Article Text

Abstract
Objective: To compare compliance with and effectiveness of adaptive servoventilation (ASV) versus continuous positive airway pressure (CPAP) in patients with the central sleep apnoea syndrome (CSA) with Cheyne-Stokes respiration (CSR) and with congestive heart failure in terms of the apnoea–hypopnoea index (AHI), quality of life, and left ventricular ejection fraction (LVEF) over six months.
Methods: 25 patients (age 28–80 years, New York Heart Association (NYHA) class II–IV) with stable congestive heart failure and CSA-CSR were randomly assigned to either CPAP or ASV. At inclusion, both groups were comparable for NYHA class, LVEF, medical treatment, body mass index, and CSA-CSR.
Results: Both ASV and CPAP decreased the AHI but, noticeably, only ASV completely corrected CSA-CSR, with AHI below 10/h. At three months, compliance was comparable between ASV and CPAP; however, at six months compliance with CPAP was significantly less than with ASV. At six months, the improvement in quality of life was higher with ASV and only ASV induced a significant increase in LVEF.
Conclusion: These results suggest that patients with CSA-CSR may receive greater benefit from treatment with ASV than with CPAP.
- AHI, apnoea–hypopnoea index
- ASV, adaptive servoventilation
- CHF, congestive heart failure
- CPAP, continuous positive airway pressure
- CSA, central sleep apnoea syndrome
- CSR, Cheyne-Stokes respiration
- ESS, Epworth sleepiness scale
- LVEF, left ventricular ejection fraction
- MWT, maintenance of wakefulness test
- NYHA, New York Heart Association
- QOL, quality of life
- SAS, sleep apnoea syndrome
- Cheyne-Stokes respiration
- central sleep apnoea syndrome
- continuous positive airway pressure
- adaptive servoventilation
- heart failure
Statistics from Altmetric.com
- AHI, apnoea–hypopnoea index
- ASV, adaptive servoventilation
- CHF, congestive heart failure
- CPAP, continuous positive airway pressure
- CSA, central sleep apnoea syndrome
- CSR, Cheyne-Stokes respiration
- ESS, Epworth sleepiness scale
- LVEF, left ventricular ejection fraction
- MWT, maintenance of wakefulness test
- NYHA, New York Heart Association
- QOL, quality of life
- SAS, sleep apnoea syndrome
- Cheyne-Stokes respiration
- central sleep apnoea syndrome
- continuous positive airway pressure
- adaptive servoventilation
- heart failure
Cheyne-Stokes respiration (CSR) is a distinct pattern of periodic breathing with alternating crescendo–decrescendo sequences of hyperventilation and apnoea, often found in congestive heart failure (CHF).1 The detrimental consequence of the central sleep apnoea syndrome (CSA) with CSR (CSA-CSR) on the outcome of patients with CHF has long been known.2,3 This effect appears to be independent of other known risk factors, such as left ventricular ejection fraction (LVEF) or peak oxygen consumption. Haemodynamic improvement after pharmacological treatment for CHF is often associated with a significant decrease in CSA-CSR. However, persistent CSA-CSR, despite optimal pharmacological treatment, should be treated more aggressively. Its treatment with nocturnal continuous positive airway pressure (CPAP) was first described in 1990.4 CPAP, when it alleviates CSA-CSR, reduces sympathetic nervous system activity and improves LVEF.5 The effect of CPAP over a prolonged period has been found to improve ejection fraction and combined mortality–cardiac transplantation rate in a monocentric randomised study.6 However, CPAP did not always normalise the sleep apnoea syndrome (SAS). Adaptive servoventilation (ASV) (AutosetCS; ResMed Corp, San Diego, California, USA) is a novel therapy that provides positive expiratory airway pressure and inspiratory pressure support, which is servocontrolled based on the detection of CSR, with a backup respiratory rate. In a study with a randomised cross over design, ASV was shown to be more effective than CPAP or nasal oxygen in controlling central apnoeas and in improving sleep quality.7 In a one month randomised parallel trial versus placebo, ASV was recently reported to induce a significant improvement in daytime sleepiness, as well as in plasma brain natriuretic factor and catecholamine urinary excretion, both markers of CHF prognosis.8 No change was observed in patients with the placebo, which was subtherapeutic ASV.9 With the objective of comparing ASV with CPAP in the long term treatment of CSA-CSR in patients with heart failure, we have performed a six month, randomised, prospective, parallel comparison of therapeutic ASV versus CPAP and assessed compliance, apnoea–hypopnoea index (AHI), daytime sleepiness, quality of life (QOL), and LVEF after six months of either treatment.
METHODS
Study patients
This study was a prospective, parallel, randomised, multicentre trial. Patients between 18 and 80 years old, with stable CHF and newly diagnosed CSA-CSR by nocturnal polygraphy (Embletta, Flaga, distributed by ResMed SA, Lyon, France) with an AHI > 15/h were invited to participate in this study. CHF was defined by a medical history of heart failure, LVEF of ⩽ 45% at rest, assignment to New York Heart Association (NYHA) functional class II, III, or IV, and the absence, within the previous month, of exacerbations of heart failure while receiving stable optimal pharmacological treatment at the highest tolerable doses.
Sleep studies, daytime sleepiness, respiratory function, and cardiovascular assessment
Patients underwent a baseline overnight polysomnographic sleep study in a sleep laboratory. Sleep stages and arousals were scored according to standard criteria10 and an AHI was calculated.11 Nasal flow was evaluated with a nasal cannula together with an oral thermistor. Two channel (chest and abdomen) respiratory inductance plethysmography was also used to distinguish obstructive from central events, based on the absence of thoracoabdominal movements in case of central events. Oxyhaemoglobin saturation was monitored by oximetry. CSR was defined by the occurrence of crescendo–decrescendo periodic ventilation and CSA was defined by an AHI > 15/h with more than 80% of central apnoea–hypopnoea. The desaturation index was calculated as the number of dips > 3% from the baseline for each hour of sleep.
Daytime sleepiness was evaluated by the Epworth sleepiness scale (ESS) and the maintenance of wakefulness test (MWT) was performed the day after the overnight sleep study.12 Patients sat in a comfortable chair in the dark and were asked to resist sleep. Five 30 minute long tests were performed (at 0800, 1000, 1200, 1600, and 1800). Sleep onset was defined as the time from the lights being turned off to the first of three consecutive epochs of stage 1 non-rapid eye movement sleep or one epoch of any other sleep stage. Once sleep onset was identified, patients were awakened to prevent consolidated sleep improving their performance on the subsequent test. The mean latency of the five tests was calculated.
QOL was evaluated by the Minnesota living with heart failure questionnaire,13 which is a self administered test of 21 questions specifically assessing the limitations commonly associated with heart failure. The answer to each question ranges from 0 to 5; the lower the score, the better the QOL. LVEF was measured by a conventional radionuclide isotopic technique.
Intervention
After their baseline polysomnography, patients underwent the therapeutic trial. All patients were naïve to nocturnal ventilation. Patients adapted to a CPAP device during one night in the polysomnography laboratory to determine the effective pressure of CPAP and to check blood pressure tolerance to nocturnal ventilation and mask leaks. The ventilation was started with a nasal mask that was switched to a facial mask if leaks amounted to > 0.4 l/s. Airway pressure was manually increased from 4 cm H2O to the effective pressure, with a maximum of 12 cm H2O. The effective pressure was chosen as the pressure abolishing or significantly decreasing the CSR. Pressure was titrated with blood pressure monitoring: blood pressure was checked just before and five minutes after any increase in CPAP. In case of a blood pressure drop of > 20% from baseline after an increase in CPAP, the pressure was decreased by 1 cm H2O, blood pressure was checked, and the titration was interrupted if the blood pressure did not return to the previous value within five minutes.
On the next day, patients were randomly assigned to either CPAP set at the effective pressure or to ASV set to its default settings (expiratory pressure 5 cm H2O, inspiratory pressure support between 3–10 cm H2O, and back up respiratory rate 15 breaths/min).
Nocturnal ventilation was provided at day 0 by a non-profit home care company (ADEP Assistance), whose nurses checked blood pressure at rest and after 15 minutes of machine use on awake patients. The nurses came back to check tolerance to and compliance with treatment on the following day (day 1), on day 7, and then every month over the six month period of the study. Compliance was measured as the machine use (hours each night) given by the inbuilt counter.
The effectiveness of treatment on CSA-CSR evaluated by polysomnography and QOL were assessed at three months. QOL, polysomnography, MWT, ESS, and LVEF were measured at inclusion and at six months.
The study complied with the Declaration of Helsinki and was approved by a locally appointed ethics committee. All patients gave their informed consent to participate in the study.
Statistical analysis
Data are presented as mean (SD), unless otherwise stated. Unpaired t tests were used for normally distributed data and Mann-Whitney U tests were used for non-normally distributed data. Correlations were tested with the z test (StatView, version 5.0; Abacus Concepts, Berkeley, California, USA). Significance was considered for p < 0.05.
Compliance was compared after exclusion of the patient who underwent heart transplantation in the ASV group and of the two patients who died in the CPAP group. A compliance value of zero was assigned to the two patients in the ASV group and the three patients in the CPAP group who dropped out.
RESULTS
Patients
We screened 320 patients between April 2001 and November 2003. Thirty two met the inclusion criteria and 25 patients (28–80 years, NYHA class II–IV) were recruited. The remaining seven declined to participate in the study. Both randomisation groups were comparable in terms of clinical presentation, LVEF (range 18–44%), SAS, and sleepiness (table 1). Five patients in the ASV group and six in the CPAP group had atrial fibrillation. In the overall population of the study 92% were treated with diuretics, 64% with angiotensin converting enzyme (ACE) inhibitors, 72% with β blockers, and 76% with antiplatelets or anticoagulants. Medical treatment was comparable in both groups (table 1).
Baseline characteristics of both study groups
Twelve patients were allocated to the ASV group and 13 to the CPAP group. Eight patients dropped out of the study: three in the ASV group and five in the CPAP group. In the ASV group, one patient underwent heart transplantation (after three months) and two chose to discontinue ASV after four and five months. In the CPAP group, three patients discontinued CPAP (one at two weeks after initiation of treatment, one after one month, and one after four months) and two died, one of septic shock at one month of treatment and one of carcinoma at three months. In the CPAP group, mean effective pressure was 8.0 (1.8) cm H2O (range 5.0–10.0 cm H2O).
Effects on SAS and daytime sleepiness
In both groups nocturnal ventilation induced a significant decrease in AHI (fig 1A); however, the decrease in AHI obtained with ASV was significantly greater than that with CPAP, both at three and at six months (fig 1B). In the CPAP group, three patients had an AHI ⩾ 20/h at six months but they did not exhibit any particular clinical characteristics. No correlation was found between the effective pressure and the AHI at six months, suggesting that lack of effectiveness was not due to an insufficient level of CPAP. Noticeably, only ASV completely corrected CSA-CSR with normalisation of AHI (fig 1A).

Effect of nocturnal ventilation on apnoea-hypopnoea index (AHI (/h)). (A) Individual AHIs at baseline and after three and six months of treatment with either adaptive servoventilation (ASV) (left) or continuous positive airway pressure (CPAP) (right). (B) Difference between baseline AHI and AHI measured at three and six months. ASV induced a greater decrease in AHI than did CPAP. Data are mean (SD). *Significant difference.
Nocturnal ventilation induced a non-significant decrease in the ESS score (−3.0 (5.7) in the ASV group and −1.3 (3.2) in the CPAP group) and a non-significant increase in MWT time (1.1 (6.0) minutes in the ASV and 5.8 (6.9) minutes in the CPAP group). However, and in line with a previous report,9 those patients were not, or only a little, sleepy at baseline, with ESS score 8.0 (4.4) and MWT time 18.5 (8.5) minutes.
Compliance with treatment
Overall compliance with treatment was 4.7 (2.6) h/night at three months and 4.3 (3.1) h/night at six months. In contrast to ASV, compliance with CPAP significantly decreased over time (fig 2) and, therefore, compliance at six months was higher with ASV than with CPAP.

Compliance with nocturnal ventilation in both groups at three and six months treated with either ASV (left) or CPAP (right). One patient died and one discontinued nocturnal ventilation in the CPAP group before the third month, explaining why two points are reported as zero as early as three months. Compliance with ASV is significantly better with ASV than with CPAP at six months. Additionally, compliance with CPAP decreased significantly between three and six months. Data are mean (SD). *Significant difference.
Effects on cardiac function and on QOL
LVEF was measured at six months in only seven patients treated with ASV and six patients treated with CPAP. Despite these small numbers, a significant difference was found, as ASV induced a significant increase in LVEF, whereas CPAP had no effect (fig 3).

Changes in left ventricular ejection fraction (LVEF) obtained with either ASV or CPAP. Only ASV induced a significant increase in LVEF. Results are mean (SD). *Significant difference.
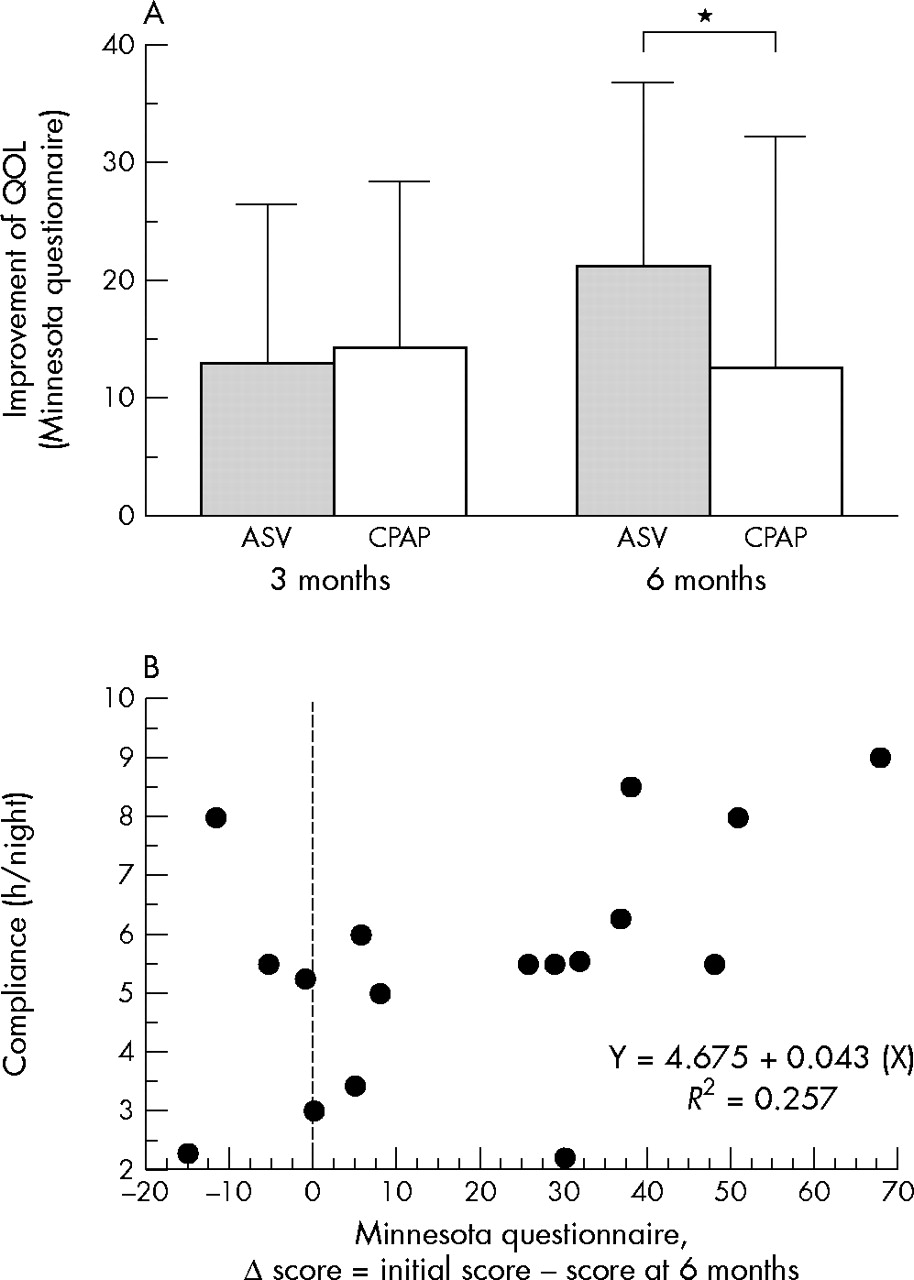
QOL was improved by either mode of nocturnal ventilation, as shown by the positive difference between the initial value of the score minus the value at the considered time point, either three or six months. However, the improvement in QOL was significantly higher with ASV than with CPAP after six months of treatment (fig 4A). A positive correlation was found between compliance with treatment measured at six months and the improvement in QOL (fig 4B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Change in quality of life (QOL) measured by the Minnesota living with heart failure questionnaire. The improvement in QOL is expressed by the positive difference between the baseline score minus the score at the considered time point, either three or six months. Both ASV and CPAP induced a significant improvement in QOL at three months, but the improvement observed after six months was significantly greater with ASV than with CPAP. Data are mean (SD). *Significant difference. (B) A significant positive correlation between compliance with treatment measured at six months and improvement in QOL was seen.
DISCUSSION
The present study was undertaken to compare compliance with and effectiveness of ASV versus CPAP over a long term, namely six months. This study shows that patients with CSR and symptomatic CHF treated by either ASV or CPAP comply well with nocturnal ventilation over six months but that treatment compliance is higher with ASV than with CPAP. We also showed that nocturnal ventilation improved both SAS and QOL, with ASV having a greater effect than CPAP. In addition, in this study only ASV induced a significant gain in LVEF over six months.
In previous studies,7,9 ASV was effective in correcting CSA-CSR and was more effective than CPAP. Additionally, CSA-CSR was always corrected with ASV, in contrast to CPAP. A previous study had shown that ASV was effective in correcting CSA-CSR and improving sleep, and that it was more effective than oxygen or CPAP.7 This partial response to CPAP is in line with some previous studies.5,14 Remarkably, some patients who responded to CPAP after three months of treatment did not respond at six months, whereas the effectiveness of ASV was consistent over six months. The method used in this study to apply CPAP was somewhat different from methods used in other studies, in which the target pressure was 10–12.5 cm H2O6 and was not based on a titration night. Here, the effective pressure for each patient was determined by both the haemodynamic tolerance to CPAP and the effectiveness of CPAP on CSA-CSR, leading to a lower mean pressure (8.0 (1.8) cm H2O). Taking the haemodynamic tolerance to CPAP into account may be important, as a potentially detrimental effect of CPAP has been underlined in an early report.15 Indeed, a reduction in cardiac output under CPAP has been described in the case of a patient with post-capillary wedge pressure < 12 cm H2O.16 Conversely, Bradley et al17 reported an increase in cardiac output and stroke volume with a low level (5 cm H2O) of CPAP. Accordingly, Baratz et al18 found an increase in cardiac output in seven of 13 patients with acute heart failure at several CPAP levels. Naughton et al19 showed that stroke volume index and cardiac index decreased significantly when CPAP (which was up to 10 cm H2O) was applied to healthy subjects but did not change in patients with CHF. Altogether, these results suggest that the effect of CPAP depends on the level of pressure and the initial haemodynamic status of the patient.
Compliance with treatment was in the range of what is usually reported for the use of CPAP to treat obstructive SAS. Adherence to treatment was also in the range of that usually reported for the treatment of conventional obstructive SAS with CPAP, where the dropout rate is from 5%20 to 37%.21 In the current study, three (23%) patients in the CPAP group and two (17%) in the ASV group discontinued the study secondary to nasal ventilation intolerance. The lack of adherence may be linked to absence of daytime sleepiness, as shown by an ESS score below 11, and to normal MWT times at inclusion, in line with previous studies that have suggested that non-sleepy patients with obstructive SAS have a low acceptance of CPAP.22,23 Patients who continued nocturnal ventilation over the study duration had good overall compliance with treatment. Interestingly, compliance with CPAP decreased significantly over time and became significantly lower than that with ASV at six months. The better compliance with ASV may be due to better comfort observed with bilevel ventilation, which may result from the lowering of the pressure at expiration, as suggested by some previous reports on the use of bilevel ventilation in obstructive SAS.24 The variation of pressure support, which is anticyclical to the CSR, may also be a source of increased comfort. Interestingly compliance at six months was correlated with the improvement in QOL, suggesting that compliance is a consequence of the subjective benefits that patients experience from their treatment, according to previous observations.22,23 Compliance may also reflect the effectiveness of treatment, in line with Pepperell et al,9 who showed superior compliance with therapeutic ASV than with subtherapeutic ASV.
The correction of CSA-CSR did not improve daytime sleepiness. However, our patients were not, or only moderately, sleepy at baseline and therefore a striking effect was not expected, in line with previous studies of non-sleepy patients.22,23 Hanly et al25 have reported that patients with CHF have more pronounced daytime sleepiness, but the measurement of sleepiness was based on multiple sleep latency tests that measure the propensity to get to sleep, and not the capability to resist sleep, in contrast to MWT. Accordingly, Pepperell et al9 recently studied the effect of ASV on daytime sleepiness as the capability to resist sleep by performing Osler tests. They found a significant improvement, which was not found, however, on the ESS.
In the present study, CPAP did not improve LVEF, in contrast to previous studies conducted in the treatment of both CSA-CSR6 and obstructive SAS.26 This may be due to the small number of patients in this study. Another hypothesis is that the lower mean CPAP pressure applied to our patients resulted in limited haemodynamic benefits from CPAP. On the other hand, using higher levels of CPAP may have detrimental consequences, as discussed above. A final hypothesis is based on the decrease in compliance with CPAP treatment observed over time, which may negatively influence the usually beneficial effect of CPAP on LVEF. This absence of an effect of CPAP on LVEF contrasts with the significant increase in LVEF observed with ASV. The effect of ASV on LVEF is in line with the results of Pepperell et al,9 who reported a significant decrease in plasma brain natriuretic peptide and urinary metadrenaline excretion after one month of treatment.
The acute beneficial effects of CPAP on the cardiovascular system in patients with CHF are well described and are thought to explain the improvement of physiological outcomes over periods of one to six months, as previously reported.6,27 Indeed, in patients with CHF, positive airway pressure has positive effects on cardiac haemodynamic function, as it increases intrathoracic pressure and augments stroke volume and cardiac output.17 CPAP also reduces left ventricular preload and afterload by decreasing left ventricular transmural pressures.28 However, the reduction in preload may be detrimental under certain conditions (see above).15 It has been previously suggested that atrial fibrillation should be envisaged as a potential detrimental factor in further reducing left ventricular preload during positive pressure application. In the present study, however, five patients in the CPAP group and six in the ASV group had atrial fibrillation, and this did not interfere with nocturnal ventilation. The reduction in preload is expected to be lower with ASV than with CPAP, as pressure support varies between inspiration and expiration and varies from one cycle to another. However, these safety data should be obtained in further studies. Additionally, ASV, as a bilevel ventilatory mode, may have a greater beneficial effect than CPAP on arterial oxygen pressure. Indeed, a greater increase in arterial oxygen pressure had been observed with conventional bilevel ventilation than with CPAP,16,29 thus contributing to a further decrease in sympathetic nervous system activity during sleep.
Another important finding of this study is the greater improvement obtained with ASV than with CPAP in QOL, along with an increase in LVEF. This improvement was more pronounced than that observed in some studies of other treatments for CHF. For example, a meta-analysis of cardiac resynchronisation showed a mean difference in the Minnesota score of 7.6 points (confidence interval 3.8 to 11.5 points),30 whereas the difference in the present study was twice this value. Improvement in fatigue and exercise capacity with treatment of CSA-CSR after nocturnal ventilation have previously been reported,31 as well as an improvement in inspiratory muscle strength,32 and both may contribute to improve QOL. Interestingly, compliance with treatment evaluated at six months was correlated with improvement in QOL, whereas it was not correlated with initial AHI, initial LVEF, or initial sleepiness. This improvement in QOL was noted despite a lack of significant effect on daytime sleepiness.
The present trial has limitations, the first one being the small number of patients. However, despite this small number, significant differences were noted between ASV and CPAP, consistent with previous results on ASV7,9 and with complete correction of CSA-CSR obtained with such a ventilation mode. Blinding was also not possible but study personnel who took polysomnography readings and LVEF measurements were blinded to the treatment assigned to patients.
On the other hand, only a few randomised studies have compared two ventilation modes in treating SAS.33 In CSA-CSR, only one study compared long term CPAP with another mode (bilevel pressure support) and showed that both modes were equally effective.34
In summary, our study showed that both CPAP and ASV decrease AHI but that ASV induced a greater decrease in AHI than did CPAP, with a consistent normalisation of AHI. Compliance with treatment decreased significantly over time with CPAP, whereas it remained stable with ASV. This may have contributed to the increase in LVEF and to the improvement in QOL observed with ASV. These results suggest that patients may benefit more from treatment of CSA-CSR with ASV than with CPAP.
Acknowledgments
We are indebted to Marie-Françoise Bigi, Djibril Bokar-Thire, Ahmed Hchikat, and Laurent Margarit (sleep technicians, Hôpital Henri Mondor) for their technical help throughout the study and for the care of patients. We thank Rolland Baruch, Margaret Dyane, Valérie Gaërel, Sylvie Montfollet, Guillaume Raverdy, and Catherine Salé (ADEP Assistance) for care provided to patients at home. The study was performed with the help of the Service de Pharmacologie Clinique and of the Centre d’Investigation Clinique (Hôpital Henri Mondor, AP-HP, Créteil, France). We also thank Suzan Sortor-Leger, Gentiane Rouffet (ResMed Corp, Lyons, France), and Alison Hansford (Resmed Corp, Sydney, Australia) for their technical support.
REFERENCES
Footnotes
-
Published Online First 20 June 2005
-
Competing interests: the study was supported by non-profit organisation funds (ADEP Assistance) and a non-commercial donation made by ResMed France to support research in the Créteil Sleep Laboratory in 2001. CP and M-P d’O were reimbursed by ResMed for travel expenses to attend the American Thoracic Society Annual Conference 2004; SR is employed by ADEP Assistance, which is a non-profit organisation for home care. Other authors have no declared conflict of interest.