Article Text

Abstract
Objective: To determine if the Niigata-Chuetsu earthquake of October 2004 increased long-term mortality from acute myocardial infarction (AMI).
Design: A comparative study of mortality rates before and after the earthquake, as well as between the disaster and control areas, by analysing death certificate data from 1 October 1999 to 30 September 2007.
Setting: The disaster area and a control area in Niigata Prefecture (n = 2 448 025 in 1 October 2004) in Japan.
Population: The total population of Niigata Prefecture observed for five years (12 333 429 person-years) before and three years (7 279 076 person-years) after the earthquake.
Main outcome measures: Mortality from AMI (ICD-10, I21 and I22).
Results: Overall mortality rates from AMI five years before and three years after the earthquake in the disaster area were 47.3 and 53.9 per 100 000 person-years, respectively. Change (+6.6 or +14.0%) was significantly different (p = 0.0008), compared to the control area, where mortality rates were 42.5 and 42.6 per 100 000 person-years, respectively, and was not significantly different (p = 0.9028). In men, a change in AMI mortality before and after the earthquake in the disaster area was +7.1 per 100 000 person-years (+13.4%, p = 0.0172), and +2.0 (+4.2%, p = 0.2362) in the control area. In women, a change in AMI mortality in the disaster area was +6.2 per 100 000 person-years (+14.9%, p = 0.0184) and −1.6 (−4.2%, p = 0.2735) in the control area.
Conclusions: The Niigata-Chuetsu earthquake significantly increased long-term mortality from AMI in both men and women. Clinicians and policymakers in public health must recognise the need for long-term prevention of AMI in earthquake disaster areas.
Statistics from Altmetric.com
In 2004, an earthquake with M6.8 on the Richter scale hit mid Niigata Prefecture (Chuetsu region) in Japan. This earthquake was one of the strongest ever recorded in Japan with its near-epicentre maximum seismic intensity of 7 on the Japan Meteorological Agency’s Intensity (JMAI) scale, which was comparable to that of the 1995 Great Hanshin-Awaji earthquake in Japan. The Niigata-Chuetsu earthquake caused a great deal of damage; 68 dead, 4795 wounded and 121 495 destroyed homes (3175 completely destroyed).1 Direct and indirect socioeconomic losses from destroyed infrastructure after the Niigata-Chuetsu earthquake was estimated at 3 trillion yen ($30 billion).2
Large earthquakes are recognised as acute stressors.3 A short-term increase in mortality from acute myocardial infarction (AMI), one of the prevalent stress-related diseases, following an earthquake has been reported worldwide.4 5 6 7 8 For example, the Great Hanshin-Awaji earthquake (5480 total deaths) in Japan resulted in an increased mortality from AMI for eight weeks after the earthquake.7 Although human casualties from the Niigata-Chuetsu earthquake were much fewer than those of the Great Hanshin-Awaji earthquake, a short-term increase in cardiovascular events from the Niigata-Chuetsu earthquake has been reported.8
An interesting characteristic of the Niigata-Chuetsu earthquake was that it occurred in a rural, mountainous area, and thereby caused remarkable ground disaster, traffic and communication network disruption and further isolated the mountainous villages.2 These factors delayed reconstruction of community lifelines such that approximately 9000 people lived in temporary housing provided by the local government one year after the earthquake, and 5000 people even two years after the earthquake.9 Although temporary housing ended in December 2007, a number of people continued to struggle to reconstruct their lives owing to financial losses.9
We hypothesised that the residents of Chuetsu experienced stress from living in an unfavourable environment, resulting in high risk of AMI death. To our knowledge, however, very few epidemiological studies have investigated long-term effects of an earthquake on AMI mortality. The aim of this study was to determine if the Niigata-Chuetsu earthquake increased mortality from AMI three years after the earthquake in comparison to the control area.
Methods
The Niigata-Chuetsu earthquake occurred on 23 October 2004, with its epicentre located at 37 degrees latitude, 29 minutes North, and 138 degrees longitude, 87 minutes East.10 The disaster area was the Chuetsu region comprises 12 municipalities, including Nagaoka, Ojiya, Tokamachi, Kashiwazaki, Mitsuke, Uonuma, Minamiuonuma, Kawaguchi, Yuzawa, Tsunan, Izumozaki and Kariwa. A short-term analysis1 of casualties and destroyed houses in the disaster area is shown in table 1. Damage to some municipalities, such as Yuzawa, Tsunan and Izumozaki was light. However, people living in these towns are closely connected socioeconomically to other communities in Chuetsu, and thus we included these three towns as disaster areas. We defined all other municipalities other than the disaster area in Niigata Prefecture as the control area, in order to compare changes in mortality rates before and after the earthquake.
Short-term casualties and destroyed homes in disaster areas (12 municipalities) and control area following the Niigata-Chuetsu earthquake, as officially announced by the Niigata Prefectural government
We examined death certificates for all decedents in the Niigata Prefecture between 1 October 1999 and 30 September 2007 (that is, five years before and three years after the earthquake). In the present study, AMI mortality during the five years before the earthquake was defined as the base mortality. The Japanese government approved this study before we obtained death certificate data. Death certificate data were provided by the Ministry of Health, Labour, and Welfare (No 0819001) and the Ministry of Internal Affairs and Communications (No 272) of Japan with official permission, after each person’s name, address and other identification had been removed. The dataset included the date of death, cause of death, sex and area code. Causes of death from AMI (ICD-10, I21 and I22) were coded using the International Classification of Disease Tenth Revision (ICD-10).
To calculate death rates, we obtained yearly population data from the annual reports of Niigata Prefectural Health and Social Welfare published in 2000–8,11 which is based on the population census of Japan. Since the earthquake occurred in October 2004, we defined the first year after the earthquake as the time period from October 2004 to September 2005. In Japan, the population on the first day of October is published each year. Therefore, the average population of the first year of this study was calculated as an average of the 1 October populations of 2004 and 2005. Yearly populations for other years were calculated in the same manner.
The χ2 test was used to assess differences in mortality rates before and after the earthquake. SAS statistical software (release 9.1.3) was used for all analyses and a p value of less than 0.05 was judged as statistically significant.
Results
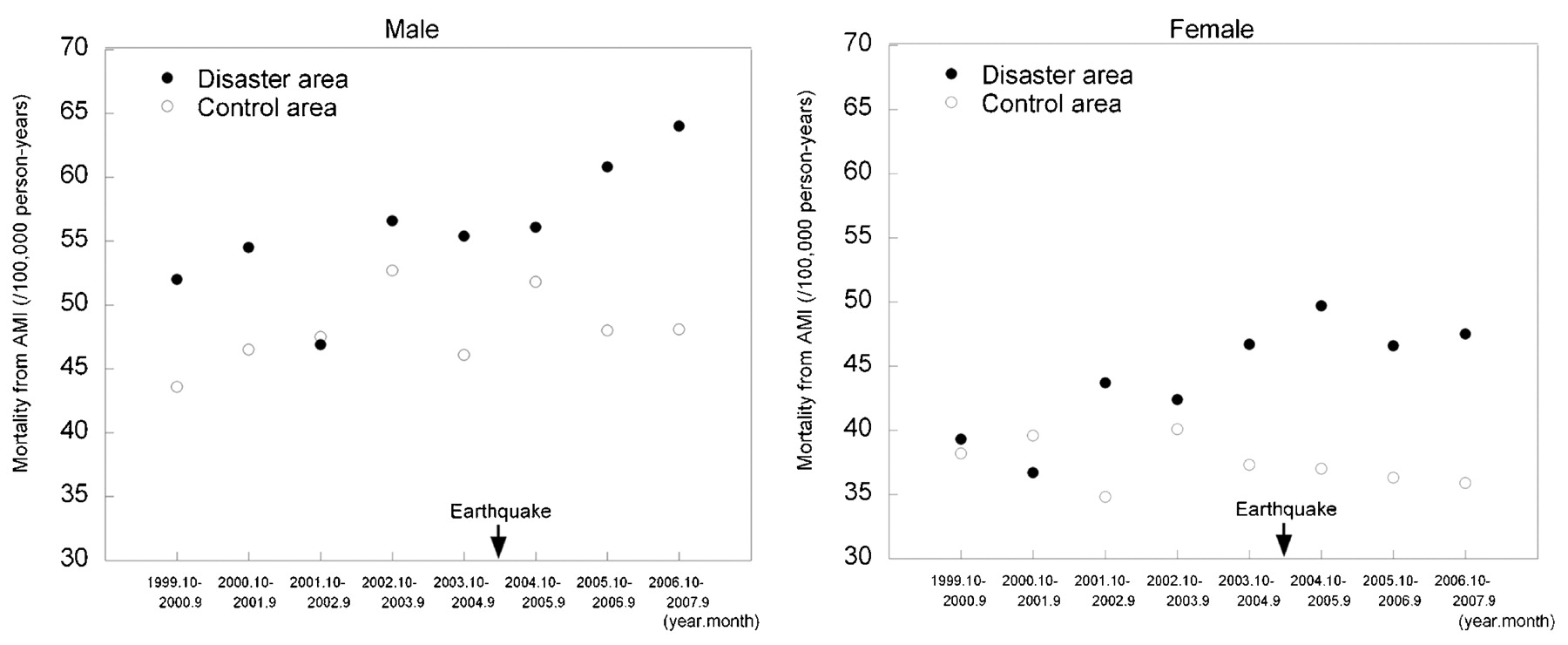
Baseline mortality rates from AMI (five years before the earthquake) in Niigata Prefecture were 48.9 per 100 000 person-years in men, 39.0 in women and 43.8 in total. Overall mortality rates from AMI five years before and three years after the earthquake in the disaster and control areas are shown in table 2. In the disaster area, mortality rate three years after the earthquake increased significantly compared to five years before the earthquake. In the control area, on the other hand, mortality rate after the earthquake did not increase significantly. Similar analyses were conducted by sex, as shown in table 2. In men, mortality rate three years after the earthquake increased significantly in the disaster area, but not in the control area. Secular trends in mortality rates in men in the disaster and control areas are shown in figure 1 (left). Mortality from AMI in the second and third years after the earthquake appears higher than the first year. Similarly, in women, mortality rate three years after the earthquake increased significantly in the disaster area, but not in the control area. Secular trends in mortality rates in women in the disaster and control areas are shown in figure 1 (right). Mortality from AMI during the first year after the earthquake appears higher than that of the second and third years.
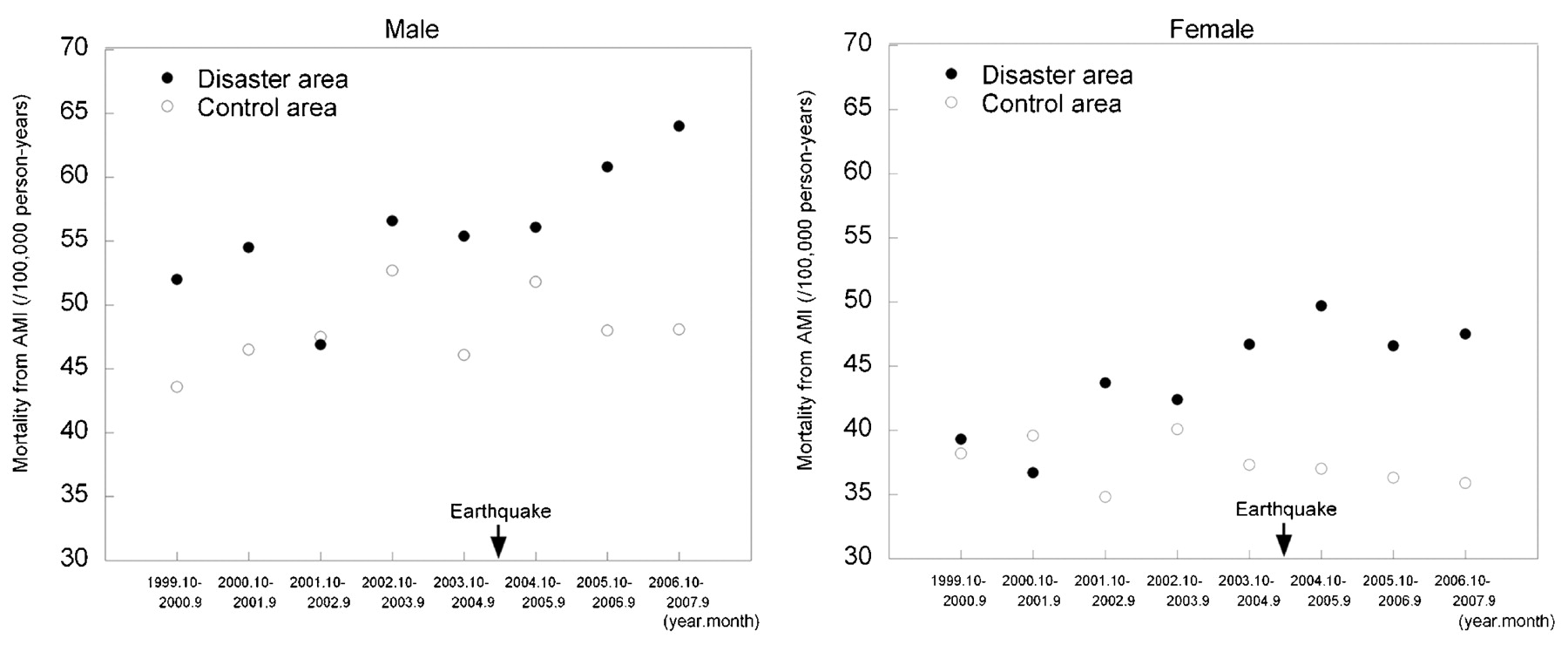
Secular trends in mortality rates from acute myocardial infarction (AMI) in the disaster and control areas by sex.
Comparison of overall mortality from acute myocardial infarction (AMI) between five years before and three years after the Niigata-Chuetsu earthquake (23 October 2004)
Overall mortality rates from AMI five years before and one year after the earthquake in the disaster area were 47.3 and 52.8 per 100 000 person-years, respectively. This change in mortality rates (+5.5) was of borderline significance (χ2 = 3.53, p = 0.0603), while change in the control area from 42.5 to 44.2 was not significantly different (χ2 = 0.96, p = 0.3275).
Change in population between the disaster and control areas after the earthquake must be compared. In the disaster area three years after the earthquake, there was a −1.4% population change ((668 620–659 103)/668 620) compared to a −0.9% change in the control area ((1 771 123–1 754 557)/1 771 123), which reflects a significant difference (p = 0.0153). Changes in the proportion of the population aged 65 years and older in the disaster and control areas are shown in figure 2. After the earthquake, the rate of ageing was similar in the two areas.

{kind=link}
{kind=link}
Trends in the proportion of people aged 65 years or over in the disaster and control areas.
Discussion
The present study shows that the Niigata-Chuetsu earthquake significantly increased long-term mortality from AMI by 14% three years after the earthquake in both men and women. Short-term effects of an earthquake on AMI are considered to result from an acute stressor.3 However, long-term effects of an earthquake probably follow a different pathogenesis as a chronic stressor (we will refer to chronic stress as “stress”).
Several epidemiological studies have shown that psychological consequences of an earthquake may last as long as seven years.12 13 14 These studies assessed psychological stress, distress and psychiatric disorders, including post-traumatic stress disorders, depression, anxiety and sleep disorders. Considering these facts, the damage from an earthquake appears to cause long-term stress on the lives of people living in disaster areas. We believe that financial loss and social network disruptions are important determinants of psychological stress among the residents of Chuetsu, given the geographical characteristics of this area.
Other studies
Although numerous studies have examined short-term effects of an earthquake on AMI, few have done so for mid-term or long-term effects. Armenian et al15 reported that the number of deaths from heart disease increased within the first six months following an earthquake in Armenia. The present study is the first study demonstrating an increase in long-tem mortality from AMI in a disaster area.
Considerable evidence suggests that stress, such as perceived mental stress, is associated with coronary heart disease.16 Although perceived mental stress is subjective and differs across various ethnic groups, recent studies have shown a positive association between psychological stress and AMI mortality across ethnic groups, including Japanese.17 18 Iso et al studied a Japanese population and showed that, in women, those who perceived high mental stress had a 2.7-fold higher risk of myocardial infarction mortality and a 1.6-fold higher risk in men (statistically insignificant).17 Rosengren et al conducted a large, multi-ethnic case-control study and demonstrated that those with chronic stress have significantly higher risk of AMI, with an odds ratio (OR) of 2.2 and a population attributable risk (PAR) of 12%. They also reported a significantly higher risk in groups with severe financial stress (OR = 1.3, PAR = 11%), more than one stressful life event (OR = 1.5, PAR = 10%) and feelings of depression (OR = 1.6, PAR = 9%). These findings are consistent with the results of our study.18
Strengths and weaknesses of the study
We were able to conduct a comparative study by selecting an appropriate control area for the disaster area of focus. In addition, changes in the population were relatively small because Niigata Prefecture is surrounded by high mountains. The average population change within the disaster area was 3.2% in 2004, 3.1% in 2005, 2.9% in 2006 and 2.8% in 2007, compared to 3.2%, 2.9%, 2.7% and 2.9%, respectively, in the control area.11
The present study also has some important limitations. We did not assess a dose-response relation between earthquake-induced damage/loss and AMI mortality for two reasons. First, the most damaged areas near the epicentre were sparsely populated. In addition, physical damage and financial losses differed among subregions within a municipality. We were not able to obtain detailed data on both damage/loss and the number of AMI deaths in such subregions. Finally, an association between the earthquake and AMI mortality may possibly be due to chance alone. The descriptive nature of this study did not allow us to determine an adjusted association for established risk factors of AMI. Such an association should be reconfirmed by investigating other earthquakes.
Mechanism
The long-term mechanism of earthquake-related stress on AMI is unclear, although stress plays an important part. A longitudinal study of a 1980 earthquake in Italy showed that psychosocial consequences were unrelated to changes in risk factor profiles of coronary heart disease.19 20 This suggests that earthquake-related stress is associated with cardiac events through a separate mechanism. Unfortunately, we did not assess a dose-response relation between earthquake-related stress and AMI mortality, and thus this should be clarified in future studies.
Implications for clinicians and policymakers
This study suggests that prolonged stress following an earthquake increases the long-term mortality from AMI. The excess mortality from AMI after the earthquake was estimated to be 6.5 per 100 000 person-years (6.6 in the disaster area minus 0.1 in the control area). It should be noted that Japan has the lowest AMI mortality rate in the world, and the age-adjusted mortality rate from ischaemic heart disease has been reported to be one-third that of the UK.21 Therefore, an earthquake in areas with higher risk of AMI would experience more deaths from AMI compared to the Niigata-Chuetsu earthquake. Clinicians and policymakers in public health must be made aware of the need for long-term prevention of AMI after an earthquake, especially in countries with a high risk of AMI.
Unanswered questions and future research
The present study demonstrated an elevated AMI mortality in the disaster area three years after the earthquake. The duration of the increased mortality from AMI must be further analysed. In addition, an analytical epidemiological study on the association between stress after an earthquake and AMI mortality should be conducted in the near future as a follow-up to the present descriptive study.
What is already known on this subject
Increased short-term mortality from acute myocardial infarction (AMI) following an earthquake has been reported worldwide. However, the long-term effects of an earthquake on AMI mortality are not clear.
What this study adds
The Niigata-Chuetsu earthquake increased the long-term mortality from AMI in both men and women. Clinicians and policymakers should be aware of the need for providing long-term prevention of AMI among those living in earthquake disaster areas.
Acknowledgments
All authors designed the study and approved the final version of the manuscript. IN, KN and MY designed the study, and IN and KN drafted the manuscript. OY and KI were responsible for the population data of Niigata Prefecture. IN and MO were responsible for the death certificate data. KN and YT were responsible for statistical analyses. KN is the guarantor.
REFERENCES
Footnotes
See Editorial, p 1972
Competing interests None declared.
Provenance and Peer review Not commissioned; externally peer reviewed.