Article Text

Abstract
BACKGROUND Asthma exacerbations contribute substantially to morbidity, and their reduction is an important therapeutic objective. In this integrated analysis the risk of asthma exacerbations was assessed during treatment with the leukotriene receptor antagonist zafirlukast.
METHODS Data were collected from all five double blind, multicentre, randomised, placebo controlled, 13 week trials of zafirlukast 20 mg twice daily performed in steroid-naive patients with mild to moderate asthma. Exacerbation data were collected prospectively during monitoring of adverse events and concomitant medication use. Pooled data were used to assess the relative risk of asthma exacerbations using three definitions: worsening of asthma leading to withdrawal from the study; requirement for additional anti-asthma therapy (excluding increased short acting β2 agonist use); and requirement for oral corticosteroid therapy.
RESULTS The proportion of patients with an asthma exacerbation leading to withdrawal was consistently lower in the group treated with zafirlukast 20 mg twice daily than in the placebo group. Overall, the risk of an asthma exacerbation requiring withdrawal from zafirlukast therapy was approximately half that of placebo (odds ratio 0.45; 95% CI 0.26 to 0.76; p = 0.003). Similar results were observed for exacerbations requiring additional control medication (odds ratio = 0.47; 95% CI 0.30 to 0.74; p = 0.001) and oral corticosteroid rescue (odds ratio = 0.53; 95% CI 0.32 to 0.86; p = 0.010).
CONCLUSIONS Zafirlukast in a dose of 20 mg twice daily reduces the risk of asthma exacerbations and the need for additional anti-asthma therapies, fulfilling an important goal of control medication in patients with mild to moderate asthma.
- asthma
- zafirlukast
- leukotriene receptor antagonist
Statistics from Altmetric.com
In clinical trials of anti-asthma treatments investigators have traditionally used measures of pulmonary function such as forced expiratory volume in one second (FEV1) or home peak expiratory flow (PEF) to characterise patient improvement. These efficacy outcome measures are surrogate measures of disease control but are useful to physicians and patients for monitoring asthma. However, the outcome measures that have the greatest effect on patients are likely to be symptom reduction and prevention of asthma exacerbations, particularly those resulting in days absent from work or school or the need for emergency treatment or admission to hospital.1The reduction of such exacerbations is increasingly recognised as an important goal of asthma control therapy.2 Consequently, exacerbations of asthma are now being used as efficacy outcome measures in clinical trials for the evaluation of new anti-asthma therapies.
At present, inhaled corticosteroids have been shown unequivocally to decrease the risk of asthma exacerbations3-7 and these drugs represent the mainstay of anti-inflammatory treatment in asthma. In addition, evidence suggests that long acting β2agonists also provide protection from asthma exacerbations.7 However, drugs that interfere with the leukotriene pathway—that is, 5-lipoxygenase inhibitors and leukotriene receptor antagonists—may also prevent or reduce the severity of asthma exacerbations. The cysteinyl leukotrienes are important mediators of acute airway obstruction in asthma8 ,9 and increased urinary levels have been observed in patients during severe exacerbations.10
Compared with placebo, the leukotriene receptor antagonist zafirlukast has been shown to improve pulmonary function, reduce daytime and night time asthma symptoms, decrease the use of β2 agonists as rescue medication, and decrease treatment failure rates.11-13 The objective of this analysis of data from all five randomised, double blind, placebo controlled, 13 week trials comparing the most widely used dosage of zafirlukast (20 mg twice daily) with placebo in steroid-naive patients with mild to moderate asthma was to determine the role of zafirlukast in reducing the risk of exacerbations that led to trial withdrawal or required additional treatment.
Methods
DATA SOURCES
We chose to integrate data from all randomised trials (all sponsored by Zeneca Pharmaceuticals, Wilmington, Delaware, USA and Zeneca Ltd, Alderley Park, UK) conducted to date that met the following criteria: design—13 week, double blind, parallel group; treatment—zafirlukast 20 mg twice daily compared with placebo; target population—steroid-naive patients with mild to moderate asthma who were appropriate for chronic asthma therapy. The data used in this integrated analysis came from the complete safety and efficacy databases which included all patients who received at least one treatment dose. Patients were recruited and studied between January 1993 and August 1996. All trials were multicentre studies; trials A, B, C, and E were conducted in North America, and trial D was a multinational study conducted in Europe. All subjects gave their written informed consent and the trials were conducted in accordance with the Declaration of Helsinki and Guidelines on Good Clinical Practice.
Trial A was a dose ranging trial comparing placebo with zafirlukast 4, 10, 20, 40 and 80 mg twice daily and 40 mg once a day.11In this analysis we included only data from subjects who received zafirlukast 20 mg twice daily or placebo. Results of the other four trials which compared zafirlukast 20 mg twice daily with placebo were reported by Fish et al 12 (B), Nathan et al 14 (C), Holgateet al 15 (D), and Nathanet al 13 (E). In all these trials the primary outcome measured was asthma symptoms.
PATIENT CHARACTERISTICS
Male and female patients, both non-smokers or ex-smokers who had not smoked for at least six months and had less than a 10 pack year history (packs/year × number of years of smoking), with a documented clinical history of asthma were eligible for recruitment. All patients were aged ⩾12 years and women of childbearing potential were required to practise an effective method of birth control throughout the trial. Trial A included only patients who were aged between 18 and 65 years, and trial D excluded patients aged more than 65 years.
In all studies patients were required to demonstrate reversible airway disease as shown by either a positive histamine or methacholine challenge test within six months of screening or a ⩾15% increase in FEV1 or PEF after use of an inhaled bronchodilator. (A positive histamine or methacholine challenge was one in which the provocative concentration that decreased the FEV1 by 20% was 8 mg/ml or the provocative dose that decreased the FEV1 by 20% was <2 mg.) Patients in trials A, B, and C were required to have an FEV1 ⩾55% of the predicted value at entry, and patients in trial E were required to have an FEV1 of 45–80% of the predicted value. The protocol of trial D did not specify entry criteria for FEV1, but patients' lung function and symptom levels had to be consistent with definitions of step 2 in international treatment guidelines.16
In trials A, B, D, and E patients were maintained on “as required” β2 agonists alone at entry to the trial. In trial C patients taking oral theophylline were permitted to enter the trial if the medication was withdrawn prior to or on entry to the one week placebo run in period before randomisation. None of the patients were using oral or inhaled corticosteroids or long acting β2agonists at entry to the trial.
Patient characteristics at the time of randomisation to double blind treatment are summarised in table 1. Patients were generally well matched between treatment groups and across trials, with similar disease profiles. Patients in trial D had slightly milder disease as shown by lower mean daytime asthma symptoms scores, fewer mean nocturnal awakenings, and higher mean percentage predicted FEV1 values. All patients in the combined data set had mild to moderately severe, persistent asthma according to the criteria defined in national and international guidelines.16-18
Characteristics of patients in each of the five multicentre trials by treatment group
DATA EXTRACTION
In all trials investigators recorded (on case report forms) health care contacts and changes in asthma treatment at the time of withdrawal or scheduled or unscheduled visits. The data from these forms were subsequently validated by data management personnel from Zeneca Pharmaceuticals and entered into computerised databases before the blind was broken.
The data sets analysed included all patients randomised to treatment with either zafirlukast (n = 972) or placebo (n = 692) from the five trials (full analysis data set or intention-to-treat approach). The 2:1 randomisation allocation in favour of zafirlukast in trial B largely explains the larger number of patients receiving zafirlukast overall.
Three analyses, corresponding to three different definitions of asthma exacerbations, were performed on these combined data. Because no standard universally accepted definition of asthma exacerbation exists, we chose those that could reliably be applied to our data set and that appeared to be most clinically relevant.
The first analysis included only asthma exacerbations that required withdrawal from the trials according to the individual trial protocols. In trials A, B, and C investigators withdrew patients if they had asthma exacerbations that required any of the following: more than one emergency room visit or hospital admission; the addition of regular inhaled corticosteroids; or a short course of rescue inhaled or oral corticosteroids. In trial D these criteria for withdrawal were expanded to include patients with worsening symptoms that were unrelieved with salbutamol as judged by the patient. In trial E the criteria for withdrawal were the same as described for studies A, B, and C except that a single seven day course of oral prednisolone was permitted without requiring the patient to be withdrawn from the study.
The second analysis of the combined data set counted patients who received prescriptions for additional anti-asthma therapy other than an increased use of short acting β2 agonist. The third analysis counted patients who required oral corticosteroid rescue therapy. In both of these analyses patients were included irrespective of whether they were withdrawn from the study.
The three different definitions of exacerbations were not mutually exclusive. All patients who required oral corticosteroid rescue therapy were also counted among the patients who received prescriptions for additional anti-asthma therapy. Each patient was counted only once in each analysis even if that patient had multiple exacerbations. The rationale for doing this was that exacerbations led to withdrawal in most cases, thereby eliminating the possibility of counting additional exacerbations. Also, the way the data were captured often made it difficult to distinguish between multiple exacerbations and multiple prescriptions of medication for the same exacerbation.
The data for the patients who required oral corticosteroid rescue therapy were stratified by baseline lung function (percentage peak flow variability and percentage predicted FEV1) to determine the effect of asthma severity on exacerbations.
STATISTICAL ANALYSIS
Analyses were performed with all trials combined using a continuity corrected Cochran-Mantel-Haenszel test adjusted for the effects of individual trials.19 ,20 p values of ⩽0.05 from this test were considered to be statistically significant. The Mantel-Haenszel test-based adjusted odds ratio estimator and corresponding 95% confidence interval (CI) were calculated to estimate the common relative risk across trials of having an asthma exacerbation. To evaluate the consistency of treatment effect across trials, the Breslow-Day test of homogeneity of odds ratios was calculated for each definition of asthma exacerbation.20In addition, for each trial a χ2 test of independence was performed and the odds ratio and Mantel-Haenszel test-based 95% CI of the odds ratio were calculated.
Results
The group treated with zafirlukast 20 mg twice daily had a lower risk of experiencing exacerbations leading to trial withdrawal than the placebo group. Overall, 38 patients (5.5%) in the placebo group and 26 patients (2.7%) in the zafirlukast group were withdrawn because of an asthma exacerbation (odds ratio = 0.45; 95% CI 0.26 to 0.76; p = 0.003; table 2). This result was consistent across all five trials, as suggested by the non-significant Breslow-Day test of homogeneity of odds ratios (p = 0.833). In the largest of the five trials (trial B) the difference between treatments was also significant (odds ratio = 0.47; 95% CI 0.23 to 0.93; p = 0.031).
Integrated analysis comparing the number of patients who had asthma exacerbations according to three definitions among patients who received zafirlukast 20 mg twice daily or placebo
The results of the second analysis, which used the definition of an exacerbation as a requirement for additional anti-asthma therapy (other than increased use of short acting β2 agonist) were that 33 (3.4%) of the group receiving zafirlukast 20 mg twice daily needed additional anti-asthma therapy compared with 53 (7.7%) of the placebo group. The difference between groups in risk of requiring additional anti-asthma treatment was statistically significant (odds ratio = 0.47; 95% CI 0.30 to 0.74; p = 0.001) and consistent across trials (p = 0.477, Breslow-Day test).
The results of the analysis for the need for oral corticosteroids are shown in fig 1 and table 2. Most of the patients (69%) who had asthma exacerbations leading to withdrawal from trials A, B, C, and D required short bursts of oral corticosteroids. Trial E had the lowest number of exacerbations leading to withdrawal (two (0.9%) in the zafirlukast group and six (2.7%) in the placebo group) but the highest numbers of patients who required treatment with oral corticosteroids (12 (5.2% in the zafirlukast group and 21 (9.4%) in the placebo group). This difference is explained by the fact that patients in trial E may have had more severe disease than the patients in the other trials, and the protocol allowed them to remain in the trial after a single short course of oral corticosteroids. Forty five patients (6.5%) receiving placebo compared with 31 (3.2%) receiving zafirlukast 20 mg twice daily required oral corticosteroid rescue (odds ratio = 0.53; 95% CI 0.32 to 0.86; p = 0.010). In all but the smallest of the five trials (trial A) the percentage of patients requiring oral corticosteroid rescues was less in the zafirlukast group than in the placebo group. (In trial A only two patients in each treatment group required oral corticosteroids.) Thus, there was little evidence that this treatment effect was not consistent across trials (p = 0.702, Breslow-Day test).

Odds ratio (with 95% confidence intervals) by trial and overall for asthma exacerbations defined as the need for oral corticosteroids.
In total, 102 patients had an asthma exacerbation that met at least one of the three definitions (39 (4.0%) on zafirlukast, 63 (9.1%) on placebo). Eighty six (84.3%) of these patients required the addition of another asthma therapy which included oral corticosteroids in 76 of 86 cases (88.4%). Other asthma therapies included inhaled corticosteroids in 19 patients (22.1%) and cromones or theophylline in 16 (18.6%); some patients received more than one medication. Most of the patients who required additional asthma medications (n = 48, 55.8%) were withdrawn for worsening asthma, which was consistent with the trial protocols. Only 16 patients (six zafirlukast, 10 placebo) were withdrawn for worsening asthma without having received a prescription for an additional asthma medication.
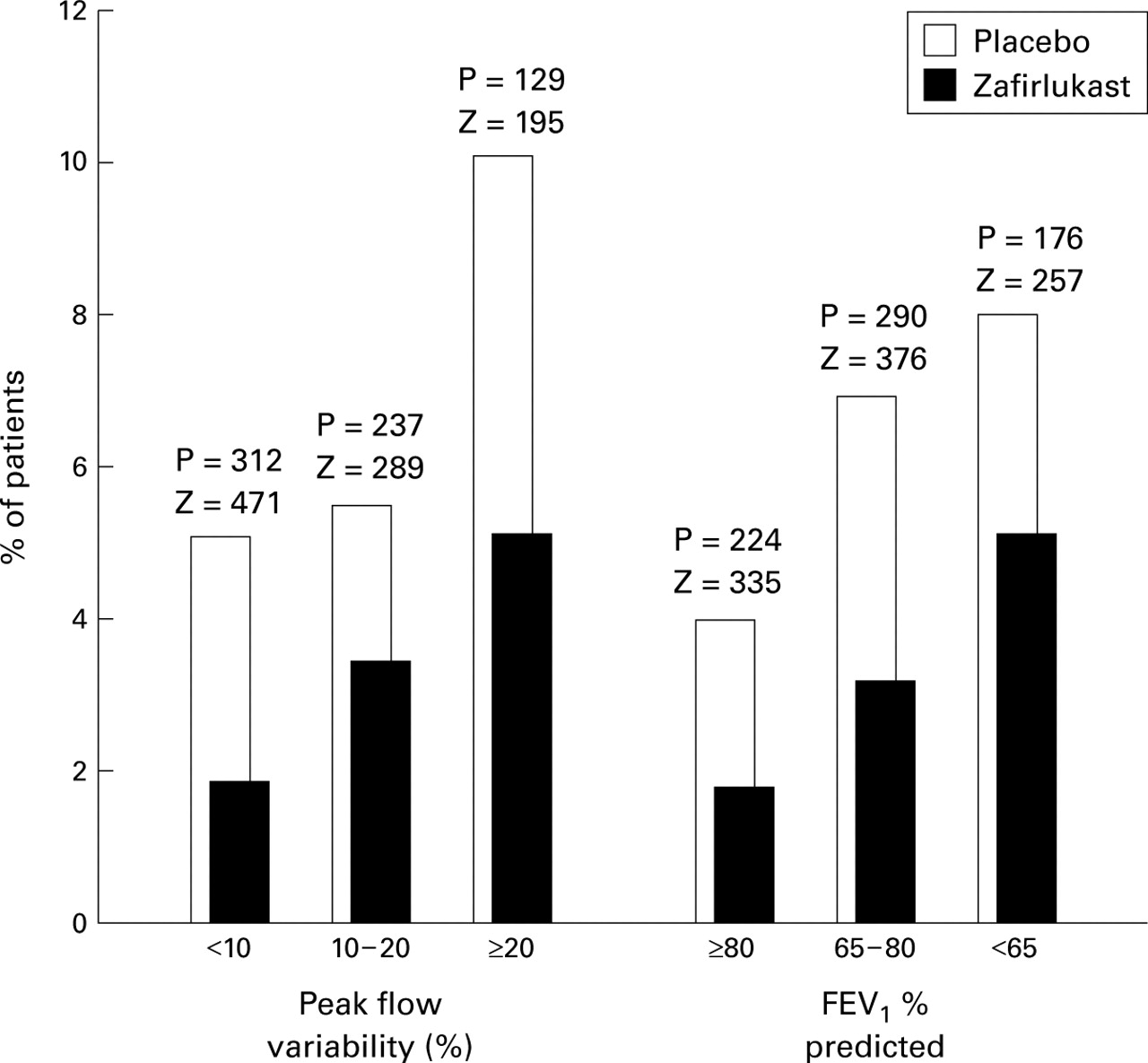
Figure 2 shows the results of stratifying the number of patients who required oral corticosteroid rescue by baseline asthma severity, characterised by percentage predicted FEV1 or peak flow variability. The percentage of patients experiencing exacerbations increased with increasing asthma severity; however, zafirlukast provided a similar degree of protection across all asthma severities.

{kind=link}
{kind=link}
Percentage of patients within each stratified group (stratification by baseline % peak flow variability* or percentage predicted FEV1) who had asthma exacerbations defined as the need for oral corticosteroids. Numbers above each set of columns are the numbers of patients at risk in each stratified group (Z = zafirlukast, P = placebo). Odds ratios and 95% CI for peak flow variability subgroups were: <10%, OR = 0.40, 95% CI 0.17 to 0.93; 10–20%, OR = 0.70, 95% CI 0.21 to 2.34; ⩾20%, OR = 0.56, 95% CI 0.20 to 1.56. Odds ratios and 95% CI for FEV1 percentage predicted subgroups were: <65%, OR = 0.70, 95% CI 0.24 to 2.02; 65–80%, OR = 0.48, 95% CI 0.22 to 1.05; ⩾80%, OR = 0.43, 95% CI 0.12 to 1.55). *See footnote to table 1.
A total of 167 patients (17.2%) in the zafirlukast group and 139 (20.1%) in the placebo group withdrew from the trials before completion. Other than asthma exacerbations, the reasons for withdrawal were similar in the two groups. Twenty one patients (2.2%) in the zafirlukast group and 16 (2.3%) in the placebo group withdrew because of adverse events unrelated to asthma and 12.3% of patients in each group withdrew because of other reasons such as protocol violations, failure to return, and refusal to continue.
Discussion
Exacerbations of asthma causing unscheduled asthma care, such as admission to hospital or the need to attend a primary care physician or visit an accident and emergency department, are responsible for considerable morbidity and a substantial proportion of the costs of asthma care.21 Prevention of asthma exacerbations or improvement of disease control is therefore an important objective in the treatment of chronic asthma.1 ,2 The results of our analysis of the integrated databases of five trials in mild to moderate steroid-naive asthmatics indicate that, compared with placebo, zafirlukast 20 mg twice daily significantly reduced and more than halved the risk of asthma exacerbations leading to withdrawal from clinical trials or the need for further treatment interventions including oral corticosteroid rescue.
The analysis method we used is a widely accepted way to reach a general conclusion about a particular question which had not been adequately addressed in individual studies due to a lack of statistical power.22 In our trials with patients who had mild to moderate asthma the incidence of asthma exacerbations was low, as shown by the fact that only 5.5% of patients receiving placebo withdrew because of asthma exacerbation during the 13 week trial period. By analysing all the data from trials of similar design, we were able to estimate the effect of zafirlukast in a dose of 20 mg twice daily on the risk of exacerbations in patients with mild to moderate asthma. By using the complete 13 week study data set we were able to eliminate publication bias, increase the accuracy of the estimate, and apply different definitions for additional analyses. Although the trials had some minor differences in subject selection and study design, the results were remarkably homogenous. This analysis supports the results of a previous six week trial in patients with more severe asthma (mean FEV1 66% predicted) in which 2% of patients treated with zafirlukast 20 mg twice daily withdrew because of failure of asthma treatment compared with 10% of patients receiving placebo.11
Exacerbations resulting in withdrawal were not analysed as the primary efficacy end point in any of the five trials. However, these data were collected prospectively and investigators and patients were blinded as to treatment. The investigators used their own discretion and judgement as they would have in a routine clinical practice and were not led by preset symptom or pulmonary function limits to make these clinical judgements. Fabbri et al 5 used similar exacerbation data to demonstrate a lower exacerbation rate in patients treated with fluticasone propionate than in those treated with beclomethasone dipropionate in moderate to severe steroid-dependent asthma.
We also defined asthma exacerbations as the need to treat patients with additional asthma therapy including oral corticosteroids. This definition of asthma exacerbations has been employed in several studies that have established the usefulness of inhaled corticosteroid therapy.4 ,5 In the Formoterol and Corticosteroids Establishing Therapy (FACET) trial7 one of the definitions of severe exacerbations used was the requirement for oral corticosteroids. Additionally, the 5-lipoxygenase inhibitor zileuton and the leukotriene receptor antagonist montelukast have been shown to decrease asthma exacerbations as defined by the need for corticosteroid treatment. In a 13 week placebo controlled trial a retrospective analysis of a subpopulation of patients with more severe asthma (FEV1 <50% predicted) indicated that zileuton significantly reduced the need for oral corticosteroid therapy compared with placebo.23 In a further prospective six month trial24 zileuton 600 mg four times daily significantly decreased the need for oral corticosteroid therapy by more than half compared with placebo in patients whose baseline FEV1 was 62% of predicted. In a large placebo controlled trial in patients with a mean baseline FEV1 of 67% predicted, 6.9% of the patients in the group receiving 10 mg montelukast required oral corticosteroid rescues compared with 9.6% of patients in the placebo group, although the difference was not statistically significant.25 More recently, montelukast and beclomethasone dipropionate were compared with placebo in 895 patients whose mean baseline FEV1 was 65% predicted.26The need for rescue oral corticosteroids or an unscheduled physician or hospital visit was significantly decreased by 63% in the beclomethasone group and 43% in the montelukast group.
Although these trials employed definitions of asthma exacerbations that were similar to ours, the rate of exacerbations for the placebo groups in these trials was higher than that in our trial population in which the patients had milder asthma (mean FEV1 75% predicted). Nevertheless, with the increased statistical power afforded by the integrated analysis, we were able to demonstrate a statistically significant approximate halving in the risk of having an exacerbation requiring oral corticosteroid therapy for patients treated with zafirlukast 20 mg twice daily. The robustness of the estimate of effect with zafirlukast compared with placebo is further supported by the consistency of effect across the subgroups of patients stratified by severity of airway obstruction and degree of airway instability at baseline.
Wider definitions of asthma exacerbations other than those we used have included prospectively defined increases in symptoms or β2 agonist use or a decrease in pulmonary function occurring on at least two days.7 ,27 ,28 Noonanet al 28 reported that fewer patients (47.1%) in a combined group of patients treated with montelukast 10 or 50 mg per day had such exacerbations compared with placebo (69.6%), and Reiss et al 25 reported a statistically significant 31% reduction in exacerbation days with montelukast 10 mg per day compared with placebo. In these studies asthma exacerbations were defined by days with increased symptoms or decreased lung function. Using such definitions, asthma exacerbations can be found to be more prevalent, thereby increasing the statistical power of individual studies to detect the beneficial effects of treatment. However, these definitions tend to define relatively mild exacerbations and their relationship to exacerbations of importance in clinical practice is not clear.
Our analyses confirm that zafirlukast monotherapy in steroid-naive asthmatic patients can reduce the risk of asthma exacerbations by half compared with placebo, regardless of the definition of exacerbation that is chosen. Further studies will be needed to confirm these results in patients with more severe asthma and in patients who are receiving concomitant asthma treatments. The FACET trial7 showed that, in patients receiving 200 and 800 μg/day inhaled budesonide, the addition of the long acting β2 agonist formoterol reduced severe asthma exacerbations by 26% compared with placebo. In a four week study of patients with persistent asthma, 80% of whom were on concurrent corticosteroids, zafirlukast and the long acting β2 agonist salmeterol had a similar effect on exacerbations.29 Further studies are needed to evaluate the effectiveness of zafirlukast compared with long acting β2 agonists and other established treatment.
In conclusion, the ability of the leukotriene receptor antagonist zafirlukast to halve the risk of having asthma exacerbations that require further interventions by clinicians represents an important clinical property of this drug. Compared with placebo, zafirlukast 20 mg twice daily reduces the incidence of asthma exacerbations leading to withdrawal from treatment and the need for rescue oral corticosteroid therapy in patients with mild to moderate asthma.
Acknowledgments
We wish to thank Barbara Murray for assistance with writing and Susy Hassall for technical assistance.
References
Footnotes
Funding: Research funding was supplied through research grants from Zeneca Pharmaceuticals, USA and Zeneca Limited, UK.