Article Text

Abstract
Background: Hormone replacement therapy (HRT) and obesity both appear to increase the risk of asthma. A study was undertaken to investigate the association of HRT with asthma and hay fever in a population of perimenopausal women, focusing on a possible interaction with body mass index (BMI).
Methods: A postal questionnaire was sent to population based samples in Denmark, Estonia, Iceland, Norway, and Sweden in 1999–2001, and 8588 women aged 25–54 years responded (77%). Pregnant women, women using oral contraceptives, and women <46 years were excluded. Analyses included 2206 women aged 46–54 years of which 884 were menopausal and 540 used HRT. Stratified analyses by BMI in tertiles were performed.
Results: HRT was associated with an increased risk for asthma (OR 1.57 (95% CI 1.07 to 2.30)), wheeze (OR 1.60 (95% CI 1.22 to 2.10)), and hay fever (OR 1.48 (95% CI 1.15 to 1.90)). The associations with asthma and wheeze were significantly stronger among women with BMI in the lower tertile (asthma OR 2.41 (95% CI 1.21 to 4.77); wheeze OR 2.04 (95% CI 1.23 to 3.36)) than in heavier women (asthma: pinteraction = 0.030; wheeze: pinteraction = 0.042). Increasing BMI was associated with more asthma (OR 1.08 (95% CI 1.05 to 1.12) per kg/m2). This effect was only found in women not taking HRT (OR 1.10 (95% CI 1.05 to 1.14) per kg/m2); no such association was detected in HRT users (OR 1.00 (95% CI 0.92 to 1.08) per kg/m2) (pinteraction = 0.046). Menopause was not significantly associated with asthma, wheeze, or hay fever.
Conclusions: In perimenopausal women there is an interaction between HRT and BMI in the effects on asthma. Lean women who were HRT users had as high a risk for asthma as overweight women not taking HRT. It is suggested that HRT and overweight increase the risk of asthma through partly common pathways.
- BMI, body mass index
- ECRHS, European Community Respiratory Health Survey
- HRT, hormone replacement therapy
- IR, insulin resistance
- RHINE, Respiratory Health in Northern Europe
- asthma
- menopause
- hormone replacement therapy
- body mass index
Statistics from Altmetric.com
- BMI, body mass index
- ECRHS, European Community Respiratory Health Survey
- HRT, hormone replacement therapy
- IR, insulin resistance
- RHINE, Respiratory Health in Northern Europe
Hormonal replacement therapy (HRT) as a remedy for menopausal symptoms has long seemed to be biologically plausible, although there has been no firm assessment of its side effects. As a result of the Women’s Health Initiative1 and other trials,2 in the last few years there has been an increasing awareness of the risks of HRT, mainly on cardiovascular diseases, stroke, venous thromboembolism, and breast cancer. Less attention has been paid to the effects of HRT on the airways, even though there is mounting—but somewhat contradictory—evidence of an association between HRT and obstructive airways disease.
Data from the Nurses Health Study3,4 and the Copenhagen City Heart Study5 show that women taking HRT are more likely to have asthma. In an elderly US Medicare population,6 HRT users had higher lung function. Small intervention and case-control studies in selected healthy women generally show an improvement in asthma or lung function related to HRT intake.7,8 The apparently contradictory findings may be caused by unrecognised sources of error in some studies.9 Another possibility is that the effects of HRT differ between subgroups of women of different ages,9 metabolic conditions,10–14 or menopausal status.15
The association of asthma with BMI is well known although not fully understood.16–18 Sex hormones and body fat mass are closely interrelated; the levels of oestrogens are related to body fat mass9,12 and the subject’s metabolic status.19 Exogenous estrogens and BMI are known to interact in their effects on breast cancer; the increase in breast cancer risk related to HRT is stronger in lean women.20
Initiation of menopause may possibly also play a role in the development of asthma; asthma may sometimes start or worsen around the age of menopause,15 but has also been reported to be less common among postmenopausal women.3
We wanted to investigate the possible associations of HRT and menopause with symptoms of asthma and allergy among perimenopausal women in general population samples from Northern European countries with different prescription practices,21 particularly the possible heterogeneity in the effects of HRT according to BMI.
METHODS
Study design and subjects
The study was a cross sectional analysis of the Respiratory Health in Northern Europe (RHINE, www.rhine.nu).16,22 RHINE is a follow up study of subjects from seven Northern European centres who participated in the European Community Respiratory Health Survey (ECRHS) I stage 1 (www.ecrhs.org), a study that took place in 1990–4.23 In stage 1 of the ECRHS men and women aged 20–44 years were randomly selected from population registers within specific boundaries of each participating centre. A postal questionnaire was sent to 3000–4300 subjects in each centre. The population included in the RHINE study consisted of responders from Reykjavik in Iceland, Bergen in Norway, Umeå, Uppsala and Gothenburg in Sweden, Aarhus in Denmark, and Tartu in Estonia (n = 21 802, response rate 83.7%). The eligible subjects (excluding 264 deaths) were sent a postal questionnaire in 1999–2001. Subjects not responding to the first mailing were sent two reminders. In total, 16 191 subjects answered the questionnaire including 8588 women (response rate 77%) born between 1945 and 1973.
Analyses were restricted to women aged 46–54 years since the mean age of onset of the perimenopausal transition is 45–46 years.24 Pregnant women (n = 6) and women using oral contraceptives (n = 72) were excluded, leaving 2206 women for analyses.
There were 121 women younger than 46 years who reported menopause, and 102 of these were taking HRT. The age group 26–45 was not included in further analyses because pathological conditions underlying early menopause might introduce unknown confounders, and because the 19 younger menopausal women not taking HRT would constitute a small and possibly biased reference group.
Questionnaire
The first part of the questionnaire contained 12 questions identical to those asked in the ECRHS I stage 1. These items covered respiratory symptoms, asthma medication, and hay fever. Asthma was defined as currently using asthma medication and/or having had asthma attacks during the last 12 months, wheeze as having had wheeze during the last 12 months, night symptoms as waking with tightness in chest or waking with shortness of breath, and hay fever as currently having hay fever or nasal allergies. Three or more asthma symptoms were defined based on the following eight symptoms: wheeze, wheeze with shortness of breath, wheeze without cold, waking with tightness in chest, waking with shortness of breath, waking with cough, asthma attacks, and current asthma medication.25
The second part of the questionnaire included 52 items covering various aspects including factors related to hormonal status in women. Menopause was defined as answering “yes” to the question “Have you reached the menopause (6 or more months since your last menstruation)?”. HRT was defined as answering “yes” to the question “Are you using hormones/hormone replacement therapy?”. In some centres HRT was only registered in women answering “yes” to having reached the menopause. The women were also asked about pregnancy, use of oral contraceptives, age of menopause, and date of the last menstrual bleeding.
BMI was based on self-reported weight and height and calculated as kg/m2. Smoking history was assessed by two questions: “Are you a smoker?” and “Are you an ex-smoker?” Based on these, three groups were defined (never smokers, ex-smokers, and current smokers). Type of dwelling (detached, semi-detached, apartment, other) was used as a proxy for social class, “detached” corresponding to upper social class, etc. A socioeconomic index based on current occupation was available in four centres (Bergen, Gothenburg, Uppsala, and Tartu). In these centres the type of dwelling was strongly correlated with socioeconomic index (p<0.001), and analyses with adjustment for this variable gave similar results as when adjusting for type of dwelling.
Statistical analysis
Logistic regression models were used to assess the effects of menopause and of HRT on asthma and hay fever. The number at risk fluctuated slightly from outcome to outcome because of a varying number of missing data for each variable. Adjustments were made for age (5 year categories), BMI (kg/m2), smoking habits (never, ex, and current smoking), study centre, and social class (type of dwelling). Analyses of HRT were stratified according to BMI categorised in tertiles. Based on the results from the stratified analyses, the two upper tertiles were grouped together post hoc and the differences in the effects of HRT on asthma between lean and heavier women were analysed by including interaction terms of BMI and HRT in the logistic regression models. Similarly, logistic regression models were used to assess the effects of BMI (as a continuous variable) on asthma and hay fever; analyses were stratified by HRT use and an interaction term between BMI and HRT was included to assess the statistical significance of differences in BMI effects between subjects using or not using HRT. Potential heterogeneity between centres was studied by meta-analyses according to derSimonian and Laird. The analyses were carried out using the statistical software program Stata 7.0 (Stata Corporation, College Station, Texas, USA).
RESULTS
Of 2206 women aged 46–54 years, 540 (24%) were using HRT at the time of the study. There was some variation between centres, with HRT being more widely used in Reykjavik and Bergen and less used in Tartu and Aarhus compared with the Swedish centres (table 1). In total, 844 women reported that they were menopausal (table 1). Women taking HRT were leaner, were more often smokers, and more often lived in a semi-detached house than women not taking HRT.
Characteristics of women aged 46–54 years participating in the RHINE study
Asthma, wheeze, or hay fever did not differ significantly between premenopausal and postmenopausal women, while there was a borderline significant association between night symptoms and menopause (table 2).
Asthma and hay fever according to menopause in 1527 women aged 46–54 years (women using HRT were excluded)
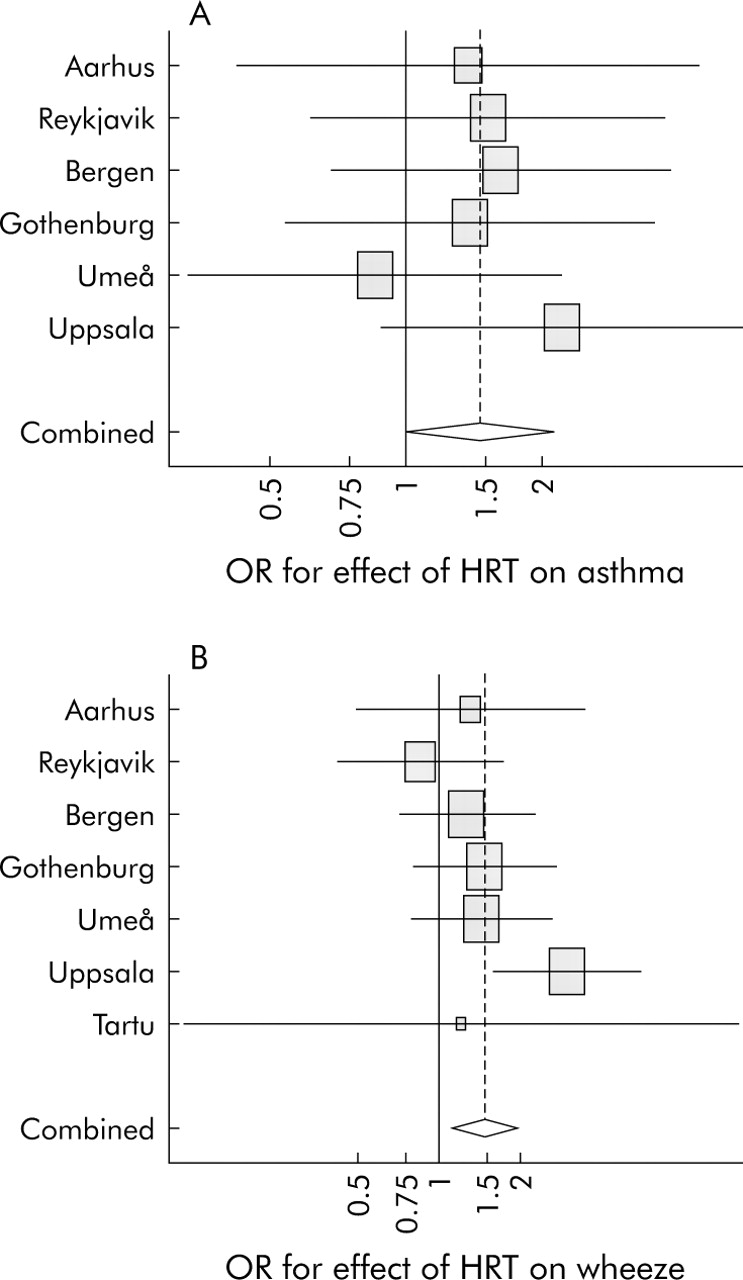
Asthma, asthma symptoms and hay fever, but not night symptoms, were significantly more common among women using HRT (table 3). There was no significant heterogeneity between centres in the association of HRT with asthma or wheeze (pheterogeneity = 0.84 and 0.35 for asthma and wheeze, respectively; fig 1).
Asthma and hay fever according to HRT use in 2206 women aged 46–54 years
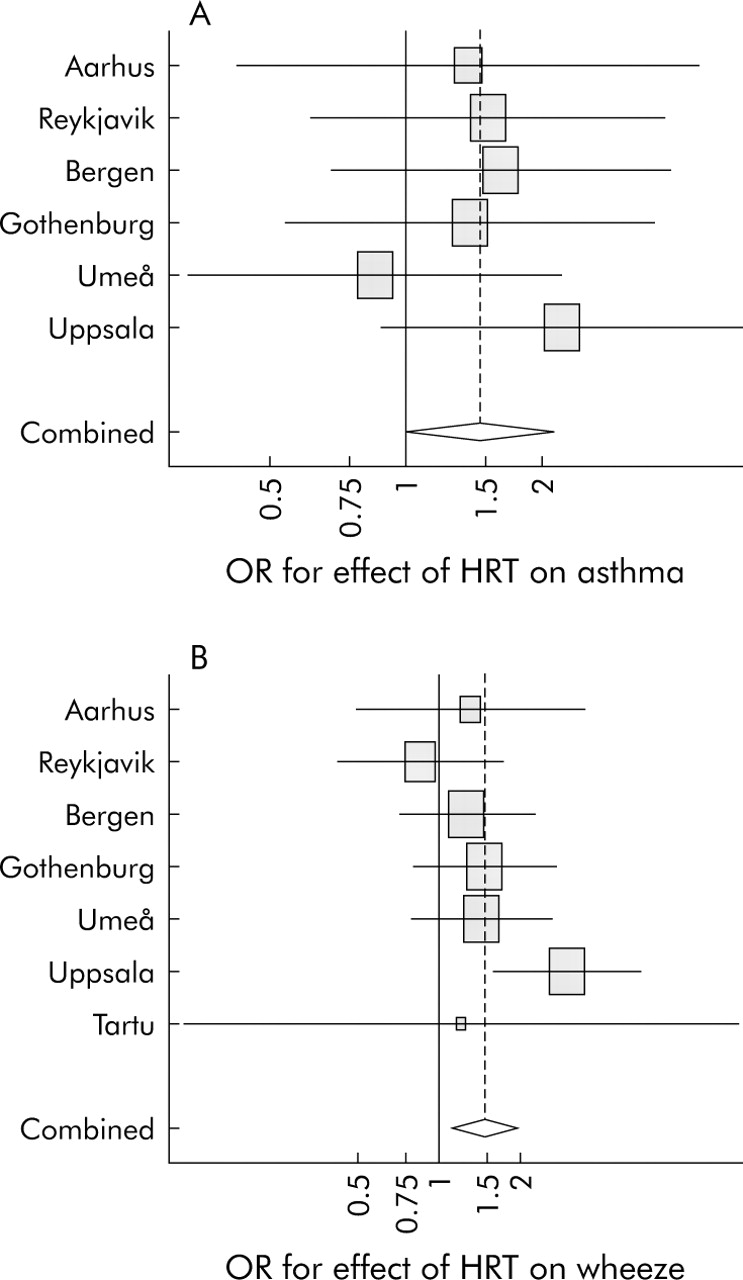
Odds ratios for the associations between (A) HRT and asthma by centre (Tartu not included because of small numbers) and (B) HRT and wheeze by centre. Adjustment within centre for smoking habits, BMI, age, and social class. For each centre, horizontal lines indicate 95% CI. For combined OR, diamond indicates 95% CI from model with centre as random effect. The size of each square is proportional to the sample size.
When stratifying by BMI in tertiles, HRT was significantly associated with a higher risk for asthma, wheeze and hay fever only among lean women (table 4). The associations between HRT and asthma and wheeze in women in the lower BMI tertile were significantly stronger than the corresponding associations in women in the medium and upper tertiles (pinteraction = 0.020 and 0.026, respectively).
Asthma and hay fever in women according to HRT use stratified by BMI in tertiles
Increasing BMI was associated with more asthma and asthma symptoms, but not with hay fever (table 5).
Asthma and hay fever according to BMI in tertiles, and adjusted associations of BMI with asthma and hay fever
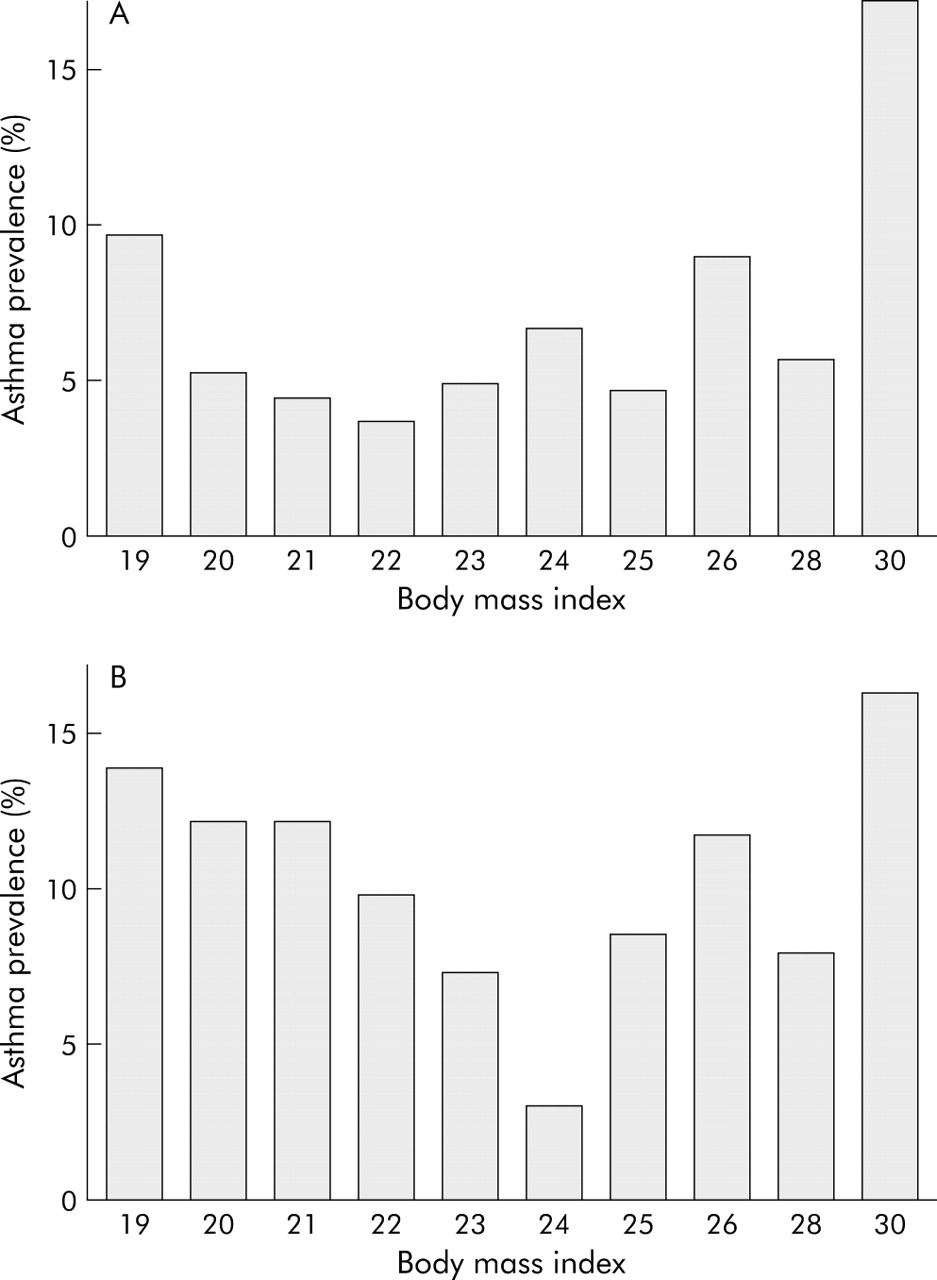
Stratifying by use of HRT, an association between asthma and BMI was observed in women not taking HRT (OR 1.10; 95% CI 1.05 to 1.14 per kg/m2; fig 2A) while no such association could be detected in women taking HRT (OR 1.00; 95% CI 0.92 to 1.08 per kg/m2; fig 2B). The difference in the associations between asthma and BMI according to use of HRT was significant (pinteraction = 0.046).

{kind=link}
{kind=link}
Asthma prevalence according to BMI in (A) 1648 subjects not taking HRT and (B) 535 subjects taking HRT.
The associations between HRT and asthma, wheeze and hay fever were only significant in never smokers (table 6), although the differences between smoking groups were not significant (pinteraction = 0.19, 0.6, and 0.4 for asthma, wheeze and hay fever, respectively).
Asthma and hay fever according to use of HRT, stratified by smoking history
DISCUSSION
The prevalence of diagnosed asthma, asthma symptoms, and allergy was higher among HRT users in a multicentre, population based, cross sectional survey of Northern European perimenopausal women. This was consistent between centres with different prescription practices. The risk for asthma related to HRT use was significantly greater in lean women than in heavier women, and this interaction in the effects of HRT and BMI on asthma was significant. The well documented association of asthma with BMI was observed only in women not taking exogenous sex hormones, while no significant association between asthma and BMI was found among HRT users. Exogenous oestrogens therefore appear to interfere with the mechanism causing more asthma among overweight women, resulting in a similar high prevalence of asthma in lean HRT users as that observed in obese women not taking HRT.
The observed higher prevalence of asthma among HRT users is in agreement with findings from the two large cohort studies, the Copenhagen City Heart Study and the Nurses’ Health Study.3–5 The interaction between BMI and HRT in the effects on asthma is supported by the Nurses’ Health Study in which the relative risk for HRT on asthma was 3.09 in lean women and 1.58 in heavier women.4 An association between HRT and hay fever has not been reported previously. Our study supports the findings of Lange et al5 who noted a stronger association of HRT with asthma among never smokers, possibly due to anti-oestrogen effects of smoking.26 Our findings are not necessarily contradictory to those of Carlson et al6 as we did not have data on lung function and our study population comprised much younger women.
The main limitation of the present study is its cross sectional design. Due to the lack of information about when the women started using HRT, we do not know with certainty whether or not HRT preceded asthma. Self-reported use of HRT is considered to be reliable.27 We did not have information about the type of HRT, but Barr et al4 did not observe differences with regard to type of HRT. Differential misclassification of asthma related to HRT use is a possibility; women taking HRT might have their asthma diagnosed more often because of a higher health awareness or more frequent contact with a doctor. The association between asthma and obesity might also be influenced by doctor bias. However, it seems unlikely that these sources of error explain our findings because the associations were consistent between centres with different prescription practices, the findings were similar for doctor diagnosed asthma and asthma symptoms such as wheeze, adjustment for social class did not alter the effects, and the associations between asthma and HRT differed significantly between lean women and those of normal weight. This interaction between HRT and BMI is biologically plausible but difficult to attribute to systematic error.
Women in the age group 46–54 years as included in this study are usually in the perimenopausal transition. The mean age of onset for the perimenopausal transition is 46 years and the mean duration is 5 years.24 This is the age when the climacteric symptoms are most frequent and the use of HRT most relevant. There is a possibility for residual confounding by menopausal status, but self-reported menopausal status is considered reliable even though some caution must be exerted.28 Differential misclassification of respiratory night symptoms as related to menopause could be suspected; night symptoms as opposed to other asthma symptoms appeared to be more common in menopausal women and less common in those taking HRT. There are some discrepancies in the current available literature about the role the onset of menopause plays in the development of pre-existing or new asthma and allergy. Some studies show a reduced asthma risk in naturally menopausal women3 while others suggest that asthma may start or worsen with the menopause.15 In our study menopause in itself was not significantly associated with asthma or hay fever.
Our study shows that the association between HRT and asthma appears to be modified by BMI. This is biologically plausible as there is a close interplay between sex hormones, fatty tissue, and metabolic status. A similar interaction has been described for breast cancer where the increase in relative risk among HRT users was greatest in lean women.20,29 The association between asthma and BMI is well documented although not fully understood.16–18 BMI is closely related to insulin resistance (IR),30,31 and we suggest that the association between asthma and BMI may be due to the pro-inflammatory effects of IR.31–33 There is no direct evidence linking asthma with IR, but several studies have shown an association between lung function and IR33–35 and a previous analysis of the present population showed an association between asthma and menstrual irregularity which is often a manifestation of IR.22
The effects of oestrogens on the airways appear to be complex. Both direct pro-inflammatory effects36,37 and indirect beneficial metabolic effects are described.38 Oestrogens are closely related to BMI, which is the strongest marker of oestrogen levels in postmenopausal women.9,12 IR is intimately involved in the regulation of local oestrogen production.13,19 We therefore hypothesise that exogenous oestrogens and BMI act on the airways in part through common pathways, where inflammation associated with IR might have an important role. In lean women with low IR the direct pro-inflammatory effects of HRT could be predominant, while in heavier and more insulin resistant women such effects might be counterbalanced by an oestrogen related reduction in IR.
In conclusion, our study shows an association between HRT and asthma and hay fever, and confirms the association of obesity with asthma. This study also reveals an interaction between HRT and BMI in the effects on asthma, HRT increasing the risk of asthma in lean women to the same level as that observed in obese women. These findings are fairly convincing as the interaction with BMI is biologically plausible and difficult to explain as error, even if the study design is not ideal. This study therefore indicates that asthma and allergy may be side effects of HRT, at least in subgroups of women. Furthermore, obesity and exogenous oestrogens may be involved in the pathogenesis of asthma through partly common pathways. Future studies of the effects of HRT on the airways should be conducted in representative general population samples, taking into account the possibility that the effects of oestrogens might be dependent on BMI or metabolic status. Likewise, further studies of asthma and BMI should take into consideration the hormonal status.
Acknowledgments
The following scientists in the Rhine study group are acknowledged for helpful contributions: T Blöndal, US Björnsdottir, G Boman, B Forsberg, D Gislason, A Gulsvik, M Gunnbjörnsdottir, E Juel Jensen, M-C Ledin, L Lillienberg, B Lundbäck, BN Lærum, E Norrman, A-C Olin, E Rydén, U Spetz-Nyström, K Stenudd Cashelunge, M Söderberg, J Talvik, A Tunsäter, G Wieslander.
REFERENCES
Supplementary materials
Files in this Data Supplement:
- [view PDF] - Correction.
Footnotes
-
Published Online First 21 October 2005
-
FGR was supported by a grant from the Norwegian Research Council. The study was supported financially by the Icelandic Research Council, the Swedish Heart and Lung Foundation, the Vårdal Foundation for Health Care Science and Allergy Research, the Swedish Association against Asthma and Allergy, the Norwegian Research Council project 135773/330, the Norwegian Asthma and Allergy Association, the Danish Lung Association, and the Estonian Science Foundation grant no 4350.
-
Competing interests: none.
-
The study was approved by local ethics committees in all the study centres.
Linked Articles
- Airwaves
- Correction