cardiovascular stress. These findings have implications for counselling and treating patients with OSA planning to travel to high altitude.
ClinicalTrials.gov identifier NCT00514826.
- Hypoxia
- sleep apnoea
- control of breathing
- periodic breathing
- altitude
Statistics from Altmetric.com
Introduction
The obstructive sleep apnoea syndrome (OSA) is caused by repetitive collapse of the upper airway during sleep, provoking apnoeas/hypopnoeas associated with oxygen desaturations and sleep disruption.1 Excessive daytime sleepiness, loss of concentration and other symptoms considerably impair the quality of life of patients with OSA, and they are at increased risk of causing traffic accidents2 and suffering from cardiovascular disease.3 At least 5–10% of the adult population are affected to some extent.4 Nocturnal application of continuous positive airway pressure (CPAP) via a mask is currently the most effective treatment. It improves breathing disturbances, sleep quality and daytime symptoms.
Worldwide, a large number of individuals residing at low altitude travel to higher altitudes for work and recreational activities. In various mountain areas including the Alps, the Rocky Mountains and the Andes, settlements are located at altitudes between 1000 and 3000 m, and certain towns, lodges and mountain huts are situated at even higher elevations. High altitude periodic breathing associated with sleep disturbance and altitude-related illness such as acute mountain sickness and high altitude cerebral and pulmonary oedema may affect unacclimatised healthy lowlanders when travelling to high altitudes.5 Whether altitude exposure has similar or even more unfavorable consequences in patients with OSA is largely unknown although, because of the high prevalence of the disorder, many are expected to travel to altitude. Based on pathophysiological considerations and uncontrolled observations in a small number of patients, there have been concerns that a stay at altitude might aggravate sleep-related breathing disturbances in patients with OSA and induce central apnoea,6 7 but more robust evidence would be desirable as a basis for counselling and treating patients with OSA travelling to altitude. A randomised controlled trial was performed to evaluate the hypothesis that exposure to moderate altitude would aggravate nocturnal hypoxaemia, sleep and breathing disturbances and impair daytime performance in patients with OSA residing at low altitude and discontinuing CPAP during a 4-day stay at altitude.
Methods
Patients
Patients with OSA on CPAP therapy were invited to participate in the study by flyers distributed at the University Hospital of Zurich and the Zurich Lung League. Patients aged >20 years living at an altitude below 600 m were considered for participation if a prior diagnosis of OSA was documented by medical records and history confirming excessive sleepiness and an apnoea/hypopnoea index (AHI) >20/h before initiation of CPAP treatment. Study inclusion further required >15 oxygen desaturations/h (>3% dips) during an ambulatory pulse oximetry (PULSOX 300i, Konica Minolta, Osaka, Japan) performed during the last of four nights of CPAP withdrawal that allowed sleep-disordered breathing to return to near the untreated level.8 9 Patients also had to have an AHI >10/h with predominant obstructive apnoea/hypopnoea during polysomnography at low altitude (Zurich, 490 m). The following conditions excluded study admission: unstable cardiovascular disease, any lung disease, internal medical, neurological or psychiatric disease thought to interfere with sleep quality, chronic rhinitis, previous upper airway surgery, use of medication that interferes with ventilation or sleep (acetazolamide, benzodiazepines, opioids).
Protocol
A randomised controlled crossover trial was performed to evaluate the effects of altitude on untreated OSA. For logistic reasons, during the study period from July to October 2007 a total number of 40 time slots were available that allowed 40 patients to be allocated to two different sequences of interventions and evaluations (A and B) according to a balanced block design. In order to control for a potential order effect, 20 sequence A (starting with low altitude studies and ending with high altitude studies) and 20 sequence B (starting with high altitude studies and ending with low altitude studies) were available and allocated to time slots at random (figure 1). Details of the sequences and the fact that selecting any particular time slot determined the sequence were concealed from patients until allocation was complete. Randomisation was achieved by letting patients register for one of the available time slots according to their preference (without being aware of the corresponding sequence) until all slots were filled.
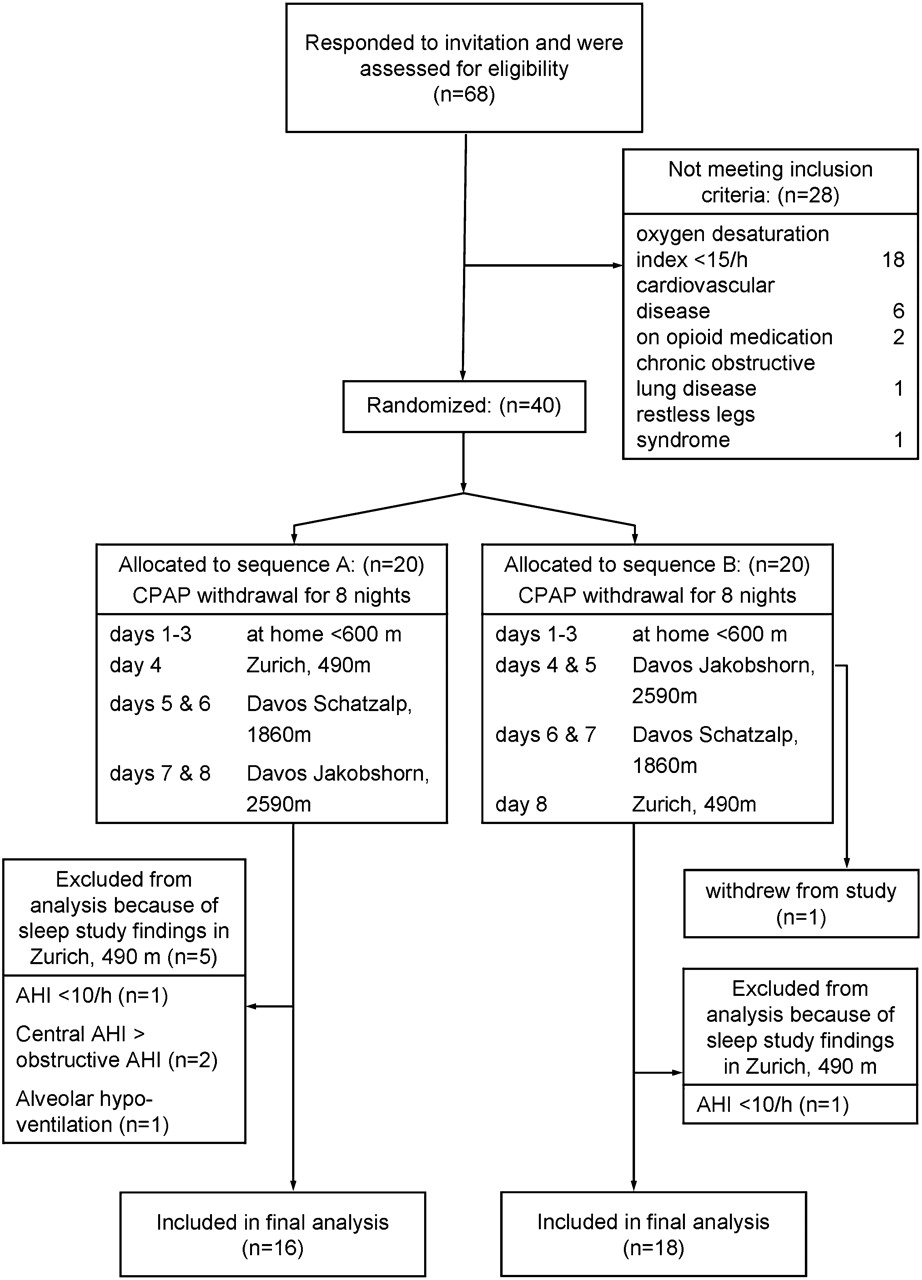
Study flow chart. AHI, apnoea/hypopnoea index; CPAP, continuous positive airway pressure.
Patients discontinued CPAP for a total of eight nights. Days 1–3 were spent at home (<600 m) while the effect of CPAP was washed out. Patients assigned to sequence A spent day 4 in Zurich (490 m, 1608 ft, barometric pressure (PB) 717 Torr), days 5–6 in Davos Schatzalp (1860 m, 6103 ft, PB 607 Torr) and days 7–8 in Davos Jakobshorn (2590 m, 8498 ft, PB 554 Torr). Patients assigned to sequence B spent days 1–3 at home, days 4–5 in Davos Jakobshorn, days 6–7 in Davos Schatzalp and day 8 in Zurich (figure 1). Transfers between Zurich and Davos, a village in the Swiss Alps, were by a 2.5 h train ride and between Davos train station and Schatzalp and Jakobshorn, respectively, by cable car. Patients spent nights in sleep laboratories at the study locations.
Outcomes
Examinations after waking up in the morning included pulse oximetry, body weight and sphygmomanometric blood pressure. Acute mountain sickness was assessed by the Lake Louise protocol10 which evaluates headaches, gastrointestinal upset, fatigue/weakness, dizziness/light-headedness, difficulty sleeping and peripheral oedema, tachypnoea, altered mental status and ataxia. The score ranges from 0 to 24 points with increasing severity of acute mountain sickness. Sleepiness was assessed by the Karolinska Sleepiness Scale11 ranging from 1 (very awake) to 9 (very tired). During a 30 min test drive with the Divided Attention Driving Simulator, the tracking error (deviation from centre line) and reaction time were recorded.12
Polysomnography was performed from approximately 22:00 h to 06:00 h according to standard techniques13 (Alice5, Respironics AG, Zofingen, Switzerland). Derivations included electroencephalogram (EEG) and electro-oculogram (EOG) leads, submental and bilateral anterior tibial electgromyogram (EMG), pulse oximetry, calibrated respiratory inductive plethysmography,14 nasal prong pressure recordings,15 bilateral diaphragmatic surface EMG,16 end-tidal and transcutaneous carbon dioxide tension (Ptcco2).17 18 Sleep stages and arousals were scored.19 20 Apnoea/hypopnoea was defined as a reduction in the inductive plethysmographic sum signal or the nasal pressure swings to <50% of the preceding 2 min baseline during ≥10 s.15 21 Transient reductions in breathing amplitude to <50% baseline for 5–10 s were also scored as apnoeas/hypopnoeas if they occurred as part of a periodic breathing pattern with hyperventilation alternating with central apnoeas/hypopnoeas for at least three consecutive cycles.22 Obstructive apnoeas/hypopnoeas were identified by rib cage and abdominal asynchrony and persistent or increasing diaphragmatic EMG activity (figure 2). Central apnoeas/hypopnoeas were identified by absent rib cage-abdominal asynchrony, no signs of inspiratory flow limitation (no flattening of nasal pressure contour) and reduced or absent diaphragmatic EMG activity. The AHI and the oxygen desaturation index (>3% dips) were computed as the number of events per hour of sleep. The sleep study analysts were blinded to the clinical data.

Polysomnographic recordings obtained in a representative patient during NREM sleep stage II at Zurich (490 m) and at Davos Jakobshorn (2590 m). At 490 m, intermittent absence of nasal pressure swings with paradoxical rib cage and abdominal excursions and persistent diaphragmatic EMG activity during events indicate that apnoeas are obstructive. At 2590 m, the intermittent absence of rib cage abdominal motion and diaphragmatic EMG activity indicates that apnoeas are central. Traces are a central EEG derivation (C3A2), left and right EOG (LEOG, REOG), submental EMG, nasal pressure swings (Pnas), inductive plethysmographic sum, rib cage and abdominal volume curves, left and right diaphragmatic EMG (EMGdiaL, EMGdiaR), oxygen saturation by pulse oximetry (Spo2) and heart rate (HR).
Data analysis
Data are summarised as medians and interquartile ranges. The effects of altitude and time at any altitude were evaluated by Friedman ANOVA followed by Wilcoxon matched pairs tests if ANOVA indicated a significant overall effect. To test the hypothesis that outcomes at altitude (ie, at 1860 m and 2590 m, days 1 and 2, respectively) differed from those at 490 m, we planned to perform four comparisons. To account for this, we assumed statistical significance at p<0.01 (ie, we performed a Bonferroni correction by factor 5 rather than 4 to be conservative). In additional exploratory comparisons between data from altitudes 1860 m and 2590 m, we adjusted the statistical significance of the p value from 0.05 by a factor of 10 to 0.005 (10 possible comparisons between data from all three altitudes and days 1 and 2). The primary outcomes were oxygen saturation and AHI, and secondary outcomes were sleep quality and vigilance, symptoms and physical findings. Clinically relevant differences were assumed to be 2% (SD 2%) for oxygen saturation and 10/h (SD 15/h) for the AHI. Power calculation indicated a minimal sample size of 29 to detect clinically relevant differences in primary outcomes with a power of 80% (α=0.01). To account for potential drop-outs, our aim was to recruit 40 patients.
Results
Patients
Figure 1 illustrates the patient flow. Of 68 patients who applied to participate in the study, 40 met the inclusion criteria and were randomised. One patient withdrew after one night at Jakobshorn because of lack of motivation. Data from five patients had to be excluded according to predefined criteria because baseline polysomnography at low altitude (Zurich) revealed an obstructive AHI <10/h in two, predominant central apnoeas/hypopnoeas in two and alveolar hypoventilation in one. Data from 34 patients (32 men, 2 women) were available for analysis. Median (IQR) age was 62 (57–65) years and body mass index was 33.7 (27.3–38.1) kg/m2. Patients had been on CPAP treatment for 41 (20–56) months. Comorbidities included arterial hypertension in 68% and diabetes mellitus in 15% of subjects; 38% were receiving ACE inhibitors/angiotensin II antagonists, 35% diuretics, 24% β blockers and 18% calcium channel blockers. No serious adverse events requiring medical treatment occurred.
Sleep studies
The sleep study results are summarised in table 1 and data on nocturnal ventilation, oxygen saturation and heart rate are shown in table 2. A representative recording is shown in figure 2. A comparison of the data from subjects undergoing sequences A and B did not reveal significant differences in oxygen saturation, AHI, percentage slow wave sleep and sleep efficiency, so the data from the two groups are presented together. Compared with values recorded at 490 m, oxygen saturation was significantly reduced at 1860 m and even more so at 2590 m, particularly during REM sleep. Transcutaneous Pco2 was highest at 490 m during REM sleep and lowest at 2590 m during NREM sleep. Studies at 490 m revealed severe OSA and only occasional central apnoeas/hypopnoeas according to inclusion criteria. On the first and second day at 1860 and 2590 m, respectively, the AHI increased significantly to medians of 147%, 141% and 166%, 167% of the 490 m baseline value. This was related to the emergence of frequent central apnoeas/hypopnoeas during NREM sleep while obstructive apnoeas/hypopnoeas persisted (figure 3). Sleep quality worsened significantly at altitude as reflected in an increased arousal index, reduced sleep efficiency and slow wave sleep (NREM stages III and IV) at 2590 m. The number of arousals was significantly correlated with the AHI at all altitudes (at 490 m: Spearman R=0.77; 1860 m, day 1: R=0.70; 1860 m, day 2: R=0.77; 2590 m, day 1: R=0.68; 2590 m, day 2: R=0.77; p<0.01 in all instances). Compared with 490 m, the heart rate and the number of premature beats were significantly increased at altitude.
Sleep studies (n=32)
Nocturnal ventilation, oxygen saturation and heart rate (n=34)

Sleep-related breathing disturbances at 490 m and in the first and second night at 1680 m and 2590 m, respectively. The bars and horizontal lines represent median values and quartile ranges of obstructive and central apnoea/hypopnoea indices at the different locations. The upper panel represents events during NREM sleep and the lower panel corresponding values during REM sleep. At higher altitudes, the total apnoea/hypopnoea index increased significantly, related to the emergence of central apnoea/hypopnoea during NREM sleep. *p<0.01 vs 490 m; **p<0.01 vs 490 m and vs 1860 m.
Comparisons of sleep studies on the first versus the second night at corresponding altitude revealed no effect of acclimatisation on oxygen saturation and transcutaneous Pco2.
Symptoms and daytime findings
In the morning the Karolinski Sleepiness Scale indicated that patients felt moderately sleepy (table 3). They reported moderate symptoms of acute mountain sickness at altitude but the Lake Louise score was also increased at 490 m. None of the patients had symptoms or signs of high altitude pulmonary oedema. There was an increase in weight at 2590 m compared with 490 and 1860 m, and this was associated with ankle oedema. Systolic blood pressure was increased at 1860 m and 2590 m above values at 490 m (table 3). In two patients antihypertensive medication needed to be adapted at 2590 m because of an excessive rise in blood pressure. Driving simulator tests revealed significantly increased tracking errors at 2590 m compared with the lower altitudes (figure 4).
Daytime evaluation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Performance during a divided attention driving simulator test in a patient with obstructive sleep apnoea at 490 m and at 2590 m. During the 30 min test drive the patient had to stay in the centre of the road displayed on a computer screen by using a steering wheel. At the same time he had to check numbers appearing in the four corners of the screen. As soon as the number 2 appeared he had to press a button. The computer recorded the distance from the road centre line and the elapsed time until the number 2 was confirmed by pressing the button. In the upper panel the plot shows results obtained at 490 m. The average response time to the number 2 was 2.6 s (each response is shown as a circle in the upper panel). The patient was able to stay near the centre line (lower panel). In contrast, at 2590 m, the patient missed the number 2 several times (circles at the upper limit of the panel labelled reaction time) and he had great difficulties staying on the road. In the lowest panel, his driving path shows large fluctuations, frequently crossing the lateral boundaries of the road (two horizontal lines). Deviation from the center line is expressed in arbitrary units (a.u.).
Discussion
We performed a randomised controlled crossover trial in patients with moderate to severe OSA during temporary CPAP discontinuation to evaluate the effects of a 4-day stay at moderate altitudes (1860 m and 2590 m) on sleep, breathing and daytime performance. The main findings were a progressive reduction in nocturnal oxygen saturation associated with hyperventilation and a major increase in the AHI, particularly at the highest altitude, due to frequent central apnoeas/hypopnoeas while obstructive events persisted. Correspondingly, sleep quality and driving simulator performance were impaired at altitude. Further consequences of altitude exposure were an increased prevalence of nocturnal cardiac arrhythmias, a significant rise in heart rate and in systolic blood pressure and a weight gain with peripheral oedema. We conclude that a stay at moderate altitude in untreated patients with OSA is associated with unfavorable health effects.
In healthy subjects, hypobaric hypoxia at altitudes >2000 m induces periodic breathing with central apnoea/hypopnoea.23–25 Breathing instability is related to hypoxic stimulation of ventilation resulting in a reduced CO2 reserve—that is, an eupnoeic Pco2 close to the apnoea threshold promoting apnoea at a minor rise in ventilation because enhanced chemosensitivity causes a ventilatory overshoot.26 Data on breathing patterns and sleep in patients with OSA at altitude are scant. During exposure to a simulated altitude of 2750 m (Fio2 16.05% at 610 m, PB 700 mm Hg), five patients with OSA had an increase in central apnoeas and a reduction in obstructive apnoeas compared with studies in normoxia at sea level.6 In 11 patients with OSA undergoing repeated sleep studies at an altitude >2400 m, at 1370 m and at sea level (five patients), the AHI decreased with descent in altitude due to a reduction in central apnoeas.7 Our randomised trial corroborates and extends these observational studies by confirming a dose-response relationship between progressive hypoxia at increasing altitude, decreasing transcutaneous Pco2 reflecting more pronounced hyperventilation and emergence of frequent central apnoeas/hypopnoeas. The number of events scored as central might have been even higher if we had not applied stringent criteria requiring absence of signs of inspiratory flow limitation, perfect synchronisation of rib cage-abdominal motion recorded by calibrated inductive plethysmography and a reduced or absent diaphragmatic surface EMG activity. This conservative definition excluded central and mixed events with partial upper airway occlusion. The increase in central apnoea index at altitude occurred predominantly during NREM sleep but rarely during REM sleep (figure 3). This was consistent with a greater increase in hypoxic and hypercapnic ventilatory drive in NREM sleep compared with REM sleep at altitude25 and a widened CO2 reserve and/or absence of a post-hyperventilation-induced apnoeic threshold in REM sleep.27
In our study there was no significant change in the obstructive AHI at altitude (table 2). Presumably, factors contributing to upper airway patency during hypoxia such as chemical stimulation of dilator muscles were offset by factors promoting airway collapse such as stimulation of ventilatory pump muscles that increase the upper airway transmural pressure gradient during vigorous inspiratory efforts.28 29 A shorter duration of obstructive apnoea/hypopnoea at altitude (table 2) is consistent with a lower arousal threshold and/or a lower recruitment threshold of upper airway dilator muscles in hypoxia compared with normoxia.29
Sleep fragmentation and a reduced amount of slow wave sleep have been reported previously in healthy subjects at altitude.30–32 Correspondingly, we observed that sleep quality in patients with OSA was impaired at altitude, as reflected in a reduction in sleep efficiency and slow wave sleep and frequent arousals (table 1). Correlation analysis indicated that 46–59% of the variation in the arousal index was explained by the AHI, suggesting a significant contribution of breathing disturbances to sleep fragmentation although other factors might additionally have impaired sleep quality in hypoxia.32 In five patients with OSA studied at a simulated altitude of 2750 m (isobaric hypoxia),6 no significant changes in sleep stages compared with sea level studies were observed, possibly related to the small sample size.
Questionnaire evaluation indicated that patients perceived moderate headache, poor sleep quality and sleepiness even at low altitude (table 3), which was probably due to CPAP withdrawal. There was no clear further increase in these symptoms at altitude (table 3). We cannot exclude the possibility that the positive attitude towards a stay at altitude may have influenced the perception of altitude-related symptoms in the study participants. However, objective testing during a simulated car drive indicated reduced psychomotor vigilance at 2590 m (table 3), highlighting the potential clinical relevance of exposure to hypoxia in patients with OSA who already have cognitive dysfunction in normoxia.12
OSA is associated with cardiac arrhythmia and systemic hypertension at low altitude.3 In this study, patients had a higher prevalence of nocturnal premature beats and a rise in heart rate and systolic blood pressure at altitude (tables 2 and 3), suggesting an additional cardiovascular effect of sustained hypoxia and of the more pronounced breathing disturbances at altitude, possibly related to sympathetic activation and parasympathetic withdrawal.33 34 The weight gain we observed in association with the development of peripheral oedema (table 3) is consistent with water retention, possibly mediated by sympathetic overstimulation, rise in systemic and pulmonary artery pressure and activation of the renin-angiotensin-aldosterone system in patients with OSA with symptoms of acute mountain sickness.35
In conclusion, this randomised crossover trial in patients with OSA indicates that hypoxia, breathing and sleep disturbances are more severe at altitude and are associated with signs of cardiovascular stress and impaired driving simulator performance. The results caution against altitude exposure of untreated patients with OSA, and may help in the design of further studies evaluating the effectiveness of CPAP and other treatment modalities that might improve subjective well-being and reduce the potential risk of traffic accidents and cardiovascular complications in patients with OSA at altitude.
References
Footnotes
Funding Swiss National Science Foundation, Lung Leagues of Zurich and of Schaffhausen, Switzerland.
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics committee of the University Hospital of Zurich.
Provenance and peer review Not commissioned; externally peer reviewed.