Article Text

Abstract
BACKGROUND Diaphragm function can be assessed by electromyography of the diaphragm during electrical phrenic nerve stimulation (ES). Whether phrenic nerve conduction time (PNCT) and diaphragm electrical activity can be reliably measured from chest wall electrodes with ES is uncertain.
METHODS The diaphragm compound muscle action potential (CMAP) was recorded using an oesophageal electrode and lower chest wall electrodes during ES in six normal subjects. Two patients with bilateral diaphragm paralysis were also studied. Stimulations were deliberately given in a manner designed to avoid or incur co-activation of the brachial plexus.
RESULTS For the oesophageal electrode the PNCT was similar with both stimulation techniques with mean (SE) values of 7.1 (0.2) and 6.8 (0.2) ms, respectively (pooled left and right values). However, for surface electrodes the PNCT was substantially shorter when the brachial plexus was activated (4.4 (0.1) ms) than when it was not (7.4 (0.2) ms) (mean difference 3.0 ms, 95% CI 2.7 to 3.4, p<0.0001). A small short latency CMAP was recorded from the lower chest wall electrodes during stimulation of the brachial plexus alone.
CONCLUSIONS The results of this study show that lower chest wall electrodes only accurately measure PNCT when care is taken to avoid stimulating the brachial plexus. A false positive CMAP response to phrenic stimulation could be caused by inadvertent stimulation of the brachial plexus. This finding may further explain why the diaphragm CMAP recorded from chest wall electrodes can be unreliable with cervical magnetic stimulation during which brachial plexus activation occurs.
- phrenic nerve conduction time
- diaphragm compound muscle action potential (CMAP)
- diaphragm paralysis
Statistics from Altmetric.com
Accurate measurement of the diaphragm compound muscle action potential (CMAP) and phrenic nerve conduction time (PNCT) can provide important information regarding diaphragm and phrenic nerve function. Lower chest wall electrodes have usually been used to record the diaphragm CMAP during phrenic nerve stimulation because they are convenient and acceptable for subjects. Although the diaphragm CMAP recorded from lower chest wall electrodes elicited by transcutaneous electrical stimulation (ES) is often assumed to be free of contamination,1 ,2 the short PNCT (<5 ms) measured in some normal subjects2 ,3 suggests that chest wall electrodes do not always accurately measure PNCT. Some investigators3 ,4 have recommended that activation of the brachial plexus should be avoided during stimulation of the phrenic nerve but some involvement may be difficult to detect. No study has systematically investigated the effect of brachial plexus activation on the diaphragm CMAP recorded from lower chest wall electrodes.
Cervical magnetic stimulation (CMS) combined with chest wall electrodes is increasingly used for the assessment of diaphragm function.2 ,5-10 The value of surface EMG recordings rests on the assumption that lower chest wall electrodes record the EMG from the diaphragm and that these recordings are not affected by the co-activation of the muscles innervated by the brachial plexus which is inevitably activated during CMS.2 ,5 ,7 ,9 ,11 We have recently shown that the diaphragm CMAP elicited by magnetic stimulation of the phrenic nerves recorded from lower chest wall electrodes is unreliable, probably due to contamination by electrical activity from extradiaphragmatic muscles.11 If the diaphragm CMAP recorded from lower chest wall electrodes is influenced by the co-activation of the brachial plexus, then the diaphragm CMAP amplitude and latency obtained with CMS would need to be reinterpreted due to signal contamination.
To investigate whether the diaphragm CMAP recorded from chest wall electrodes can be affected by co-activation of the brachial plexus we recorded the diaphragm CMAP from lower chest wall electrodes and an oesophageal electrode simultaneously during ES, with and without co-activating the brachial plexus. We also investigated whether a CMAP can be recorded from lower chest wall electrodes during stimulation of the brachial plexus alone.
Methods
SUBJECTS
Six healthy volunteers (three men) aged 25–37 years (mean age 30) participated in the study. The subjects were members of the laboratory staff and all were free of neurological and respiratory disease. We also studied two patients with bilateral diaphragm paralysis confirmed by measurements of sniff transdiaphragmatic pressure (Pdi) and twitch Pdi. The study was approved by the ethics committee of King’s College Hospital and normal subjects and patients gave their informed consent.
STIMULATION OF THE PHRENIC NERVE
Stimulation focused on the phrenic nerve
The phrenic nerves were stimulated at the posterior border of the sternomastoid muscle at the level of the cricoid cartilage with a bipolar surface stimulating electrode (Medelec Ltd, Surrey, UK). The cathode was placed at the lower level. Square wave impulses of 0.1 ms duration were delivered. Stimulation began at low voltage. Once an action potential was observed the stimulus voltage was progressively increased until there was no further increase in amplitude of the CMAP. To ensure that supramaximal stimulation of the phrenic nerves was achieved, the intensity of stimulation was then further increased by 20% for the remainder of the study. The stimulation intensity for the patients with diaphragm paralysis was fixed at 160 V since this intensity is maximal for most subjects.1 The subjects sat upright in a chair throughout the studies. Stimulations were delivered at end tidal expiration by carefully observing chest movement and asking subjects to hold their breath and relax at end expiration. As much care as possible was taken to avoid co-activating the brachial plexus during ES by observing for muscle contractions and arm movement.
Stimulation of the phrenic nerve and the brachial plexus
The purpose of this procedure was to stimulate the phrenic nerve and the roots of the brachial plexus simultaneously during ES. The stimulating electrode was positioned in the supraclavicular fossa since the brachial plexus is easily activated at this site.12The optimal position of the stimulating electrode was based on the amplitude of the diaphragm CMAP recorded from the oesophageal electrode combined with strong arm movement and paraesthesia. The intensity of ES was the same as or greater than that used to achieve maximal stimulation in the study focused on the phrenic nerve. Seven stimulations were performed.
RECORDING OF THE CMAP
Lower chest wall electrodes
Two skin silver/silver chloride electrodes (Arbo Medical, Connecticut, USA) were placed over abraded skin over the sixth to eighth intercostal spaces in the anterior axillary line on the left and right side. The distance between the electrodes was 3–5 cm.
Oesophageal electrode in normal subjects
The oesophageal electrode catheter consisted of three coils 1 cm in width separated by a distance of 3 cm. The middle electrode acted as a common one with the upper and lower electrodes to form two pairs of electrodes. The oesophageal electrode was introduced pernasally and swallowed into the oesophagus. The middle electrode was positioned at the level of the oesophageal hiatus by observing the polarity and amplitude of the CMAP recorded from the two pairs of electrodes during left electrical stimulation.11 ,13 ,14 This was characterised by the negative polarity and similar amplitude of the CMAP recorded from two pairs of electrodes.11 ,13 When the optimal position had been determined the electrode catheter was taped at the nose. We used the lower electrode pair to record the diaphragm CMAP for the remainder of the study. The purpose of the upper pair was therefore to control the positioning of the electrode. The diaphragm CMAP was recorded simultaneously from the lower chest wall and oesophageal electrodes.
Oesophageal electrode for confirming diaphragm paralysis in patients
We used a catheter with four pairs of electrodes rather than two to record the diaphragm CMAP from the two patients to further confirm diaphragm paralysis. This oesophageal catheter consisted of five electrodes which were also 1 cm in width separated by a distance of 3 cm. The recording electrodes had a span of 17 cm which was wide enough to cover the oesophageal hiatus when the proximal electrode was 40 cm from the nose. We recorded the diaphragm CMAP simultaneously from the four electrode pairs during ES. The sampling rate was 2 kHz. This electrode was designed to overcome the difficulty in positioning the electrode adjacent to the diaphragm without reference to the CMAP.
EMG signals were amplified and then passed to a 12 bit analogue-to-digital converter (NB-MIO-16, National Instruments, Austin, Texas, USA) and stored and displayed on a Macintosh Centris Computer running Labview™ 2.2 software (National Instruments, Austin, Texas, USA). The signals were available in real time to the investigators. Unless stated otherwise, the sampling rate was 10 kHz.
ADDITIONAL STUDY
The purpose of this study was to observe whether the lower chest wall electrodes recorded an EMG response when only the brachial plexus was activated. The CMAP was recorded simultaneously from an oesophageal electrode and three pairs of surface electrodes: upper chest wall electrodes (placed over the pectoralis major muscle in the anterior axillary line in the fourth and fifth intercostal spaces), conventional lower chest wall electrodes (placed over the sixth to eighth intercostal spaces in the anterior axillary line), and posterior chest wall electrodes (placed over the latissimus dorsi in the posterior axillary line at the same level as the lower chest wall electrodes). The stimulating electrode was in the supraclavicular fossa, positioned so as to stimulate the brachial plexus but not the phrenic nerve. The stimulus intensity was 160 V and induced strong arm movement without hiccup. Selectivity of stimulation was confirmed by EMG recordings from the chest wall and oesophageal electrodes which were characterised by no or little EMG activity from the oesophageal electrode accompanied by a large EMG from the upper and posterior chest wall electrodes. The optimal position was usually slightly beyond the posterior border of the sternocleidomastoid muscle in the supraclavicular fossa. Stimulation focused on the phrenic nerve was also performed to compare with that focused on the brachial plexus. Bilateral studies were performed on three subjects.
ANALYSIS OF DATA
We only analysed CMAP responses with constant shape and similar amplitude, and with a stable baseline before and after stimulation, to eliminate the influence of the ECG on the CMAP. Using these criteria at least four stimulations were available for analysis for every subject for each part of the study. The PNCT was defined as the time from the stimulation artefact to the onset of the CMAP. The amplitude of the CMAP was measured from peak to peak. Results were expressed as the mean (SE) and paired t tests were used to test for differences.
Results
Stimulation focused on the phrenic nerve
Good quality diaphragm CMAPs were usually obtained from both oesophageal and chest wall surface recordings when the stimulating cathode was at the level of the cricoid cartilage and care was taken to avoid stimulating the brachial plexus. For chest wall recordings the amplitude of the CMAP was 0.61 (0.13) mV and 0.53 (0.09) mV for the left and right sides, respectively. The amplitude of the CMAP recorded from oesophageal electrodes was 2.2 times larger than that simultaneously recorded from chest wall electrodes (mean difference 0.70 mV, 95% CI 0.43 to 0.98, p<0.0001). The PNCT measured from chest wall electrodes was 7.2 (0.2) ms and 7.6 (0.4) ms for the left and right sides, respectively (table 1).
Phrenic nerve conduction time (PNCT) and amplitude of the compound muscle action potential (CMAP) recorded from oesophageal and lower chest wall electrodes during electrical stimulation (ES) focusing on the phrenic nerve and when co-activating the brachial plexus
Stimulation of both phrenic nerve and brachial plexus
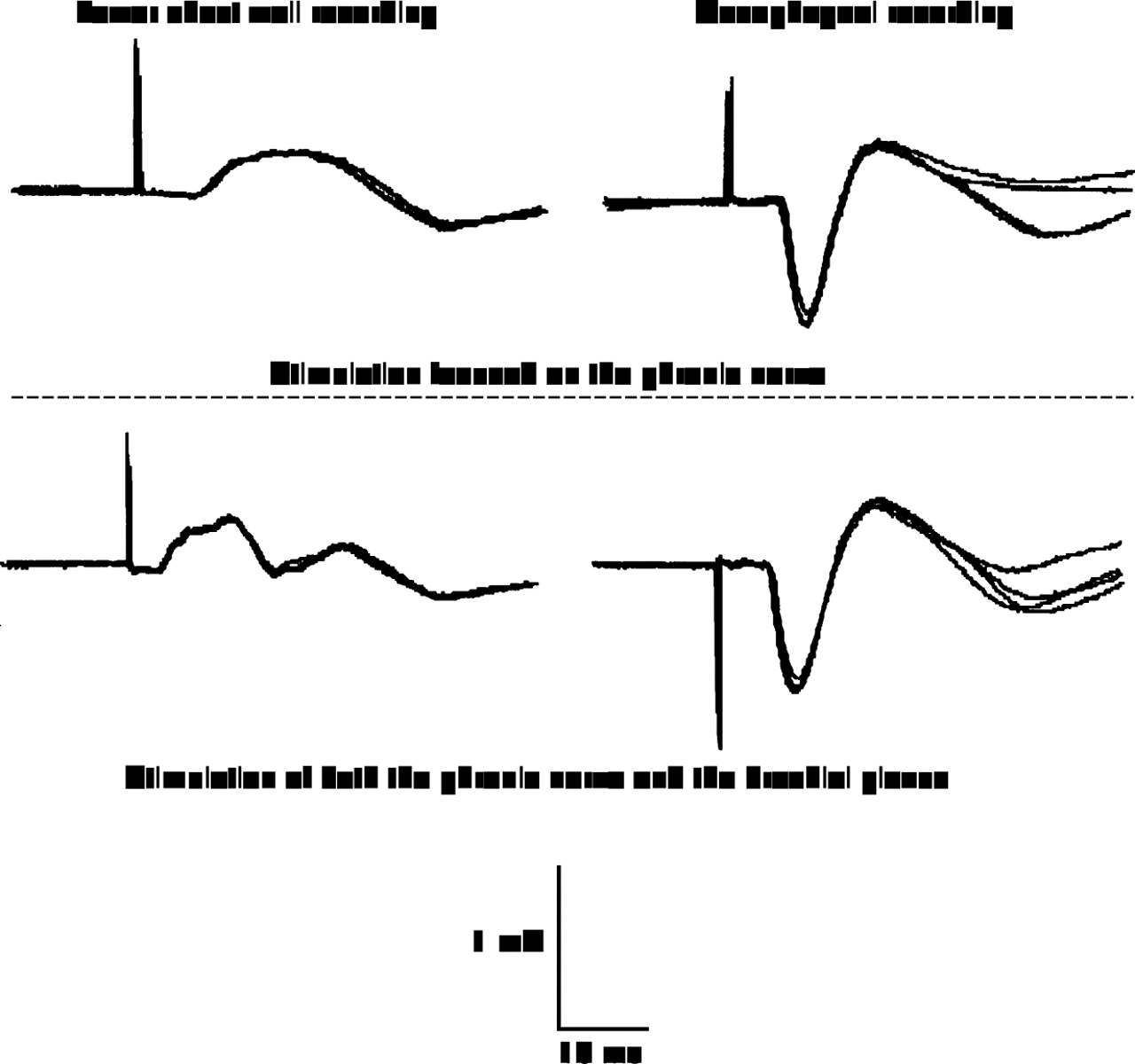
When ES was performed in such a way as to stimulate both the phrenic nerve and the brachial plexus, an obvious arm movement was observed and some subjects considered the procedure to be more uncomfortable than focused phrenic nerve stimulation. For chest wall surface recordings the shape of the diaphragm CMAP was different from that elicited by stimulation focused on the phrenic nerve. The signals were sometimes irregular (figs 1 and 2). The latency of the CMAP was substantially shorter when compared with that measured from focused phrenic nerve stimulation and was 4.3 (0.2) ms for the left side and 4.5 (0.2) ms for the right side (table 1, figs 1 and 2). However, the latency of the CMAP recorded from the oesophageal electrode was similar for both stimulation techniques and was 6.9 (0.2) ms for the left side and 6.7 (0.3) ms for the right. For oesophageal recordings the CMAP amplitude obtained from both stimulation techniques was similar. For chest wall surface recordings, although the amplitude of the CMAP was similar for the group, there were differences in amplitude for the two techniques for some individuals (table 1); the CMAP amplitude from surface electrodes was substantially higher when the brachial plexus was activated in some subjects whereas the amplitude recorded from the oesophageal electrode was similar (fig 1).
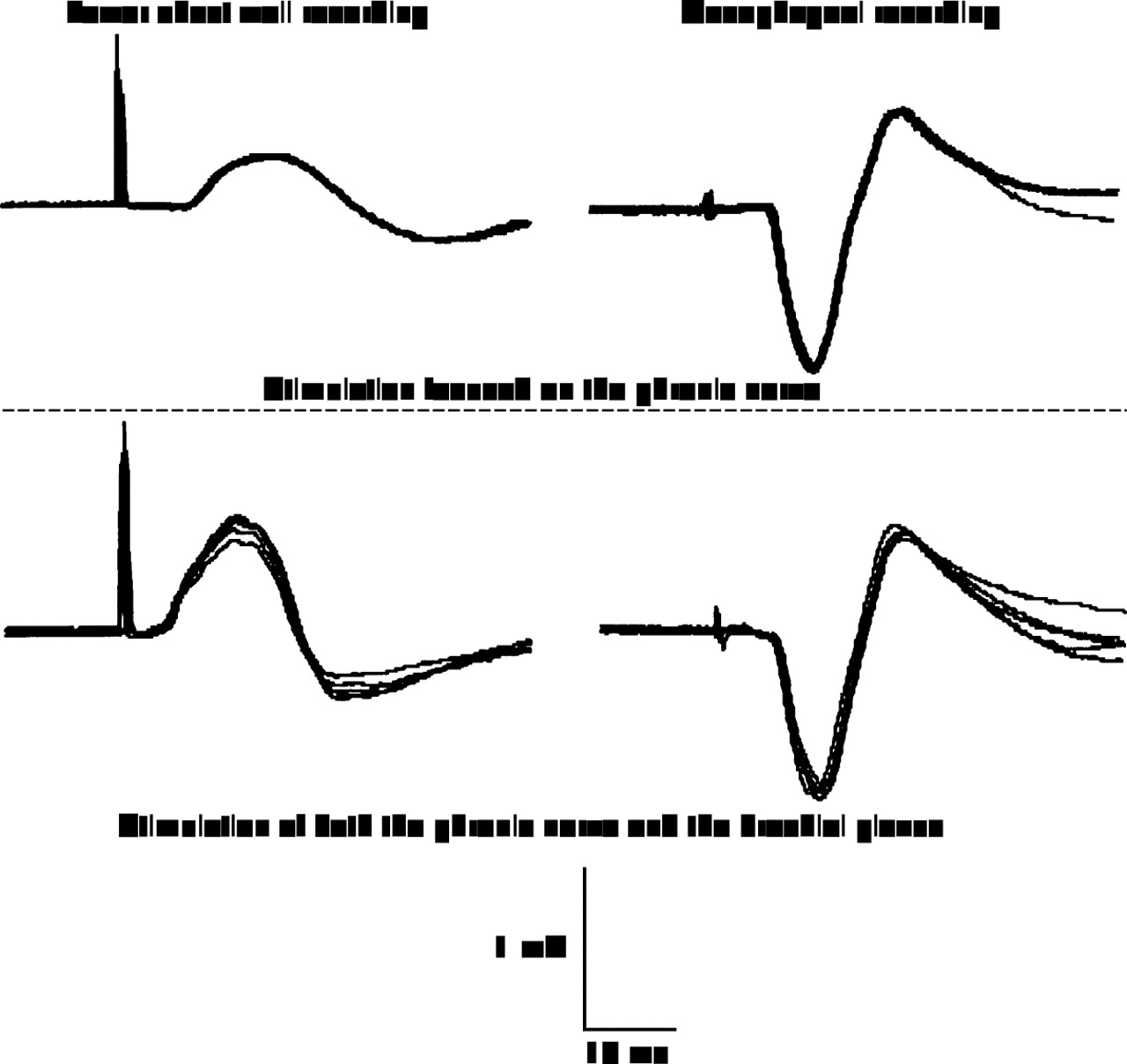
Diaphragm compound muscle action potential (CMAP) recorded simultaneously from lower chest wall and oesophageal electrodes during stimulation of the phrenic nerve only (upper traces) and both the brachial plexus and the phrenic nerve (lower traces). For lower chest wall recordings the shape of the CMAP was different and the amplitude of the CMAP was nearly twice as great and the latency of the CMAP was reduced by 3.1 ms when the brachial plexus was activated. For oesophageal recordings the waveforms of the CMAP were similar. Five stimulations superimposed. Data from one subject.

Diaphragm compound muscle action potential (CMAP) recorded simultaneously from lower chest wall and oesophageal electrodes during stimulation of the phrenic nerve only (upper traces) and both the brachial plexus and the phrenic nerve (lower traces). For lower chest wall recordings the latency of the CMAP is shorter when stimulation co-activates the brachial plexus. The amplitude of the CMAP is also reduced. For oesophageal recordings the waveforms of the CMAP were similar. Four stimulations superimposed. Data from one subject.
In the two patients with diaphragm paralysis we could not record a CMAP from the multipair oesophageal electrode during ES. No CMAP was recorded from the lower chest wall when the stimulating electrode was at the level of the cricoid cartilage. These results confirmed diaphragm paralysis. A small short latency CMAP was recorded from the lower chest wall electrodes when stimulating three of the four brachial plexuses (fig 3).

Compound muscle action potential (CMAP) recorded from oesophageal and lower chest wall electrodes during electrical stimulation of the phrenic nerve in a patient with bilateral diaphragm paralysis. When stimulation was performed in the supraclavicular fossa (left) a small short latency CMAP was recorded. No CMAP was recorded from the oesophageal electrode (right), confirming diaphragm paralysis. Data from one patient.
ADDITIONAL STUDY
When stimulation was focused on the phrenic nerve good quality diaphragm CMAPs could be obtained from both the oesophageal and lower chest wall electrodes. A small amplitude CMAP (0.18 (0.03) mV) was usually recorded from the upper chest wall electrodes. When stimulation was focused only on the brachial plexus a small CMAP (0.13 (0.02) mV) was recorded from the oesophageal electrode (12.5% of maximal diaphragm CMAP amplitude) whereas 70% of maximal diaphragm CMAP amplitude was recorded from lower chest wall electrodes. The CMAP amplitude recorded from upper and posterior chest wall electrodes substantially increased when stimulation was focused on the brachial plexus rather than the phrenic nerve (0.99 (0.14) mV vs 0.18 (0.03) mV for upper chest wall recordings and 1.00 (0.08) mV vs 0.66 (0.06) mV for posterior chest wall recordings), associated with a shortened latency of the CMAP (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diaphragm compound muscle action potential (CMAP) recorded simultaneously from upper chest wall electrodes, posterior chest wall electrodes, lower chest wall electrodes, and an oesophageal electrode during phrenic nerve stimulation and brachial plexus stimulation. Left side: stimulation of the phrenic nerve. Good quality diaphragm CMAPs were recorded from both oesophageal and lower chest wall electrodes. The onset of the CMAP was obvious and the phrenic nerve conduction time was easy to measure. The diaphragm CMAP recorded from posterior electrodes had a high amplitude but the latency of the CMAP was short. A small CMAP was also recorded from the upper chest wall electrodes. Right side: stimulation of the brachial plexus. In contrast to phrenic nerve stimulation no clear CMAP was recorded from the oesophageal electrode, confirming that the phrenic nerve was not stimulated. However, large amplitude CMAPs were recorded from the chest wall electrodes with short latencies. Data from one subject.
Discussion
This study shows that the PNCT measured from chest wall electrodes using ES in such a way that the brachial plexus is stimulated is substantially shorter than the PNCT obtained from ES of the phrenic nerve alone. Such signals also vary in amplitude, whereas the amplitude of signals recorded from an oesophageal electrode is similar for the two stimulation techniques. These findings have practical implications for investigators using both ES and CMS.
When we moved the stimulating electrode from the level of the cricoid cartilage where it was focusing on the phrenic nerve to a slightly lower position to co-activate the brachial plexus, the PNCT measured from lower chest wall electrodes shortened by approximately 3.0 ms. This cannot be explained by the slightly lower position of the stimulating electrode. The length of the phrenic nerve from the cricoid to the diaphragm surface (branching point) is about 350 mm.15 For a mean PNCT of 7 ms the slight change of stimulating electrode position (<2 cm) could account for a reduction of up to 0.4 ms of PNCT. The short PNCT cannot be explained by electrode movement since the CMAP precedes the mechanical response by about 6 ms16 and so short a latency (<5.2 ms) cannot be influenced by the mechanical response to stimulation in the neck. The short latency measured from surface electrodes is most probably due to the diaphragm CMAP being contaminated by chest muscles innervated by the brachial plexus, such muscles having a short latency.
We placed the lower chest wall electrodes over the sixth to eighth intercostal spaces in the anterior axillary line to record the diaphragm CMAP. This is the preferred location of many investigators2 ,5-7 ,10 ,17 because this site usually results in a high CMAP amplitude3 ,16 and less contamination18 because it is distant from the muscles innervated by the brachial plexus. Although the chest wall muscles innervated by the brachial plexus do not lie directly below the electrodes, the CMAP originating from these muscles can be transmitted to the electrodes by volume conduction. It has been shown that the diaphragm EMG can be recorded from electrodes over the abdomen far from the diaphragm,13 and the diaphragm CMAP elicited by unilateral ES of the phrenic nerve can be recorded from contralateral chest wall electrodes.13 ,19 These are examples of volume conduction. The EMG of the adjacent chest wall muscles may therefore be transmitted to the surface electrodes by this mechanism. Indeed, MacLean and Mattioni20 observed that activation of the latissimus dorsi obscured the lower chest wall recordings of the diaphragm CMAP, and Bolton21 showed that when the brachial plexus was stimulated a CMAP whose shape and latency differed from the diaphragm CMAP could be recorded. In the present study, when we focused the stimulation on the brachial plexus without activating the diaphragm a small short latency CMAP could be recorded in normal subjects (fig4). This small CMAP is likely to originate from chest wall muscles rather than the diaphragm since no CMAP could be detected from the oesophageal electrode. We could also record a small short latency CMAP from surface electrodes in patients with diaphragm paralysis when stimulating the brachial plexus in the supraclavicular fossa (fig 3). Furthermore, when we stimulated both the brachial plexus and the phrenic nerve simultaneously the latency and shape of the CMAP recorded from lower chest wall electrodes differed from that when only the phrenic nerve was stimulated (figs 1 and 2). We could not record a CMAP on the side of stimulation when stimulation was in the supraclavicular fossa in one patient with diaphragm paralysis. However, this patient had severe amyotrophic lateral sclerosis and upper limb weakness and the chest wall muscles may have been severely affected by the disease.
Signals from the brachial plexus may explain the observed variability in CMAP amplitude and shape since many muscles innervated by the brachial plexus could transmit signals to the surface electrodes. Different chest muscles will have different CMAP shapes (fig 4) and the muscles co-activated during ES could differ between individuals; this source of variability could explain why there was not a consistent CMAP response when the brachial plexus was stimulated.
Reliably recording the diaphragm CMAP depends on adequate and specific stimulation of the phrenic nerve and the position of the recording electrodes.18 It has been suggested that, to avoid stimulating the brachial plexus, the stimulating position can be slightly changed if arm movement occurs or a very short latency CMAP is recorded.3 ,4 ,16 However, since the brachial plexus is very close to the phrenic nerve it may be difficult to avoid activation of the brachial plexus in some cases. In the present study we took care to choose two distinct stimulation sites by reference to both the oesophageal diaphragm CMAP and arm movement. It is possible that some brachial plexus activation could occur without obvious arm movement. Attali et al 22 reported that they could record a small CMAP with ES from lower chest wall electrodes in some patients with diaphragm paralysis. In the present study we could record a short latency CMAP by stimulating the brachial plexus close to the phrenic nerve in normal subjects (fig 4) and patients with total diaphragm paralysis (fig 3 ). Thus, conventional ES may, on occasion, cause a false positive CMAP response as a result of inadvertent stimulation of the brachial plexus. Larocheet al 23 reported that they could record a CMAP from chest wall electrodes without a twitch Pdi response in a patient with suspected diaphragm paralysis using ES on the neck. Our results may explain in part the discrepancy between electrical activity and mechanical response in patient with diaphragm paralysis. Similarly, in obese subjects in whom ES can be difficult,1 a CMAP may be seen despite failure to stimulate the phrenic nerve.
Lower chest wall electrodes have been frequently used with ES to assess diaphragm electrical activity and PNCT. It is believed that the diaphragm CMAP elicited by ES recorded from chest wall electrodes originates from the diaphragm and that the PNCT can be reliably measured from lower chest wall electrodes. Our data suggest that this may not always be so and it is therefore important to review the data supporting this assumption. The PNCT measured from normal subjects first reported by Newsom-Davis16 was 7.7 ms with a range of 6.1–9.2 ms. Similar results were reported by Markandet al 18 with a range of 6.0–10.0 ms. These normal values of PNCT have been confirmed by other studies.4 ,13 ,15 ,19 ,24 However, the PNCT reported in some studies is shorter. For example, the lowest values for normal subjects were 4.78 ms in the study by Similowskiet al 2 and 3.6 ms in the study by Swenson et al.3 Even for patients with phrenic nerve dysfunction who might be expected to have a prolongation of the PNCT, values as low as 4.5 ms have been reported.1 We suspect that these CMAP results may not have arisen wholly from the diaphragm and they suggest that, even among experienced investigators, PNCT can be difficult to measure from surface electrodes during transcutaneous ES.
Cervical magnetic stimulation has frequently been used to assess diaphragm function2 ,5-10 ,22 ,25 since it was developed in 1989.9 However, conflicting results have been reported for both PNCT and CMAP amplitude measured from chest wall surface electrodes. Initial studies suggested that the diaphragm CMAP could be reliably measured from chest wall electrodes with CMS9 ,10 ,25 and the PNCT measured with CMS was the same as that measured with ES.8 ,9 ,25 In contrast, further studies showed differences between the amplitude of the CMAP elicited by CMS and ES.5 The PNCT measured with CMS is much shorter than with ES and was 5.36 ms in the study by Similowskiet al.2 Our previous study demonstrated differences between the chest wall diaphragm CMAP elicited by CMS and that with ES and postulated that the differences were due to the diaphragm CMAP being contaminated by chest wall muscle activity.11 It is recognised that the brachial plexus is invariably activated during CMS.2 ,5 ,9 Since the CMAP from chest muscles innervated by the brachial plexus can be transmitted to lower chest wall electrodes (see additional study in Results section), the “diaphragm CMAP” elicited by CMS recorded from chest wall electrodes could be a summation of the CMAP from the diaphragm and the muscles innervated by the brachial plexus, such as pectoralis major, serratus anterior, and latissimus dorsi. Since these muscles usually have a short latency (fig 4)18 the PNCT can appear to be short when the diaphragm CMAP is contaminated. The present study further explains why the diaphragm CMAP elicited by CMS recorded from chest wall electrodes can be unreliable and argues against the view that PNCT can be accurately measured with CMS.2
In conclusion, chest wall electrodes only accurately measure PNCT when great care is taken to avoid stimulating the brachial plexus. Co-activation of the brachial plexus results in shorter latency signals of variable amplitude. The site of stimulation of the phrenic nerve should not be lower than the level of the cricoid cartilage to avoid co-activating the brachial plexus. The present study, and a previous one from our laboratory,11 highlight the fact that care must be taken in interpreting the diaphragm CMAP recorded from chest wall electrodes with CMS. When using ES for diagnostic purposes investigators should be aware that false positive CMAP responses resulting from inadvertent stimulation of the brachial plexus can occur. We also suggest that a short PNCT (<5.2 ms) measured from surface electrodes should be confirmed by oesophageal EMG recordings.