Article Text

Abstract
Background Recent data show that there is an unexpectedly high prevalence of ‘inappropriate’ pulmonary responses to exercise among patients with systemic sclerosis (SS). However, no consensus exists as to which threshold of pulmonary artery systolic pressure (PASP) can be considered diagnostically relevant.
Aim To evaluate pulmonary vascular reserve and right ventricular function changes induced by exercise in SS patients without overt pulmonary arterial hypertension.
Methods and results The study enrolled 172 consecutive SS patients in NYHA class I–II, with a peak tricuspid regurgitant jet velocity at echocardiography not greater than 3 m/s, and 88 control subjects. Echocardiography was performed at rest and at the end of a maximal exercise test. SS patients showed a higher exercise-induced PASP than control subjects (36.9±8.7 vs 25.9±3.3 mm Hg, p=0.00008). The response to effort was higher in the presence of moderate interstitial lung disease (39.7±9.3 vs 36.0±8.4 mm Hg, p=0.016) or subclinical left ventricular diastolic dysfunction (42.3±5.8 vs 37.0±8.6 mm Hg, p=0.015). In control subjects, PASP values were normally distributed at rest and after exercise. In SS patients, the distribution was normal at rest but bimodal after exercise, with a second peak at 52.2 mm Hg including 13% of the total SS population. Patients in this subgroup showed subtle abnormalities of right ventricular function at rest and, most importantly, a blunted increase in right ventricular systolic function with exercise.
Conclusion Exercise echocardiography may identify a subset of SS patients with an inappropriate exercise-induced increase in PASP and early signs of right ventricular dysfunction.
- Systemic sclerosis
- stress echocardiography
- right ventricular function
- echocardiography-exercise
- pulmonary vascular disease
Statistics from Altmetric.com
- Systemic sclerosis
- stress echocardiography
- right ventricular function
- echocardiography-exercise
- pulmonary vascular disease
Introduction
Systemic sclerosis (SS) is a multisystem heterogeneous autoimmune disorder characterised by widespread vascular lesions and fibrosis of the skin and internal organs.1 Vascular involvement of the lungs leading to pulmonary arterial hypertension (PAH) is the most serious complication and a major cause of death in SS patients.2 3 Current guidelines recommend annual echocardiographic screening for the detection of pulmonary hypertension in asymptomatic patients with the scleroderma spectrum of diseases.4 However, echocardiography alone is limited by low sensitivity in the detection of pulmonary hypertension.5 6 Other screening strategies suggest evaluation of brain natriuretic peptide and diffusing capacity for carbon monoxide.7–11
Normality ranges for pulmonary artery pressure are well established for resting conditions, but normal values during exercise have not yet been defined.4 Although pulmonary artery systolic pressure (PASP) increases to some extent during exercise in normal individuals,12 13 an ‘inappropriate’ increase in PASP has been observed in patients with lung disease14 15 and SS.16 17
The aim of the present study was to evaluate pulmonary vascular reserve in SS patients without overt PAH. In particular, we hypothesised that even a mild to moderate degree of interstitial lung disease (ILD) or a poorer left ventricular (LV) diastolic function might be associated with a greater increase in PASP during exercise in such patients. Whether SS patients with an abnormal exercise-induced increase in PASP show early impairment of right ventricular (RV) function was a secondary prospective aim of the study.
Methods
Patients
SS patients consecutively admitted to two Italian Rheumatology Units (Second University of Naples and Fondazione IRCCS Policlinico S. Matteo of Pavia, Italy) from 1 September 2008 to 31 December 2009 were enrolled if they were in NYHA class I–II and had a peak tricuspid regurgitant jet velocity (TRV) ≤3 m/s at echocardiography (arbitrarily chosen as a cut-off value for normality). Exclusion criteria were the following: (1) previous diagnosis of PAH; (2) treatment with endothelin receptor antagonists, phosphodiesterase-5 inhibitors or prostanoids (continuous infusion); (3) coronary artery disease (angina pectoris, previous myocardial infarction, ECG and/or echocardiographic signs of myocardial ischaemia) and/or previous diagnosis of heart failure; (4) significant valvular heart disease; (5) atrial fibrillation/flutter; (6) interstitial lung disease at chest high-resolution CT (Kazerooni fibrosis score ≥16), and/or forced vital capacity <60% of the predicted value; (7) evidence of LV diastolic dysfunction at echocardiography (E/E′ ratio ≥15); (8) inability to perform an exercise stress test; and (9) poor quality imaging at echocardiography. All patients were investigated as described previously.18 Clinical characterisation of patients with SS was performed according to the European Scleroderma Trial and Research (EUSTAR) recommendations.19
ILD was considered present if chest high-resolution CT (HRCT) demonstrated compatible changes in reticular or air-space opacities. The extent of the individual HRCT scan patterns was estimated in each of five lobes, with five levels of scoring for ground glass and fibrosis as follows: (0) no abnormality; (1) <5% of the lobe; (2) 6–25% of the lobe; (3) 26–50% of the lobe; (4) 51–75% of the lobe; and (5) 76–100% of the lobe.20 Ground-glass opacity was defined as a hazy increase in lung parenchymal attenuation, and fibrosis score included lobular septal thickening and subpleural honeycomb changes. Table 1 shows the clinical and echocardiographic characteristics of the 172 SS patients enrolled in the study and of the age- and sex-matched control group of 88 normal subjects.
Clinical and echocardiographic characteristics of control subjects and patients with systemic sclerosis (SS)
All patients and control subjects underwent standard echocardiography and tissue Doppler imaging (TDI) at baseline and immediately after a maximal exercise test. The study was approved by the ethics committees of the two participating centres. Patients and control subjects were enrolled after giving written informed consent.
Echocardiography
Echocardiographic examinations were performed in the two participating centres using similar commercial equipment (Vivid 7; GE Medical Systems, Horten, Norway) and the same acquisition protocol.
PASP was calculated by adding a right atrial pressure estimate to the peak TRV; since inferior vena cava diameter and collapsibility were normal in all SS patients and control subjects, the right atrial estimate was always 5 mm Hg. LV peak early (E′) and late (A′) diastolic velocities were measured using TDI at the level of the lateral mitral annulus. RV peak systolic velocity (S), RV peak E′ and A′ diastolic velocities, and RV relaxation time were measured using TDI at the level of the lateral tricuspid annulus.
Stress echocardiography
The exercise stress test was symptom limited. It was performed using a standard protocol (increasing workload by 25 W every 2 min) until the patients experienced fatigue or symptoms, or until 85% of the age-predicted maximum heart rate was achieved. Because of the difficulties in obtaining good quality images while performing maximal exercise, and the necessity for several views for subsequent evaluation of pulmonary artery pressure, cardiac output and RV function, echocardiographic images were obtained immediately after exercise rather than at peak exercise. In all patients, however, the first parameter measured was the transtricuspid pressure gradient. In Naples, the tests were performed using a supine bicycle ergometer (American Echo, Kansas City, Missouri, USA), with a head tilt of 0–20° to obtain the best echo windows for imaging. In Pavia, the tests were performed on a bicycle ergometer, and at the end of the test the patients were rapidly moved onto a bed positioned nearby for echocardiographic acquisition (this usually required less than 30 s). At the end of exercise, the total time for data acquisition usually lasted no more than 2 min. To take into account predictable differences in exercise duration and CI changes during exercise between patients and control subjects, the increase in PASP during exercise was normalised by the increase in CI (ΔPASP/ΔCI).
All data were analysed off-line by two observers blinded to the patient conditions (MD and SG). Intraobserver and interobserver variability was less than 4.0% for measurements at rest and less than 6.0% at maximum exercise.
Statistical analysis
Continuous variables are reported as mean±SD and categorical variables as counts and frequencies. All data were adjusted for centres; therefore, the mean values obtained in each centre were used as covariates. Student's t test for paired and unpaired data was used to estimate differences between groups. To identify significant independent determinants of exercise-induced PASP, their individual association with clinical and echocardiographic variables was assessed by multivariate linear regression analysis. Variable selection was performed in the multivariate linear regression as an interactive stepwise backward elimination method, each time excluding the one variable with the highest p-value according to Wald statistics. The assumption of linearity was checked graphically by studying the smoothed martingale residuals from the null model plotted against the covariate variables. The linearity assumptions were satisfied. The Hosmer–Lemeshow goodness-of-fit test was used to check that the model adequately fit the data.
For descriptive analysis of PASP values at baseline and during exercise, QQ plots and the method of kernel density estimation were used.
For subgroup analysis, a Kazerooni fibrosis score of 11–15 at chest HRCT and/or forced vital capacity 60–70% of the predicted value were used as cut-offs to select patients with a moderate degree of ILD. Patients in the lowest quartile of LV E′/A′ ratio were categorised as those with a poorer LV diastolic function.
All analyses were performed using SPSS for Windows V.11.0. Differences were significant at p<0.05.
Results
Feasibility of stress echocardiography
A total of 212 consecutive SS patients were considered; 172/212 (81%) were enrolled and 40/212 (19%) were excluded. Nineteen of 40 were excluded because of inability to perform exercise (2 for recent leg injury, 12 for knee and/or hip pain, 5 for poor compliance) or poor quality imaging at echocardiography. A total of 106 consecutive control subjects were considered; 88/106 (83%) were enrolled and 18/106 (17%) were excluded. Nine of 18 were excluded because of inability to perform exercise or poor quality imaging at echocardiography. The total exclusion rate for inability to perform the exercise stress test or poor quality imaging at echocardiography was 9% in SS patients and 8% in control subjects.
Adjusting data for the centres and using the mean values obtained in each centre as covariates, no statistically significant differences were observed in demographic, clinical and echocardiographic parameters provided by the two participating centres (Naples and Pavia) in both control subjects (n=66 and n=22, respectively) and SS patients (n=89 and n=83, respectively).
Changes in PASP due to exercise
Although patients with increased resting PASP were not included in this study, PASP was higher at baseline in SS patients than in control subjects (p=0.00087, table 1). After exercise, SS patients showed both a higher PASP (p=0.00008) and a larger ΔPASP/ΔCI (p=0.00052) than control subjects (table 2).
Effects of exercise in control subjects and in patients with systemic sclerosis (SS)
The peak TRV was 3.0 m/s (range 1.9–3.9 m/s) in SS patients and 2.4 m/s (range 1.5–3.2 m/s) in control subjects (p=0.00012).
Exercise-induced changes in PASP according to ILD
Forty-three of 172 (25%) SS patients showed moderate ILD and 129/172 (75%) were free from ILD. Table 3 shows the response to exercise in SS patients according to the presence or absence of ILD.
Pulmonary artery pressure at rest and after exercise in systemic sclerosis patients with (ILD+) and without (ILD−) mild to moderate interstitial lung disease
Patients with a moderate degree of ILD had a significantly greater increase in PASP and ΔPASP/ΔCI during exercise (p=0.016 and p=0.041, respectively). Additionally, the increase in PASP and ΔPASP/ΔCI during exercise was greater in SS patients free from ILD than in control subjects (10.1±5.5 vs 5.3.±4.1 mm Hg, p=0.0022; and 4.2±3.3 vs 1.2±2.2 mm Hg/l/min/m2, p=0.00089). By multivariate linear regression analysis, after adjusting for potential confounders, presence of ILD was an independent determinant of PASP (β coefficient: 0.2; p=0.009) and ΔPASP/ΔCI during exercise (β coefficient: 1.9; p=0.012).
Exercise-induced changes in PASP according to LV diastolic function
Table 4 shows the response to exercise in SS patients according to LV diastolic function.
Pulmonary artery pressure at rest and after exercise in patients with systemic sclerosis according to the E′/A′ ratio measured at the lateral mitral annulus (lowest quartile vs highest quartile)
In patients having a more abnormal E′/A′ ratio at baseline (the lowest quartile of E′/A′ ratio), the exercise-induced increase in PASP and ΔPASP/ΔCI was higher compared to the other patients. By multivariate linear regression analysis, after adjusting for potential confounders, the presence of a poorer LV diastolic function (the lowest quartile of E′/A′ ratio) was an independent determinant of exercise PASP (β coefficient: 0.24; p=0.0071) and ΔPASP/ΔCI (β coefficient: 1.7; p=0.021). No other clinical features were associated with response to exercise.
Variability of PASP values at rest and after exercise
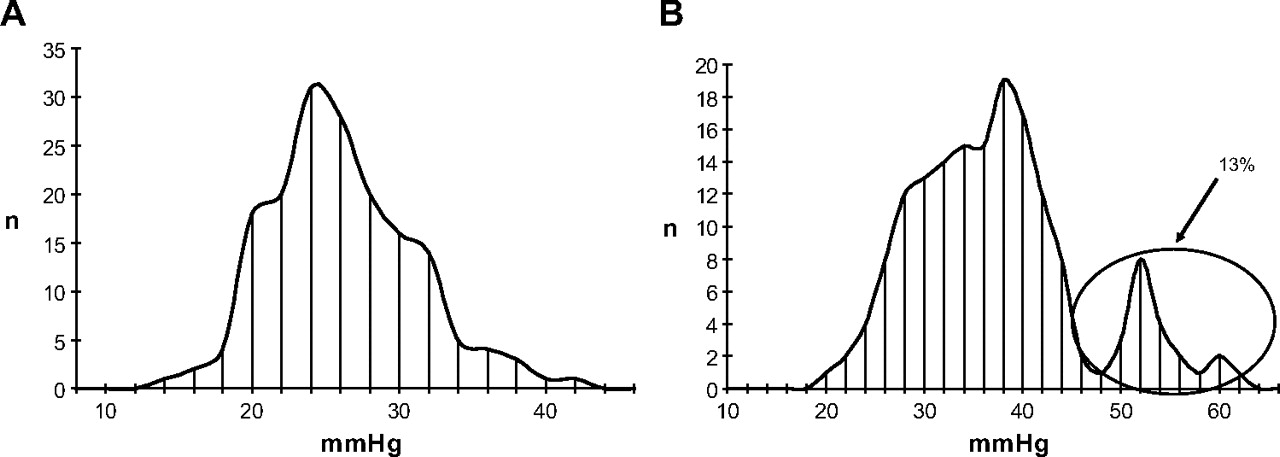
In control subjects, PASP values were normally distributed at rest (peak at 20.6 mm Hg) and after exercise (peak at 25.9 mm Hg) (figure 1). In SS patients, PASP values were normally distributed at rest (peak at 26.2 mm Hg); however, the distribution of exercise PASP was clearly bimodal, with a first peak at 37.8 mm Hg and a distinct second peak at 52.2 mm Hg. This peak included patients with a PASP of ≥48 mm Hg after exercise, which represented 13% of the total SS population (figure 2).

Distribution of pulmonary artery systolic pressure at baseline (A) and after exercise (B) in control subjects.

{kind=link}
{kind=link}
Distribution of pulmonary artery systolic pressure at baseline (A) and after exercise (B) in patients with systemic sclerosis.
The clinical and echocardiographic characteristics of the patients forming the second peak of exercise PASP were not different from those of the rest of the population (age 55±8.9 vs 55.9±12.7 years; systolic blood pressure 117±20 vs 118±23 mm Hg; prevalence of mild fibrosis 26.4 vs 24.5%; LV E′/A′ ratio 1.1±0.5 vs 1.2±0.6; baseline PASP 27.3±3.2 vs 26.5±3.6 mm Hg; baseline CI 2.9±0.8 vs 3.1±0.9 l/min/m2; all NS).
RV function at rest and after exercise
SS patients had a normal RV systolic function at rest. However, RV relaxation time was longer (p=0.00073) and the RV E′/A′ ratio was lower (p=0.0089) at TDI in SS patients than in control subjects. After exercise RV relaxation time was longer (p=0.0056), RV A′ wave was higher (p=0.0072), and the RV E′/A′ ratio was lower (p=0.00032) at TDI in SS patients than in control subjects (table 5).
Right ventricular function in control subjects and patients with systemic sclerosis (SS)
Additionally, in patients showing the largest exercise-induced increase in pulmonary pressure (PASP ≥48 mm Hg), the increase in tricuspid annulus plane systolic excursion with exercise was significantly lower than in the other patients (1.5±2.3 vs 5.2±3.8 mm, p=0.00001).
Discussion
The first conclusion of the present study is that even a mild to moderate degree of ILD or the presence of a poorer LV diastolic function may be important determinants of the increase in pulmonary pressure due to exercise in SS patients with normal resting PASP. This observation should make us cautious when trying to infer clinical significance from the results of stress echocardiography in individual patients with SS. However, this study also underlines that stress echocardiography may be a useful technique for screening patients with SS. In fact, variability analysis of the pressure response to exercise shows that there is a small subset of patients in whom the exercise-induced increase in PASP is higher than that not only of control subjects but also of the majority of SS patients.
Stress echocardiography in patients with SS
There is widespread consensus in the literature that the prevalence of apparently inappropriate pulmonary pressure responses to exercise among patients with SS and other autoimmune diseases is high.16–22 In a recent study by Huez et al,23 rest and stress echo evaluation was performed in 25 SS patients and 13 age-matched healthy controls. At basal evaluation some slight differences were found between the two groups. In particular, using TDI, the E maximal velocity at the tricuspid annulus was decreased and the isovolumic relaxation time corrected to RR interval was increased, suggesting the presence of right ventricular diastolic dysfunction. More interestingly, at exercise 18 SS patients showed no change in systolic right ventricular pressure gradient, but an increase in the slope of pulmonary artery pressure/flow relationships. These results suggest that SS patients may present with latent pulmonary hypertension as a likely cause of right ventricular diastolic dysfunction. Our findings of a longer RV relaxation time and a lower RV E′/A′ ratio in SS patients are consistent with these observations, being suggestive of a poorer right ventricular diastolic function and a larger ΔPASP/ΔCI—that is, impaired vascular reserve.
These data lend credit to the hypothesis that a reduction in pulmonary vascular reserve could be an early sign of vascular lung involvement in SS, which is likely to precede the development of overt PAH. The reasons for this are not clear. Al-Sabbagh et al24 performed morphometric measurements on pulmonary arteries in 58 patients with SS: they observed a larger area of the intima and percentage luminal occlusion in SS patients than in control subjects, providing a rationale for the poor response to vasodilator therapy in these patients. These features may underline a fixed vascular bed that is unable to respond by vasodilation to external stimuli.
Although this hypothesis is tempting and exhibits a pathological basis,24 it should be noted that the prevalence of ‘inappropriate’ responses is reported in the literature to be around 50%, a figure much higher than the prevalence of haemodynamically proven PAH among the general population of SS patients, which is reported to range from 7% to 12%.4 The reasons of such a discrepancy are unclear. The present study is the first one to show that among SS patients with normal resting PASP at echocardiography, even a mild to moderate degree of ILD (preferably during exercise-induced hypoxia) or the presence of subtle signs of LV diastolic dysfunction (even after exclusion of definite diastolic dysfunction) may be associated with a greater increase in PASP with exercise. In our study population, we did not measure oxygen saturation. According to the literature,25 26 however, we can hypothesise that exercise-induced hypoxia (ie, ILD patients) might have played a key role in inducing this response.
Therefore, the clinical implication of the present findings is that a hypertensive response to exercise does not necessarily disclose a small artery disease likely to further deteriorate over time, and this casts a shadow of uncertainty on the possibility of a widespread use of the exercise-induced increase in PASP as a predictor of future development of PAH in individual patients with SS.
More recently, in a multicentre study performed to analyse the distribution of TRV during exercise and hypoxia in relatives of patients with idiopathic and familial PAH, Grünig et al27 observed that a pulmonary hypertensive response to exercise and hypoxia in PAH relatives appears as a genetic trait with familial clustering, being correlated with but not caused by mutations of the bone morphogenetic protein receptor 2 gene. In addition, the density of TRV values exhibited a bimodal distribution in relatives, with a second peak representing the subgroup of subjects (10%) with a hypertensive TRV response to exercise and hypoxia. Similarly to what has been observed in relatives of PAH patients, in the present study variability analysis showed that a small subset of SS patients (13% of the total population) seems to react to exercise in a different and possibly pathological way. In fact, this analysis revealed a bimodal distribution of exercise PASP with a clearly distinct second peak including patients with an exercise PASP of ≥48 mm Hg. The mechanisms underlying such an exaggerated pulmonary pressure response are unknown at present.27 Finally, differently from Grünig et al,27 we did not observe a bimodal distribution in control subjects when analysing the density of TRV values at peak exercise. This is not surprising given the differences in size of the control populations (88 in the present study vs 191), mean age (55 vs 32 years) and sex (female 88% vs 48%). Follow-up studies will clarify whether this finding is associated with an increased risk of future development of PAH.
RV function in patients with SS
Data in the literature support the hypothesis that RV function can be impaired in SS, not only as a consequence of pulmonary hypertension but also probably as a result of small intramyocardial coronary involvement and/or patchy fibrosis.24 28–30 In the present study, SS patients showed subtle abnormalities of RV diastolic function at rest and after exercise; most importantly, those patients with the greatest abnormality of pulmonary vascular reserve also showed a blunted increase in RV systolic function with exercise. We acknowledge that the clinical significance of these abnormalities remains to be elucidated, and further studies are warranted to establish whether they are associated with a poorer long-term prognosis.
Study limitations
The study has some limitations.
Right heart catheterisation would have certainly provided more accurate information about pulmonary artery and right atrial pressures. However, it would have been impossible to perform invasive measurements of pulmonary artery pressure at baseline and during exercise in such a large number of SS patients as well as in normal control subjects. Despite all its limitations, echocardiography is considered the best screening tool for the assessment of pulmonary hypertension.4
The use of inferior cava vein diameter and collapsibility for estimating right arterial pressure is hypothetical and may infer inaccuracies to our data.
No pulmonary functional test was carried out in control subjects. As a consequence, no comparison between patients and controls was possible.
Echocardiographic acquisition was performed immediately after exercise, in order to obtain both the transtricuspid gradient and data for cardiac output and RV function analysis. This procedure may account for discrepancies with previous studies, in which pressure measurements were obtained at peak exercise. However, on the basis of the available data from the literature, we do not expect huge differences in PASP measured at peak or immediately after exercise.13
The results may not necessarily be extrapolated to the overall population of SS patients, since the present study enrolled relatively young and asymptomatic patients, with normal PASP at echocardiography, free from significant co-morbidities, who were able to perform a maximal exercise test.
Finally, no follow-up data are available to clarify the clinical implications of our findings. However, the predefined aim of the study was not to predict the development of PAH in SS patients, and it has to be acknowledged that predicting the development of PAH would require a long follow-up and most likely a larger population than the one enrolled in this study.
Conclusions
The present study indicates that caution is necessary in interpreting the results of exercise echocardiography in SS patients, since an abnormal pulmonary vascular reserve might be related to the presence of mild to moderate ILD or to subtle signs of LV diastolic dysfunction. This study, however, confirms that exercise echocardiography may disclose abnormalities of the pulmonary circulation in a small subset of patients with normal PASP at baseline. Although it is still unknown whether these patients are really at risk of future development of PAH, the presence of subtle abnormalities of RV diastolic function at rest and a blunted increase in RV systolic function after exercise seem to support the hypothesis that they do constitute a subgroup at higher risk.
References
Footnotes
See Editorial, p 94
MD'A and SG contributed equally in planning the study and in writing the manuscript.
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics committees of the Second University of Naples and Fondazione IRCCS Policlinico S. Matteo of Pavia, Italy.
Provenance and peer review Not commissioned; externally peer reviewed.