Article Text

Abstract
OBJECTIVE To determine the effect of adjunctive prednisolone on morbidity, pericardial fluid resolution, and mortality in HIV seropositive patients with effusive tuberculous pericarditis.
DESIGN Double blind randomised placebo controlled trial.
SETTING Two medical school affiliated referral hospitals in Harare, Zimbabwe.
PATIENTS 58 HIV seropositive patients aged 18–55 years with tuberculous pericarditis.
INTERVENTIONS All patients received standard short course antituberculous chemotherapy and were randomly assigned to receive prednisolone or placebo for six weeks.
MAIN OUTCOME MEASURES Clinical improvement, echocardiographic and radiologic pericardial fluid resolution, and death.
RESULTS 29 patients were assigned to prednisolone and 29 to placebo. After 18 months of follow up there were five deaths in the prednisolone treated group and 10 deaths in the placebo group. Mortality was significantly lower in the prednisolone group (log rank χ2 = 8.19, df = 1, p = 0.004). Resolution of raised jugular venous pressure (p = 0.017), hepatomegaly (p = 0.007), and ascites (p = 0.015), and improvement in physical activity (p = 0.02), were significantly more rapid in the prednisolone treated patients. However, there was no difference in the rate of radiologic and echocardiographic resolution of pericardial effusion.
CONCLUSIONS Adjunctive prednisolone for effusive tuberculous pericarditis produced a pronounced reduction in mortality. It is suggested prednisolone should be added to standard short course chemotherapy to treat HIV related effusive tuberculous pericarditis.
- tuberculous pericarditis
- HIV infection
- echocardiography
- prednisolone
Statistics from Altmetric.com
There has been a major increase in the incidence of tuberculosis in the past decade, largely as a result of the HIV epidemic.1-3 In particular the proportion of tuberculosis patients presenting with extrapulmonary disease has increased.4 Several reports have documented the relation of pericardial tuberculosis and HIV infection, with seropositivity being observed in 67–92% of patients.5-7 Survival is adversely affected in patients co-infected with tuberculosis and HIV.8
The treatment of tuberculous pericarditis in HIV seronegative individuals consists of standard antituberculous chemotherapy, including currently accepted short course regimens.9-11This treatment has been extended to HIV seropositive individuals, and the impression is that the outcome of treatment may be as good as in HIV seronegative patients, at least in the short term.2 ,4However, HIV seropositive patients have a higher rate of side effects from standard treatment regimens, and there is concern that these patients may have a higher relapse rate.4 Another concern is that the use of adjunctive corticosteroids in HIV seropositive individuals may increase the risk of bacterial and viral infections and Kaposi's sarcoma.12 ,13 Moreover, use of adjunctive corticosteroids in tuberculous pericarditis remains controversial, even in non-HIV infected individuals.10-14 In non-randomised15-17 and randomised studies18 19 of tuberculous pericarditis, rapid improvement of symptoms and reduced mortality has been suggested with the use of adjunctive corticosteroids in non-HIV infected individuals. A systematic review of 543 patients in three trials, however, concluded that prednisolone has no clear beneficial effect in patients with tuberculous pericarditis.20 None of these studies, however, addressed HIV seropositive patients, yet at present the greatest impact of tuberculous pericarditis is among HIV seropositive individuals. The aim of this study was, therefore, to determine the effect of adjunctive prednisolone on morbidity, pericardial fluid resolution, and mortality in HIV seropositive individuals with tuberculous pericarditis treated with a standard antituberculous regimen.
Subjects and methods
DESIGN
This was a double blind randomised placebo controlled trial of patients with tuberculous pericarditis and HIV infection. Patients were enrolled at two medical school affiliated referral hospitals in Harare city. Ethical approval was obtained from the Zimbabwe Medical Research Council. All patients gave written informed consent and received counselling for HIV antibody testing. Patients who declined testing were not entered into the trial.
PATIENTS
Eligibility criteria were: (a) age 18–55 years; (b) residence in Harare city to ensure good follow up; (c) HIV seropositive; (d) no diagnosis of tuberculosis within the past two years; (e) large pericardial effusion on echocardiography (> 1 cm anteriorly and > 1 cm posteriorly; and (f) pericardial aspirate with > 50% lymphocytes and protein content > 30 g/l. Exclusion criteria were: (a) antituberculous treatment started more than 48 hours before recruitment; (b) corticosteroid treatment within previous one month; (c) presence of Kaposi's sarcoma or any other malignancy; (d) coexisting life threatening disease; (e) bacterial pneumonia; (f) pregnancy; (g) cavitating pulmonary tuberculosis; and (h) other causes of pericardial effusion.
Demographic and clinical characteristics were obtained at baseline, including HIV related features.
DEFINITION OF PERICARDIAL TUBERCULOSIS
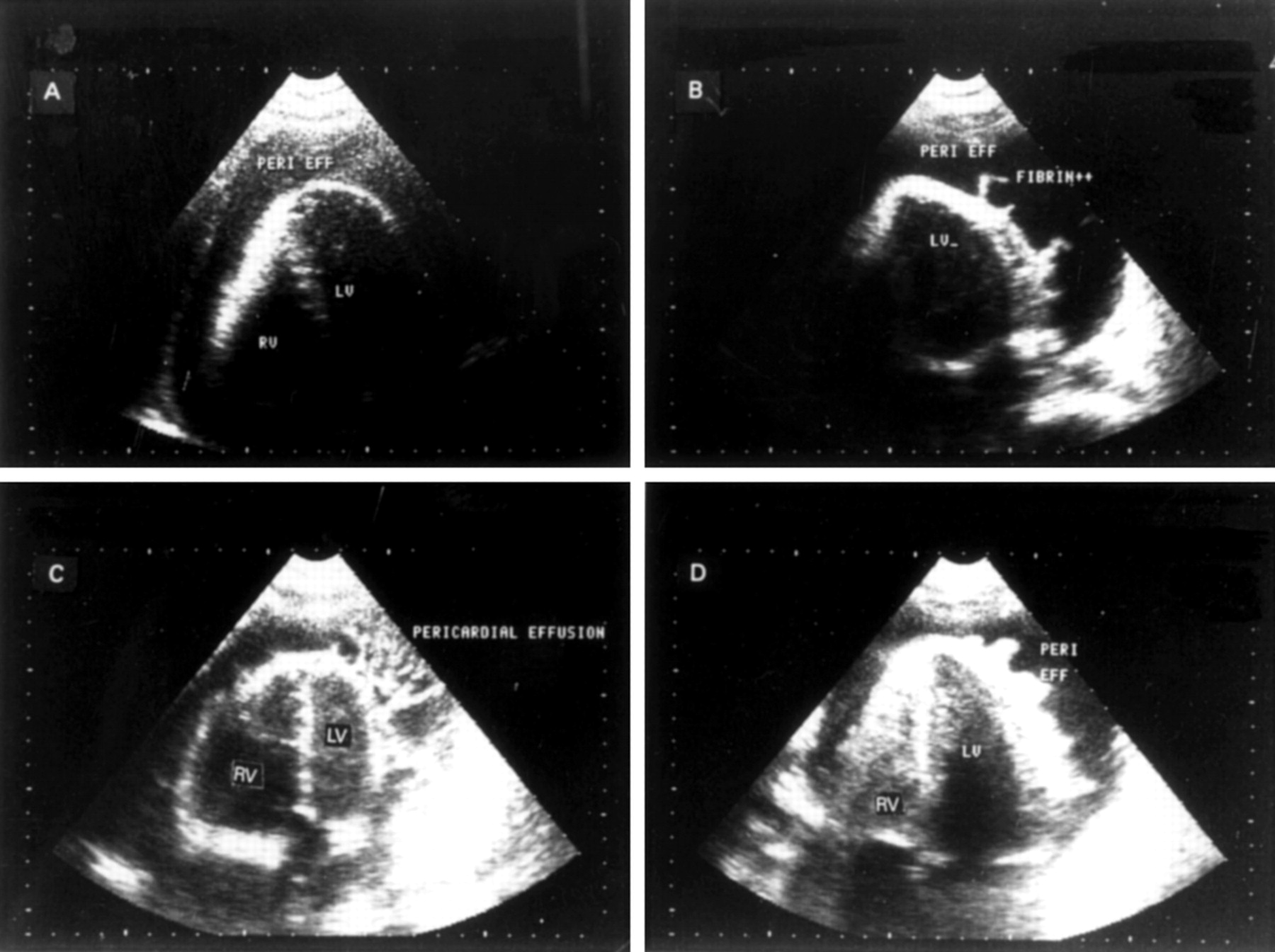
Patients were admitted into the study on the basis of an echocardiographic demonstration of a large fibrinous pericardial effusion and a clinical diagnosis of tuberculous pericarditis, supported by a high lymphocyte count and a high protein content in the pericardial aspirate. Diagnostic and/or therapeutic pericardiocentesis was undertaken in all patients. The typical two dimensional (cross sectional) echocardiography appearance of tuberculous pericarditis was a thickened pericardium with layers of shaggy echoes lining both visceral and parietal pericardium as previously described,21 but various appearances were observed. Clinical examination and appropriate tests excluded alternative causes of pericarditis.
TREATMENT AND RANDOMISATION TO PREDNISOLONE
All patients received a standard short course anti tuberculous regimen in accordance with national guidelines.22 This included rifampicin, isoniazid, pyrazinamide, and ethambutol for two months, followed by rifampicin and isoniazid for a further four months in standard doses. Prednisolone and placebo were made as identical “5 mg” tablets. The intervention consisted of prednisolone/placebo tablets starting at a dose of 60 mg (12 tablets) and tapering by 10 mg per week until completion at the end of the sixth week. Randomisation was achieved by the use of a computer generated randomisation list with an equal number of patients assigned to receive prednisolone and placebo. Prednisolone/placebo packages were prepared according to the randomisation list, but labelled with the study number only. A package consisted of six well labelled bottles each containing the number of tablets required in each of the six weeks of the intervention. Eligible patients were given a drug package consecutively working down the randomisation list. Clinicians and patients were blinded to the identity of the tablets. A randomisation code list was kept sealed and was released at the end of the study.
LABORATORY MEASUREMENTS AND FOLLOW UP ASSESSMENT
Pericardial fluid specimens (5 ml) were immediately injected onto Lowenstein-Jensen slope and into double strength Kirchner medium, and transported to the National Tuberculosis Reference Laboratory in Bulawayo, for smear, culture, and identification of isolates. Pericardial fluid smears were stained for acid–alcohol fast bacilli using Ziehl–Neelsen stain. The CD4+ lymphocyte count was determined at recruitment by immunostaining of whole blood smears with a mouse anti-CD4 monoclonal antibody (Dako, Glostrup, Denmark).23Visits were scheduled weekly for the first eight weeks, two monthly up to six months, then three monthly up to 18 months. Patients made additional visits whenever they felt unwell. At every visit patients were assessed clinically for features of ongoing tuberculosis, pericardial disease (effusion, tamponade, and constriction), side effects of medication (antituberculous drugs and prednisolone), sense of wellbeing, and functional capacity. Every two weeks during the first two months and subsequently at every visit laboratory tests, chest radiography, electrocardiography, and echocardiography were performed. Compliance was assessed by pill count at each visit during the period of drug treatment.
ECHOCARDIOGRAPHIC EXAMINATION
Two commercially available echocardiography machines (Phillips and Kretz) were used for echocardiographic examinations. JGH and IT with extensive experience of echocardiography in this setting performed all examinations. A standard protocol was used with examinations in the left parasternal long and short axes, apical two and four chamber and subcostal views. Additional views were dictated by the requirements of the individual case. Before the study the two cardiologists had joint sessions on 10 patients with large pericardial effusions and developed consensus on criteria for measurement of pericardial fluid size in the anterior, posterior, and subcostal views and the diagnosis of constrictive pericarditis.
END POINTS
The planned total observation period for each patient was 18 months from entry into the study, but patients continued to be seen until the censor date, 22 January 1997. The primary end points were resolution of pericardial effusion and death. The secondary end points were resolution of pretreatment symptoms and signs, low voltage ECG, and corticosteroid related adverse effects. The diagnosis of constrictive pericarditis was made on the basis of a combination of clinical and echocardiographic features.24 We were interested in observing complications that could be attributed to the use of prednisolone in HIV infected individuals such as increased bacterial and viral infections, and the development of Kaposi's sarcoma. Low voltage on the ECG was defined as a QRS complex of < 6 mm in V5 or V6 and < 4 mm in the limb leads, a definition used in previous studies.18 ,19
STATISTICAL ANALYSIS
All analyses were performed on an intention-to-treat basis with two sided p values. Baseline characteristics were compared using Student's t test and Kruskal–Wallis test for non-normally distributed continuous variables. The χ2test with Yate's correction was used for categorical variables; where expected values were < 5, the Fisher's exact test was used. The log rank statistic was used to compare the survival experience in the two treatment groups. Survival analysis was constructed using Kaplan–Meier plots. Values of p < 0.05 were regarded as significant. The statistical package STATA version 5 (Stata Corporation, USA) and SPSS-PC version 6.11 PROC MIXED were used for statistical analysis.
Results
All our patients were presumed to have contracted HIV infection through heterosexual contact. No patient admitted to homosexual or bisexual activity or use of illicit intravenous drugs. None gave a history of transfusion of blood products in the past. There was no direct indication as to when each might have acquired HIV infection prior to the study.
BASELINE DEMOGRAPHIC AND CLINICAL CHARACTERISTICS
Of the 58 patients entered into the study, 29 were randomised to prednisolone and 29 to placebo. There was no significant difference between the two treatment groups with regard to demographic and clinical variables (table 1). Generalised peripheral lymphadenopathy was noted in 81% of patients, but other HIV related features were infrequent and were comparable in the two groups.
Baseline demographic and clinical characteristics
LABORATORY FEATURES
Baseline haematologic, liver function tests, radiologic, electrocardiographic and echocardiographic findings were comparable between the treatment groups (table 2). Overall anaemia (haemoglobin < 12 g/dl) was found in 74% and hypoalbuminaemia (< 30 g/l) in 61% of patients; 54% of patients had CD4+ counts between 200 and 500 cells/μl.
Baseline laboratory findings
CONFIRMATION OF TUBERCULOSIS DIAGNOSIS
In total 22 (38%) pericardial fluid specimens grewMycobacterium tuberculosis on either Lowenstein–Jensen and/or double strength Kirchner media. Twelve cultures (41%) in the prednisolone group and 10 (35%) in the placebo group were positive for M tuberculosis(χ2 = 0.07, df = 1, p = 0.787).
REGRESSION OF PERICARDIAL EFFUSION: RADIOLOGICAL AND ECHOCARDIOGRAPHIC FINDINGS
Although prednisolone appeared to bring about a more rapid decrease in radiological cardiothoracic ratio and echocardiographic resolution of pericardial effusion (fig 1), these were not significant (figs 2 and3).
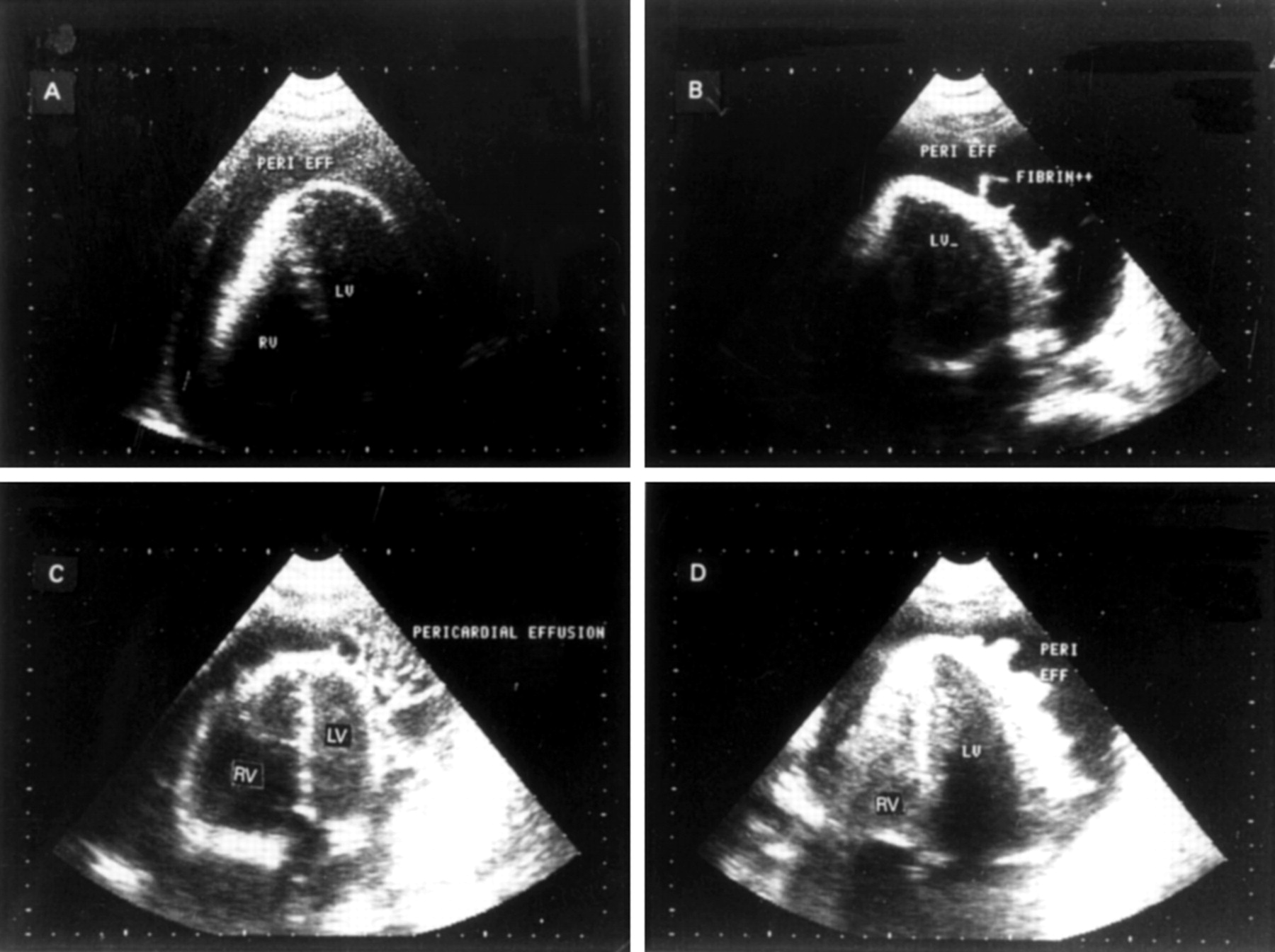
Echocardiographic apical views showing various appearances of tuberculous pericardial effusion in four study patients. (A) Effusion appears as a homogenous moderately echo dense collection. (B) Echo lucent fluid with fimbria-like fibrinous strands. (C) Fibrinous strands organised as clumps of meshwork within a mildly echo dense effusion. (D) A layer of shaggy fibrin arranged uniformly around the heart with no evidence of constriction. Peri eff, pericardial effusion; LV, left ventricle; RV, right ventricle.

Cardiothoracic ratio measured serially in the prednisolone and placebo treatment groups. Difference not significant (p = 0.80).
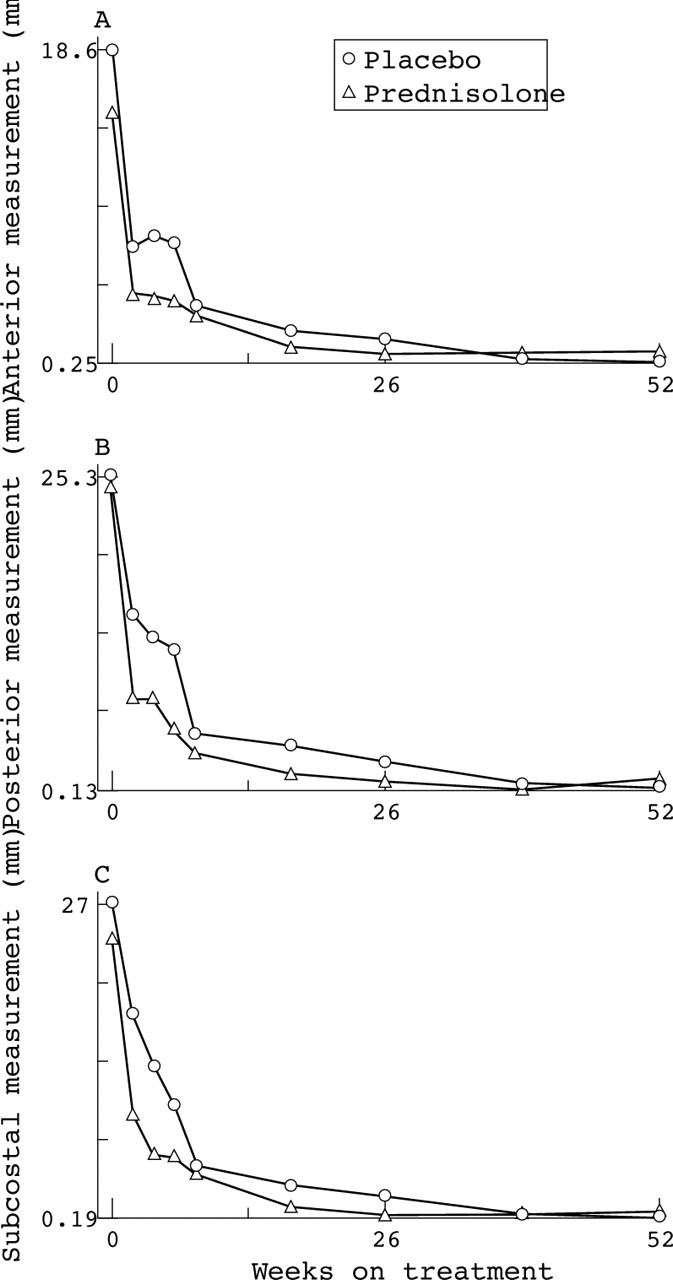
Pericardial fluid regression serial echocardiographic measurements of fluid in the (A) anterior, (B) posterior, and (C) subcostal views. Differences not significant: anterior p = 0.19; posterior p = 0.80; subcostal p = 0.39.
MORTALITY
Kaplan–Meier plots of survival in prednisolone and placebo treated patients over 18 months of follow up are shown in fig 4. Three deaths occurred within one week of introduction of antituberculous treatment (one in the prednisolone and two in the placebo group). In the first six months of treatment nine deaths occurred among the 58 patients—one in the prednisolone group and eight in the placebo group. At the end of the study five deaths were recorded in the prednisolone group and 10 in the placebo group; the difference was significant (log rank χ2 = 8.17 p = 0.004). Of the nine deaths which occurred in the six months of antituberculous treatment, three were caused by disseminated tuberculosis, five were caused by a combination of disseminated tuberculosis and ongoing active pericarditis, and one was caused by disseminated tuberculosis, active pericarditis, and possibly pulmonary Kaposi's sarcoma. None of these nine deaths were caused by constrictive pericarditis. Deaths after the six months of treatment were caused by various HIV related conditions: HIV wasting disease (three patients), pneumonia (two patients), and meningitis (one patient).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier plots of survival in prednisolone and placebo treated patients over 18 months of follow up. Significant difference in mortality, log rank χ2 = 8.17, df = 1, p = 0.004.
MORBIDITY
Improvement in physical activity (p = 0.02) and resolution of raised jugular venous pressure (p = 0.017), hepatomegaly (p = 0.007) and ascites (p = 0.015) were faster in prednisolone treated patients compared with those given placebo. No significant difference was observed in the rate of resolution or in improvement of the other predefined clinical features and low voltage ECG. Constrictive pericarditis occurred in four patients, two in each treatment group.
ADVERSE EVENTS DURING TREATMENT
During the entire study period 51 complications were observed: 30 in the prednisolone group and 21 in the placebo group. These were Kaposi's sarcoma (3), herpes zoster (2), herpes labialis (1), pneumonia (16), acne (8), skin rash (13), and others (8). There was no significant difference in the frequency of complications between the treatment groups. All three cases of Kaposi's sarcoma were observed in placebo treated patients.
COMPLIANCE WITH TREATMENT
There was significantly better compliance with treatment in the prednisolone group compared with the placebo group. Two hundred and thirteen tablet counts were performed in the prednisolone group with 169 (79.3%) counts showing that > 90% of tablets had been consumed. In the placebo group 182 counts were performed with 119 (65.4%) counts showing that > 90% tablets were consumed (χ2 = 9.73, df = 2, p = 0.008). However, there was no association between compliance and mortality during the six months of antituberculous treatment (p = 0.104).
Discussion
TUBERCULOUS PERICARDITIS
There has been a rapid rise in the incidence of tuberculosis, with a disproportionate increase in extrapulmonary tuberculosis in sub-Saharan Africa, as a result of the HIV epidemic.2 ,25In 1987 extrapulmonary tuberculosis accounted for 15.2% of tuberculosis cases in Harare city, but a decade later this figure was 23.5%.26
CORTICOSTEROIDS IN TUBERCULOSIS
The use of corticosteroids in conjunction with antituberculous drugs has been shown to be of benefit in HIV seronegative individuals with tuberculous pericarditis, meningitis, and pleural disease.27 Earlier uncontrolled studies suggested improved outcome in tuberculous pericarditis with their use,15 but it was only in the 1980s that randomised controlled studies have shown benefit,18 ,19 though this has been disputed in a systematic review.20 In these studies adjunctive corticosteroid treatment reduced mortality and had favourable clinical effects.18 ,19 However, these studies were carried out on HIV seronegative patients, and such benefit should not be extrapolated uncritically to an HIV population. The challenge to the conclusions that prednisolone had salutary effects in the treatment of tuberculous pericarditis,20 the lack of randomised controlled studies in HIV seropositive individuals, and the suggestion of potentially serious side effects of the use of prednisolone in HIV seropositive patients offered a strong ethical justification for carrying out a placebo controlled trial.
We have shown that high dose prednisolone in addition to antituberculous drugs resulted in reduced mortality and quicker improvement of clinical features, but did not influence the resolution of pericardial effusion. Unlike in Strang and colleague's studies,18 ,19 there were no favourable effects of prednisolone on fever, pulse rate, and sense of wellbeing. However, our subjects were treated largely as outpatients, thus precluding day to day assessment of these features. Compliance was better in the prednisolone arm, probably a reflection of an improved sense of wellbeing in these patients. The findings in this study relate to effusive disease, and so additional studies would be needed to determine the effect of steroids in HIV seropositive individuals with effusive–constrictive and actively constrictive tuberculous pericarditis.
CORTICOSTEROIDS IN HIV RELATED CONDITIONS
Corticosteroids are of benefit in several HIV related conditions, including immune thrombocytopenia28 and lymphoid interstitial pneumonitis,29 and as adjunctive treatment inPneumocystis cariniipneumonia.30 ,31 It has also been postulated that steroid treatment may benefit HIV infection by reducing a putative autoimmune component to CD4 depletion.32 However, there are potentially harmful side effects that may occur from their use in HIV infected individuals. In particular, there is the problem of added corticosteroid related immunosuppression which may lead to a higher incidence of bacterial infections, herpes simplex and herpes zoster reactivation, and potential development of Kaposi's sarcoma.12 ,13 ,33 In a non-randomised study of tuberculosis in HIV seropositive patients, Elliott and colleagues reported that 6/47 (13%) patients on prednisolone compared with 2/118 (2%) non-prednisolone treated patients developed herpes zoster in a two year follow up.12 In the same study three patients who received prednisolone developed Kaposi's sarcoma compared to none who did not. There are, however, other reports of Kaposi's sarcoma actually resolving with steroid treatment.34 In our study Kaposi's sarcoma occurred only in patients who were not on steroids. The assessment of the putative complications of corticosteroid use in HIV seropositive patients will require careful observation of a larger number of patients. Nonetheless, in this study the therapeutic benefits of corticosteroids outweigh their adverse effects.
MORBIDITY AND MORTALITY
Tuberculous pericarditis is a serious condition with a high incidence of constrictive pericarditis and a high mortality rate. Constrictive pericarditis has been described in 11% of patients with effusive tuberculous pericarditis occurring within two years of diagnosis.18 In our series constriction was infrequent and developed in equal numbers of prednisolone and placebo treated patients. Constriction was observed early during the course of treatment, being seen within eight weeks of the start of treatment. It is possible that the rate of constriction is reduced by HIV infection. In general HIV infected individuals in our setting die early, leaving little chance for constriction to develop. High mortality rates of up to 40% have been quoted in tuberculous pericarditis patients even in an HIV seronegative population.35 Mortality from tuberculous pericarditis in HIV infected patients is high because of the occurrence of other HIV related diseases and the increased likelihood of disseminated tuberculosis.6
CONCLUSION
We conclude that HIV seropositive patients with effusive tuberculous pericarditis show a lower mortality rate (both at completion of antituberculous treatment (six months) and at the end of follow up) and a quicker rate of clinical improvement when adjunctive prednisolone is administered in the first six weeks of standard antituberculous treatment. We therefore recommend that in the absence of any specific contraindications, HIV seropositive individuals with effusive tuberculous pericarditis should receive adjunctive prednisolone.
Acknowledgments
We are indebted to CAPS(Pvt) Ltd for providing prednisolone and placebo tablets for the study and for financial support. The University of Zimbabwe research board provided further funding. We would also like to thank the following for various contributions: Dr T Doherty (study planning), Mrs P Manjoro (patient recruitment and follow up), Ms O Lowe (processing of tuberculosis specimens), Dr P Fitzgerald (statistical analysis), Professor PS Douglas (proofreading), and Professor RF Heller (proofreading).