Article Text

Abstract
This report describes a 69 year old woman, suffering from active rheumatoid arthritis since the age of 60 and presenting with severe dyspnoea and cough. A computed tomography scan of the chest showed multiple bilateral pulmonary nodules, sometimes cavitated, associated with reticular opacities and pleural effusion. A videothoracoscopic excision of a cavitated nodule was performed. Seven days after surgery, a right pneumothorax developed, and the patient died of septicaemia one month later. Microscopically, the excised nodule was composed of necrotic fibrinoid material with a peripheral rim of palisaded histiocytes, extending to the pleural surface and containing several fungal hyphae morphologically consistent with aspergillus. A diagnosis of pulmonary rheumatoid nodule with fungus colonisation was made. In the lung, fungus colonisation is a rare complication of rheumatoid nodules. The most important differential diagnostic considerations are briefly discussed.
- rheumatoid nodule
- aspergillus
- lung
- bronchopleural fistula
Statistics from Altmetric.com
A wide spectrum of pleuropulmonary lesions are recognised in patients with rheumatoid arthritis. These include pleuritis, interstitial lung disease, bronchiolitis, vascular lesions, and rheumatoid nodules.1 Rheumatoid nodules are relatively infrequent, may be single or multiple, and are usually associated with similar subcutaneous nodules and active joint disease. Histologically, they are typically located in interlobular septa or pleura and are composed of fibrinoid necrosis surrounded by palisaded histiocytes with a rim of fibroinflammatory tissue and scattered giant cells. Rheumatoid nodules may occasionally undergo infection and cavitation, with secondary haemoptysis and bronchopleural fistulas with pneumothorax.1 We report a rare case of pulmonary rheumatoid nodule with fungus colonisation.
CASE REPORT
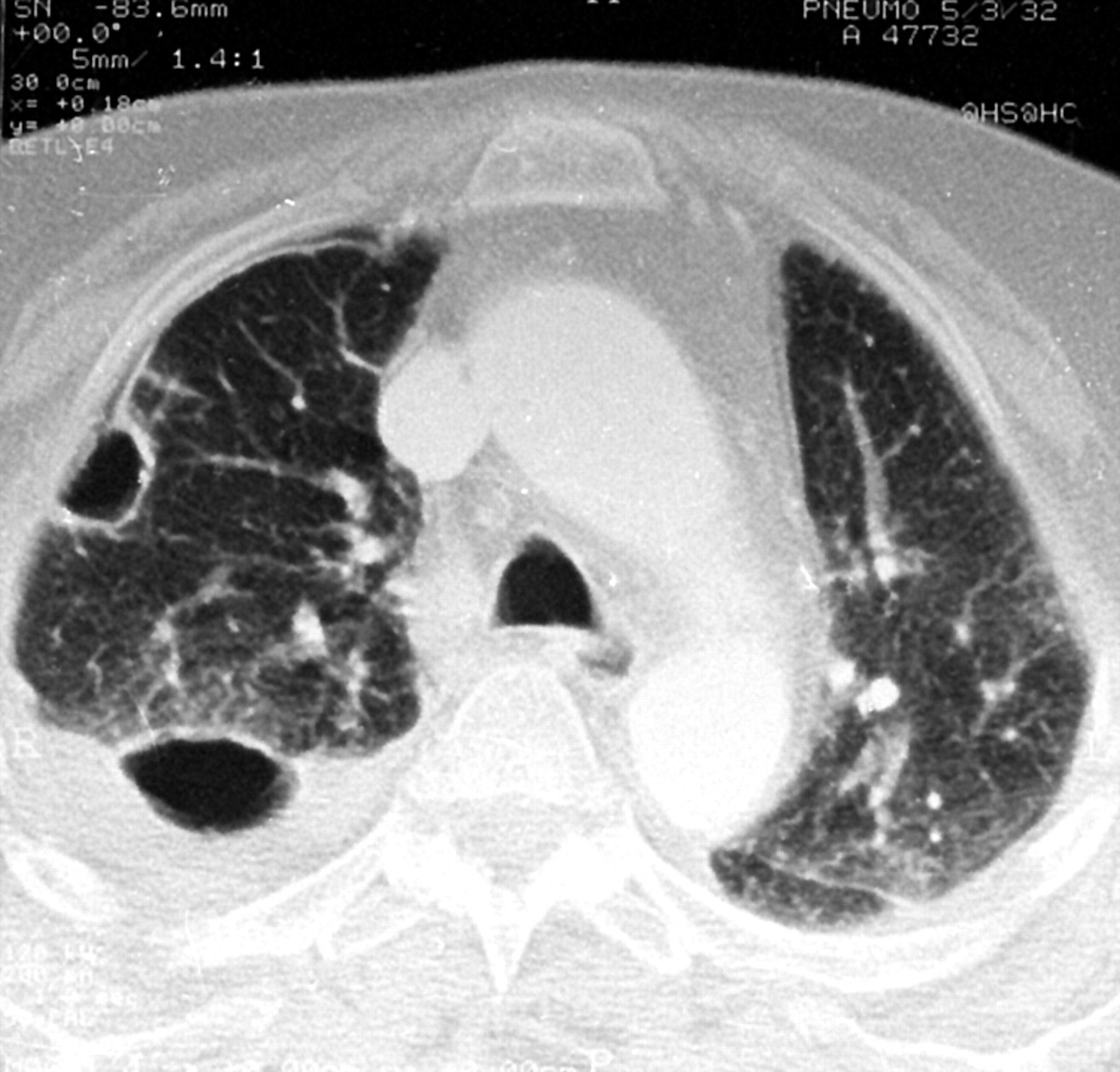
The patient, a 69 year old woman, was a smoker and presented with severe dyspnoea and cough. She had suffered from rheumatoid arthritis since the age of 60, with active synovitis and a rheuma test of 3440 mg/ml at admission (normal value, 1–20); for her rheumatological disease, she was being treated with corticosteroids and methotrexate. A chest x ray showed a right pleural effusion, and a thoracentesis obtained 500 ml of chylous fluid. Microbiological cultures of the pleural fluid were negative. A computed tomography scan of the chest (fig 1) showed multiple bilateral pulmonary nodules, sometimes cavitated, associated with reticular opacities. A right pneumothorax and a pleural effusion were also present. A videothoracoscopic excision of a cavitated nodule of the right upper lobe and lyses of multiple pleural adhesions were performed. Seven days after surgery, a recurrent right pneumothorax with persistent air leak developed. The patient died of septicaemia one month later. No necropsy was requested.

Thoracic computed tomography scan showing two subpleural cavitated nodules located in the upper lobe of the right lung. Bilateral reticular opacities and a right posterior pleural effusion are also visible.
Macroscopically, the segmentectomy specimen showed a well delimited cavitated nodule, 2.2 cm in diameter. Microscopically, the nodule was composed of necrotic, fibrinoid material, associated with scattered neutrophils and macrophages. The necrotic tissue extended to the pleural surface and into the lumen of several bronchioles, and contained numerous thin septate hyphae branching at acute angles, morphologically consistent with aspergillus (fig 2). At the periphery, a discontinuous rim of palisaded histiocytes, sometimes plurinucleated, merged with fibroinflammatory tissue, which extended into the surrounding lung parenchyma (fig 3). Fungi were limited to the necrotic foci: in particular, they were not seen in the surrounding lung or in the vascular walls. No vasculitis, well formed granulomas, or acid fast bacilli were demonstrated.

In the necrotic tissue, several fungal hyphae consistent with aspergillus are present (haematoxylin and eosin stain).

{kind=link}
{kind=link}
{kind=link}
The nodule is composed of necrotic material, surrounded by a rim of palisaded histiocytes merging with fibroinflammatory tissue (haematoxylin and eosin stain).
Take home messages
-
Rheumatoid nodules should be considered as a possible predisposing factor in pulmonary mycetoma
-
In patients with rheumatoid arthritis, a high index of suspicion for the diagnosis of pulmonary fungus infection should be maintained, both by clinicians facing cavitary nodules and by pathologists handling small biopsies with necrosis
-
Patients with rheumatological disease, particularly those receiving high dose intravenous immunosuppressive drugs, are at increased risk of life threatening aspergillus infections
DISCUSSION
This case represents a necrotising pulmonary lesion, with the classic clinical and histological features of a rheumatoid nodule. The most important differential diagnostic considerations are tuberculosis, bronchocentric granulomatosis,2 Wegener’s granulomatosis,3 and chronic necrotising aspergillosis.4 The first three possibilities can be excluded based not only on the clinical data, but also on the negativity of special stains for mycobacterium, and on some of the morphological details (for example, the lack of well formed necrotising granulomas typical of tuberculosis, and the absence of vasculitis and of multiple, scattered microabscesses characteristic of Wegener’s granulomatosis). Admittedly, it is more difficult to exclude with certainty a chronic necrotising aspergillosis (in other words, that the necrotising lesion we saw resulted exclusively from aspergillus infection, without a pre-existing rheumatoid nodule). However, in our opinion the morphology of the necrotic nodule and the absence of appreciable consolidation in the surrounding lung militate against this last possibility.
“The most important differential diagnostic considerations are tuberculosis, bronchocentric granulomatosis, Wegener’s granulomatosis, and chronic necrotising aspergillosis”
Our case is unusual for several reasons. First, the patient presented with recurrent spontaneous pneumothorax, probably secondary to a bronchopleural fistula, a rare but well recognised complication of rheumatoid nodule.5 Second, the presence of fungi in a pulmonary rheumatoid nodule is an extremely unusual phenomenon that, to the best of our knowledge, has been reported only once in the English language literature.6 Although in our case the fungi were morphologically consistent with aspergillus, the lack of culture confirmation precludes a firm conclusion about their exact classification. The fact that aspergillus can colonise a rheumatoid nodule is not surprising, considering the notorious propensity of the fungus to infect pre-existing pulmonary cavities, such as bronchiectasis, tuberculosis, cavitating carcinoma, and apical fibrobullous disease in patients with ankylosing spondylitis7 and rheumatoid arthritis.8 Moreover, patients with rheumatological disease, particularly those receiving high dose intravenous immunosuppressive drugs, are at increased risk of life threatening aspergillus infections.9
In conclusion, rheumatoid nodules should be considered as a possible predisposing cause of pulmonary mycetoma. In patients with rheumatoid arthritis, a high index of suspicion for the diagnosis of pulmonary fungus infection should be maintained, both by clinicians facing cavitary nodules and by pathologists handling small biopsies with necrosis.