Article Text

Abstract
BACKGROUND An ecological analysis was conducted of the relationship between tuberculosis notification rates and the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema in 85 centres from 23 countries in which standardised data are available. These essentially comprised countries in Europe as well as the USA, Canada, Australia, and New Zealand.
METHODS Tuberculosis notification rates were obtained from the World Health Organization. Data on the prevalence of symptoms of asthma, rhinitis, and eczema in 235 477 children aged 13–14 years were based on the responses to the written and video questionnaires from the International Study of Asthma and Allergies in Childhood (ISAAC). The analysis was adjusted for gross national product (GNP) as an estimate of the level of affluence.
RESULTS Tuberculosis notification rates were significantly inversely associated with the lifetime prevalence of wheeze and asthma and the 12 month period prevalence of wheeze at rest as assessed by the video questionnaire. An increase in the tuberculosis notification rates of 25 per 100 000 was associated with an absolute decrease in the prevalence of wheeze ever of 4.7%. Symptoms of allergic rhinoconjunctivitis in the past 12 months were inversely associated with tuberculosis notification rates, but there were no other significant associations with other ISAAC questions on allergic rhinoconjunctivitis or atopic eczema.
CONCLUSIONS These findings are consistent with recent experimental evidence which suggests that exposure to Mycobacterium tuberculosis may reduce the risk of developing asthma.
- tuberculosis
- atopy
- asthma
Statistics from Altmetric.com
The reasons for the increase in the prevalence of asthma and other atopic disorders such as eczema and allergic rhinitis1 and the international patterns of the prevalence of these diseases2 are largely unknown. In particular, they cannot be explained by the established putative risk factors such as allergen exposure and air pollution which do not appear to be strongly related to the underlying population prevalence.2-5 This has led to consideration of factors that may programme the initial susceptibility to asthma and/or atopy which have changed in temporal association with the increasing trends in prevalence worldwide, are consistent with international prevalence patterns, and for which biological plausibility exists with respect to an underlying mechanism.
One such hypothesis is that the lack of exposure in early childhood to infections such as tuberculosis, measles, and diphtheria may increase the risk of developing atopic disorders such as asthma.6 ,7 Interest has focused particularly on the role of Mycobacterium tuberculosis which is known to induce Th1 type immune responses, suppressing the development of Th2 type immune responses that are characteristic of atopic disorders.8-10 Epidemiological evidence for the association of this immunological response with a reduced risk of developing asthma comes from the study by Shirakawaet al 11 who reported that, among Japanese schoolchildren aged 12–13 years, asthmatic symptoms were one half to one third as likely in positive tuberculin responders as in negative responders, and that remission of atopic symptoms between the ages of seven and 12 years was 6–9 times more likely in positive tuberculin responders. The positive tuberculin responders had significantly lower levels of the Th2 cytokines interleukin (IL)-4, IL-10, and IL-13 and higher levels of the Th1 cytokine interferon (IFN)-γ. The interpretation of these findings has been debated intensively. The inverse association between allergic status and tuberculin reactivity may simply reflect the imbalance of Th1/Th2 responsiveness characteristic of atopic individuals who have been shown to express smaller delayed type hypersensitivity skin reactions to recall antigens than non-atopic subjects.12 This imbalance may relate to genetic or other constitutional factors rather than to exposure to mycobacteria. However, the alternative hypothesis which suggests that exposure to M tuberculosisreduces the risk of developing asthma and/or atopy is equally conceivable. The reduction in the incidence of tuberculosis in many countries during the 1900s may have contributed to the concurrent increase in the prevalence of asthma and other atopic diseases.
To investigate these hypotheses further we have conducted an ecological analysis of the relationship between tuberculosis notification rates and the prevalence of symptoms of asthma, allergic rhinitis, and atopic eczema in countries in which standardised data are available.
Methods
The analysis was based on the data for 13–14 year olds from the International Study of Asthma and Allergies in Childhood (ISAAC).2 ,13-15 ISAAC involved 463 801 children in this age group in 155 collaborating centres in 56 countries, of which 304 796 were in the 99 centres in 42 countries which used the optional asthma video questionnaire. The analyses in this paper were, however, confined to those countries in which the tuberculosis notification rates were considered to be of sufficient validity16—namely, countries in western, northern, central and eastern Europe as well as the USA, Canada, Australia and New Zealand (a full list is given at the end of the paper). These involved 235 477 children in 85 centres in 23 countries, of which 143 551 were in 52 centres in 17 countries which used the optional video questionnaire. The first centre survey took place in 1991, but most of the data were collected during the period 1994–5.
For each country the annual tuberculosis notification rates per 100 000 during 1980–2 were obtained from the World Health Organization17 and were averaged over these three years. This time period was chosen because it corresponded to the period during which participants in the ISAAC study were infants.
The analyses involved the key questions of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema from the ISAAC written and video questionnaires.18 The asthma questions used were those on wheeze ever and wheeze in the last 12 months, and on asthma ever from the written questionnaire.2 ,13 The video asthma question used was the sequence on wheeze at rest in the last 12 months. These questions were chosen because they have been shown to have the greatest validity19 and because the video question on wheeze at rest was used in both versions of the asthma video. The questions on rhinitis used were those on symptoms of rhinitis ever, rhinitis in the last 12 months, and rhinoconjunctivitis in the last 12 months.14 The questions on atopic eczema used were those on eczema ever, and on symptoms of an itchy rash ever and in the last 12 months.15
For each of these questions the data were analysed by multiple linear regression with one data point for each centre, weighted by the inverse variance of the prevalence estimate for the centre, and adjusted for the gross national product (GNP) of the country in which the centre was based.20 The level of affluence of a country was considered to be a potential confounder since increasing industrialisation and affluence involve changes in lifestyle and environmental exposures which could be related to asthma risk, as well as to the decreased risk of tuberculosis infections.21Inclusion of GNP in the model only led to a minor increase in the standard errors for the tuberculosis coefficients, indicating that multicollinearity was not a significant problem.
Results
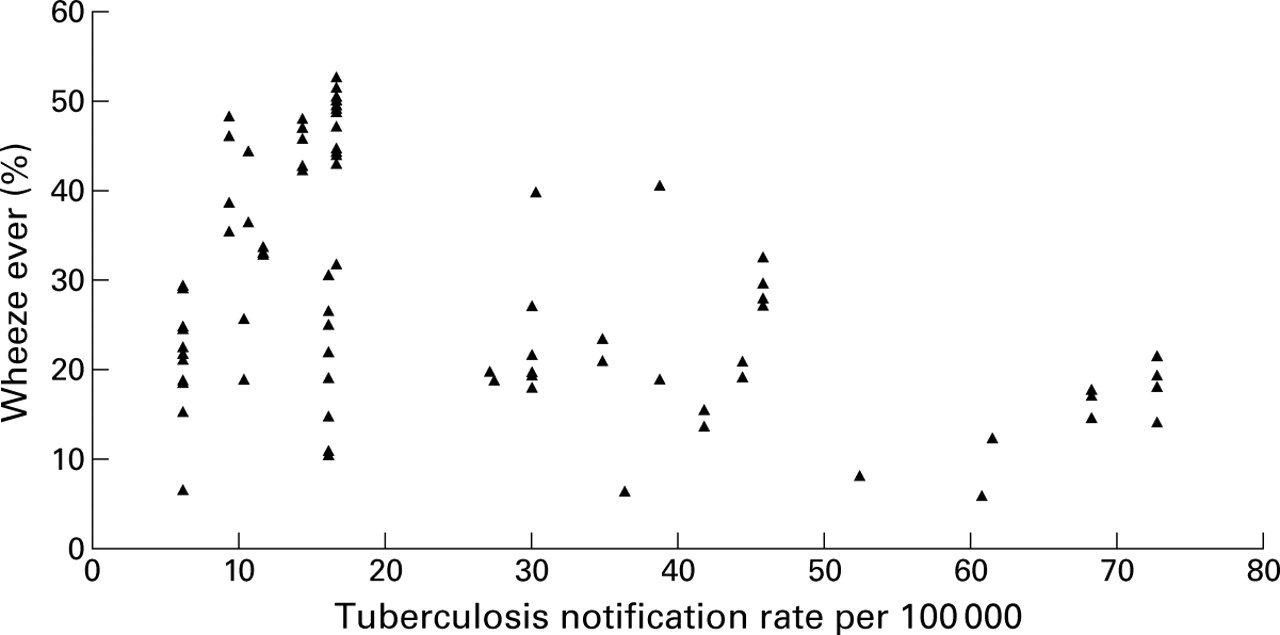
Table 1 shows the findings for the 85 centres from 23 countries considered to have valid tuberculosis notification data and comparable prevalence data for symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema. Tuberculosis rates were significantly inversely associated with the prevalence of all four asthma questions considered in the univariate analyses (table 1, fig 1). All of these inverse associations were reduced when the analysis was adjusted for GNP, but three of the four asthma questions (wheeze ever, asthma ever, and the video question) still showed significant inverse associations. These analyses showed, for example, that an increase in the tuberculosis notification rates of 25 per 100 000 was associated with an absolute decrease in the prevalence of wheeze ever of 4.7%.
Regression analysis of the prevalence of symptoms of asthma, rhinitis and eczema (by centre) against tuberculosis notification rates adjusted for gross national product (GNP) and weighted by the inverse variance of the prevalence in each centre: countries with valid tuberculosis notification data1-150
{kind=link}
Wheeze ever (written questionnaire) by tuberculosis notification rate in countries with valid tuberculosis notification data (85 centres, 23 countries).
Symptoms of allergic rhinoconjunctivitis in the past 12 months were inversely associated with tuberculosis notification rates in both the univariate and adjusted analyses (table 1). There were no other significant associations with the key questions from the rhinitis questionnaire or the eczema questionnaire when the analysis was adjusted for GNP. The rhinitis questions showed non-significant negative associations after adjustment for GNP, whereas the significant negative associations for the eczema questions became (non-significantly) positive.
Discussion
This study has identified that there is a significant inverse correlation between the prevalence of asthma and tuberculosis notification rates in countries where standardised data are available. These findings are consistent with the hypothesis that exposure toM tuberculosis in early childhood may reduce the risk of developing asthma. Before considering these findings further it is necessary to discuss the potential sources of bias.
The first consideration is the accuracy of the data on which the calculations were based. The main concern related to the accuracy of the tuberculosis notification rates published by the World Health Organization. Unfortunately, these data can only be considered to be reliable from certain regions in the world, with those emanating from Africa, Asia, Central and South America being regarded as highly inaccurate and grossly under-representing the prevalence of tuberculosis in most of the countries in these regions.16Our analysis has therefore been based on data from those 23 countries in which the WHO has recommended that it could be considered to be of acceptable accuracy. Tuberculosis notification rates are national figures which may not accurately reflect local patterns of infection. Random misclassification of exposure is, however, likely to bias results towards the null underestimation of the true effect.22
A related issue is whether a measure of tuberculous infection such as tuberculin testing would have been a more appropriate marker of exposure to M tuberculosis than the tuberculosis notification rates. Although tuberculin sensitivity would represent a direct method for assessing the exposure of a population toM tuberculosis, these data are not available in standardised form in more than a few countries23 and their interpretation is confounded by BCG vaccination which varies between countries. Furthermore, tuberculin reactivity is also a delayed type hypersensitivity reaction which is affected by the Th1/Th2 balance, thereby inversely relating to atopy.12 In contrast, tuberculosis notification rates estimate the prevalence of diseased individuals in a population, predominantly adults. In children, M tuberculosis is almost exclusively transmitted from infectious adults by inhalation of airborne droplet nuclei.24 The tuberculosis notification rates may thus be a better estimate of children's exposure toM tuberculosis than tuberculin responses.
The data used for the prevalence of asthma, allergic rhinoconjunctivitis, and atopic eczema were derived from the recently published ISAAC study which employed standardised methodology including both written and video questionnaires.2 ,18 For the written questionnaires standard guidelines for translation from English were provided in an attempt to decrease difficulties associated with the use of the questionnaires in many different languages. These guidelines included the use of translators familiar with asthma terminology, consultation with the local community, back-translation into English by an independent translator, and pilot testing of the translation. The asthma video questionnaire was designed to provide more accurate recognition of clinical asthma and to avoid problems of translation of terms such as “wheeze”. Furthermore, both written and video questionnaires have been validated using objective measures of traits closely associated with asthma such as atopic sensitisation and airway hyperresponsiveness.25
A second and perhaps more major limitation of our study is the fact that it is based on ecological analyses—that is, we have based the analyses on countries rather than individuals. The limitations of ecological analyses are well known.26 In particular, although we know that tuberculosis is negatively associated with asthma risk across the countries included in this analysis, we do not know whether this applies to individuals within these countries.
Even if the “ecological fallacy” is not itself a major problem, low tuberculosis notification rates may be a surrogate for other aspects of affluence which are associated with an increased risk of asthma. Recent findings from Sweden do, in fact, point towards a significant modification of the relation between atopy and tuberculin test reactivity by affluence of the country of origin.27 It is reassuring that, in the data presented here, the inverse association between tuberculosis and asthma prevalence was maintained when the analysis was adjusted for GNP. However, in most instances the regression coefficient was reduced by about one half after adjustment for GNP, and it might have been reduced further if “affluence” could have been controlled for more precisely.
Thus, there are some factors (particularly random inaccuracies in the tuberculosis and symptom prevalence data) that are likely to have biased our results towards the null28 whereas other factors (ecological bias, uncontrolled confounding by level of affluence) could have biased our results away from the null. The analyses presented here cannot therefore be regarded as conclusive in themselves, but should be considered together with other experimental and epidemiological evidence. In this context, the findings are consistent with the evidence from experimental8-10 ,29and population based11 studies and with the trends of the increasing prevalence of asthma and atopic diseases worldwide.
In particular, the major finding was a significant inverse correlation between the tuberculosis notification rates and the prevalence of asthma symptoms in the 23 countries from which sufficiently valid data for both measures were available. It could be calculated that an increase in cases of tuberculosis of 25 per 100 000 population was associated with an absolute reduction in the prevalence of asthma symptoms of 4.7 per 100 persons. Risk effects of similar magnitude were observed when the video questionnaire was used, suggesting that these findings are unlikely to be due to translation problems with the written questionnaire. Weaker effects were seen for wheeze in the past 12 months which may be attributable to the fact that a significant proportion of adolescents lose their symptoms during puberty.
In contrast to the findings in relation to asthma, there was no consistent significant relationship between tuberculosis rates and the prevalence of rhinitis or atopic eczema after adjustment was made for GNP, although there was a significant association with rhinoconjunctivitis. While these findings may suggest that the effects of tuberculosis relate to the development of asthma rather than atopy per se, the finding that symptoms of rhinoconjunctivitis are more closely related to skin test positivity than symptoms of rhinitis alone30 would not support this interpretation. An alternative interpretation concerning the discrepant findings for the different disorders is that infection with M tuberculosis predominantly affects the lungs, resulting in a local immune response, but may not induce systemic responses as shown in animal models.29 In this respect, the ability ofM tuberculosis to persist in the lungs throughout life, prevented from causing active or disseminated disease by the host's ongoing immune response, may be relevant.
In conclusion, this study is consistent with the recent experimental and epidemiological evidence which suggests that exposure toM tuberculosis may reduce the risk of developing asthma. Prospective clinical studies are now needed, not only to test the hypothesis that early childhood exposure to organisms such as M tuberculosis can influence the risk of developing asthma, but also to examine whether aMycobacterium-based vaccine may reduce the risk of asthma as has recently been shown in animal studies.31
Acknowledgments
The following 23 countries were included in the analysis of the questionnaire data: Albania, Austria, Belgium, Estonia, Finland, France, Georgia, Germany, Greece, Ireland, Italy, Latvia, Poland, Portugal, Romania, Russia, Spain, Sweden, United Kingdom, Canada, USA, Australia and New Zealand.
The authors thank the collaborators in the participating centres and all parents, children, teachers, and other school staff who participated in the surveys; the field workers and funding agencies who supported data collection; and national, regional, and international meetings, including the meetings of the ISAAC Steering Committee.
References
Footnotes
Funding: the ISAAC International Data Centre including the Health Research Council of New Zealand, the Asthma and Respiratory Foundation of New Zealand, Glaxo Wellcome International, the Child Health Foundation of New Zealand, the Hawke's Bay Medical Research Foundation, the Waikato Medical Research Foundation, Glaxo Wellcome New Zealand Ltd, and Astra New Zealand. The regional coordinating centres were supported by Glaxo Wellcome International Medical Affairs. The collaboration in Europe was partially funded by the EU Biomed programme.