Article Text

Abstract
β-Blockers (BBs) are an essential class of cardiovascular medications for reducing morbidity and mortality in patients with heart failure (HF). However, a large body of data indicates that BBs should not be used as first-line therapy for hypertension (HTN). Additionally, new data have questioned the role of BBs in the treatment of stable coronary heart disease (CHD). However, these trials mainly tested the non-vasodilating β1 selective BBs (atenolol and metoprolol) which are still the most commonly prescribed BBs in the USA. Newer generation BBs, such as the vasodilating BBs carvedilol and nebivolol, have been shown not only to be better tolerated than non-vasodilating BBs, but also these agents do not increase the risk of diabetes mellitus (DM), atherogenic dyslipidaemia or weight gain. Moreover, carvedilol has the most evidence for reducing morbidity and mortality in patients with HF and those who have experienced an acute myocardial infarction (AMI). This review discusses the cornerstone clinical trials that have tested BBs in the settings of HTN, HF and AMI. Large randomised trials in the settings of HTN, DM and stable CHD are still needed to establish the role of BBs in these diseases, as well as to determine whether vasodilating BBs are exempt from the disadvantages of non-vasodilating BBs.
- beta-blockers
- HEART FAILURE
- carvedilol
- myocardial infarction
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Hypertension and diabetes
Hypertension (HTN) is a largely asymptomatic disease affecting around 50 million Americans and one billion people worldwide.1–3 Patients with HTN are at an increased risk for heart failure (HF), stroke, renal disease and acute myocardial infarction (AMI).1 ,3 Although HTN is the most common primary care diagnosis in the USA, it remains undertreated.3
Pharmacological treatment of HTN includes the class of medications known as β-blockers (BBs). The various agents in this class differ substantially in their pharmacological properties. Atenolol, metoprolol, bisoprolol and nebivolol are β1 selective BBs, preferentially inhibiting cardiac β1 receptors as opposed to β2 receptors. Carvedilol, in contrast, inhibits β1, β2 (postsynaptic and presynaptic) and α1 receptors, upregulates cardiac muscarinic M2 receptors and possesses antioxidant effects.4–7 Additionally, nebivolol (which is highly selective for the β1 receptor) also has vasodilating properties due to its ability to increase the endogenous production and release of endothelial nitric oxide (NO).3 ,8
Atenolol
The Medical Research Council (MRC) elderly HTN treatment trial was a placebo-controlled, single-blind trial that randomised 4396 patients between the age of 65–74 years to receive either hydrochlorothiazide (HCTZ; plus amiloride), atenolol or placebo.9 Despite the fact that atenolol reduced blood pressure (BP) to levels below that of placebo (approximately −10/7 mm Hg over 60 months), patients receiving atenolol, compared with patients assigned to placebo, did not have a significant reduction in any cardiovascular (CV) end point during 5.8 years of the study (stroke (relative risk (RR) 0.82, 95% CI 0.60 to 1.14, p=0.25); coronary heart disease (CHD; RR=0.97, 95% CI 0.73 to 1.30, p=0.85); CV events (RR=0.96, 95% CI 0.77 to 1.19, p=0.69); CV death (RR=1.06, 95% CI 0.81 to 1.39, p=0.66) and total death (RR=1.08, 95% CI 0.88 to 1.34, p=0.46)). On the other hand, patients receiving HCTZ plus amiloride had a significantly reduced risk of stroke (31%, 95% CI 3% to 51%, p=0.04); CHD events (44%, 95% CI 21% to 60%, p=0.0009) and all CV events (35%, 95% CI 17% to 49%, p=0.0005). Even after adjusting for lower than atenolol-induced BP changes, HCTZ plus amiloride still led to a lower risk of CV events (p=0.01) than atenolol. Despite this fact, both the HCTZ plus amiloride and the atenolol groups compared with placebo had significantly increased withdrawals per 1000 patient years due to impaired glucose tolerance 6.9 (HCTZ) versus 2.7 (placebo) per 1000 patient years and 5.8 (atenolol) versus 2.7 (placebo) per 1000 patient years.
In summary, atenolol provided no CV or all-cause mortality reduction in elderly hypertensive patients over a period of 5.8 years but increased glucose intolerance.8 A limitation in the interpretation of these results is the fact that after 5.8 years only 52% of patients remained on HCTZ plus amiloride and only 37% of patients remained on atenolol.
The Heart Attack Primary Prevention in Hypertension (HAPPHY) study trial randomised 6569 men aged 40–64 years with mild-to-moderate HTN to a thiazide diuretic (bendrofluazide or HCTZ) or a BB (atenolol or metoprolol) to determine if BBs differed from thiazides in the prevention of CHD events and death.10 Although both groups had a similar BP lowering effect (140/89 mm Hg in the BB group and 140/88 mm Hg in the thiazide group, p value not significant), when compared with each other, the BB group did not show any difference in fatal/non-fatal CHD per 1000 patient years (10.62 vs 9.48/years, respectively; OR=0.88, 95% CI 0.68 to 1.14), fatal/non-fatal stroke (2.58 vs 3.35/years, respectively; OR=1.29, 95% CI 0.82 to 2.04) or all deaths (7.73/years vs 8.25/years, respectively; OR=1.06, 95% CI 0.80 to 1.41). This was unexpected since HCTZ monotherapy (without amiloride, etc) has never been shown to reduce CV events compared with placebo or controls.11–13 Therefore, the first generation BBs (atenolol and metoprolol) in this study offer no additional benefit when compared with a thiazide diuretic (HCTZ), which suggests that atenolol or metoprolol may not be superior to placebo for improving CV prognosis in HTN.
Left ventricular hypertrophy (LVH), which typically develops as a consequence of poorly controlled HTN as well as obesity and ageing, carries a higher CV morbidity and mortality rate; it remains uncertain whether or not BBs reduce the risk of CV events in this patient population. In the Losartan Intervention For Endpoint Reduction (LIFE) trial, atenolol was compared with losartan in patients with HTN with evidence of LVH on ECG.14 Losartan was statistically superior to atenolol for reducing the primary composite end point of CV death and stroke (11% vs 13%, adjusted HR=0.87, 95% CI 0.77 to 0.98, p=0.021). Similarly, the incidence of stroke (5% vs 7%, HR=0.75, 95% CI 0.63 to 0.89, p=0.001) as well as new-onset diabetes mellitus (DM; 6% vs 8%, HR=0.75, 95% CI 0.63 to 0.88, p=0.001) was significantly lower in the losartan group. However, CV mortality (4% vs 5%, HR=0.89, 95% CI 0.73 to 1.07, p=0.206), MI (4% vs 4%, HR=1.07, 95% CI 0.88 to 1.31, p=0.491) and total mortality (8% vs 9%, HR=0.90, 95% CI 0.78 to 1.03, p=0.128) were not statistically different between the two groups. The incidence of adverse effects was lower in the losartan group as compared with the atenolol group. These adverse events included bradycardia (1% vs 9%, p<0.0001), cold extremities (4% vs 6%, p<0.0001), hypotension (3% vs 2%, p=0.001), sexual dysfunction (4% vs 5%, p=0.009), albuminuria (5% vs 6%, p=0.0002), hyperglycaemia (5% vs 7%, p=0.007), asthenia/fatigue (15% vs 17%, p=0.001), back pain (12% vs 10%, p=0.004), dyspnoea (10% vs 14%, p<0.0001), lower extremity oedema (12% vs 14%, p=0.002) and pneumonia (5% vs 6%, p=0.018).14
The rebound peripheral vasoconstriction that occurs from decreased cardiac output (CO) and unopposed α stimulation due to β1 selective BB therapy results in decreased skeletal muscle perfusion causing adverse effects on lipid and glucose metabolism by increasing insulin resistance. Significant increases in glucose concentrations have been seen with atenolol, metoprolol and propranolol.15–18 As discussed previously, the LIFE study showed a 25% (HR=0.75, 95% CI 0.63 to 0.88, p=0.001) lower risk of new-onset DM in the losartan-treated group compared with the atenolol group.19 In the Atherosclerosis Risk in Communities (ARIC) cohort study of 3804 patients with HTN, the BB group had a 28% higher risk of type 2 DM (T2DM) compared with the control group (RR=1.28, 95% CI 1.04 to 1.57).14 The Captopril Prevention Project (CAPP) trial investigated in 10 985 patients with HTN the effect of captopril (50–100 mg/day) versus a conventional anti-HTN treatment regimen that included a diuretic, a BB or both.20 The patients in the conventional treatment group most frequently received atenolol (50–100 mg/day) or metoprolol (50–100 mg/day) and/or HCTZ (25 mg/day) or bendrofluazide (2.5 mg/day); CV mortality (0.77, p=0.092) and the incidence of T2DM (RR=0.79; p=0.007) were found to be lower in the captopril than in the conventional therapy group. Conversely, fatal and non-fatal strokes showed a higher incidence with captopril treatment (1.25, p=0.044), whereas fatal and non-fatal MI had similar incidences (0.96, p=0.68).
In the International Verapamil-Trandolapril Study (INVEST) trial, approximately 23 000 patients with HTN and CHD were randomised to verapamil or atenolol. Verapamil-treated patients had a significantly lower incidence of new-onset DM versus atenolol (15% lower risk; RR=0.85, 95% CI 0.77 to 0.95).21 In the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA) trial, atenolol given for 5.5 years increased CV mortality (p=0.001), all-cause mortality (p=0.025), and the development of DM (p<0.0001) compared with amlodipine.22 In a post hoc analysis of the ASCOT-BPLA study, use of atenolol was a significant predictor for the development of DM.23 In a 5-year study of 228 patients comparing treatment with doxazosin to atenolol, atenolol caused a significant reduction in high-density lipoprotein cholesterol from baseline (p<0.05), as well as a significant increase in triglycerides from baseline (p<0.0001); both of these changes suggest that atenolol triggered an increase in insulin resistance. Several other studies have confirmed the negative effects of atenolol on lipids in patients with HTN.24 Thus, it is clear that β1 selective BBs (atenolol and metoprolol) can worsen the metabolic syndrome (increased insulin resistance, worsened atherogenic dyslipidaemia and increased weight gain).
Metoprolol
The Metoprolol Atherosclerosis Prevention in Hypertensives (MAPHY) trial was a post hoc analysis of the metoprolol arm of the HAPPHY study.25 It focused on male patients between 40 and 64 years of age who had a history of HTN with an untreated diastolic BP of over 100 mm Hg and investigated the effects of metoprolol on the incidence of CHD events (sudden cardiac death (SCD) and MI) compared with thiazide diuretics. Patients receiving metoprolol were significantly less likely to experience a CHD event as compared with those on diuretics (111 vs 144 cases, p=0.001, corresponding to 14.3 vs 18.8 cases/1000 patient years; RR=0.76 at the end of the trial; 95% CI 0.58 to 0.98). Moreover, the incidence of SCD, fatal and non-fatal MI was reduced with metoprolol as compared with the diuretic treatment (p=0.024). Similarly, the risk of silent MI (p=0.016) and first definite non-fatal MI (p=0.0034, 10.6 vs 14.3 cases/1000 patient years at the end of the trial) were also lower with metoprolol. It is important to note that all baseline characteristics, including BP, were similar in the 255 participants who had a CV event versus those who did not. This suggests that the benefit demonstrated by metoprolol occurred due to something other than an anti-HTN effect. Despite these beneficial results, MAPHY should be interpreted with caution because of its post hoc subgroup design.
Metoprolol has been shown to have less favourable effects on glycaemic control when compared with carvedilol. The Glycemic Effects in Diabetes Mellitus: Carvedilol-Metoprolol Comparison in Hypertensives (GEMINI) trial showed that compared with metoprolol, carvedilol significantly reduced new-onset DM (10.3% vs 12.6%, p=0.048), and significantly improved insulin sensitivity (p<0.004 vs p=0.48).4 Additionally, carvedilol decreased triglycerides significantly more than metoprolol (−2.9%; p=0.001 for the between-group difference) and caused significantly less weight gain (0.17 vs 1.2 kg, respectively; p<0001).4 In addition, microalbuminuria, a surrogate marker for endothelial function, occurred less often in the carvedilol group (6.4% vs 10.3%; p=0.04).4 Pharmacological comparisons between carvedilol versus atenolol and metoprolol are listed in table 1.
Atenolol and metoprolol versus carvedilol
Meta-analyses
Almost two decades ago, conflicting meta-analyses came out, just a year apart from each other. While the first suggested BB therapy was appropriate as a first-line antihypertensive agent, another meta-analysis published a year later indicated that BBs are indeed inappropriate first-line antihypertensives in uncomplicated HTN in elderly patients.26 ,27 A recent meta-analysis of 13 randomised controlled trials (RCTs) encompassing 105 951 patients with primary HTN indicated that the RR of stroke was higher for BBs than other anti-HTN medications (RR=16%; 95% CI 4% to 30%);28 in these meta-analyses, atenolol was the most frequently utilised BB for first-line treatment of HTN. The meta-analysis concluded that BBs (mainly atenolol) increased the risk of stroke and were less effective than other antihypertensives as first-line therapy.
Another meta-analysis evaluated the effects of atenolol on morbidity and mortality in patients with HTN29 and demonstrated that although there was a significant difference in the BP lowering effect of atenolol and placebo, this anti-HTN effect of atenolol failed to translate into a significant reduction in the all-cause mortality (RR=1.01, 95% CI 0.89 to 1.15). Similarly, CV mortality (RR=0.99, 95% CI 0.83 to 1.18) and MI (RR=0.99, 95% CI 0.83 to 1.19) were not significantly different between the placebo and the atenolol groups. However, the risk of stroke was decreased, but not significantly, in the atenolol group as compared with placebo (RR=0.85, 95% CI 0.72 to 1.01). When compared with other anti-HTN agents, there was no significant difference in the anti-HTN effect; there was, however, a significantly higher mortality in the atenolol group (RR=1.13, 95% CI 1.02 to 1.25). Moreover, there was a higher risk of CV mortality (RR=1.16, 95% CI 1.00 to 1.34) and stroke (RR=1.30, 95% CI 1.12 to 1.50) with atenolol as compared with the other antihypertensives. Thus, this meta-analysis illustrated that although atenolol produces a marginal benefit as compared with placebo with regard to stroke prevention, it does not hold any benefit over other antihypertensives. The authors concluded that the results of this meta-analysis question whether atenolol should be used as a first-line anti-HTN agent.
A Cochrane review was conducted on the effectiveness and safety of BBs on the rates of morbidity and mortality in patients with HTN.30 This meta-analysis failed to show any significant benefit of BBs on the total mortality rates when compared with placebo (RR=0.99, 95% CI 0.88 to 1.11), diuretics (RR=1.04, 95% CI 0.91 to 1.19) or renin-angiotensin aldosterone system (RAAS) inhibitors (RR=1.10, 95% CI 0.98 to 1.24). Conversely, total mortality was higher when BBs were compared with calcium-channel blockers (CCBs; RR 1.07, 95% CI 1.00 to 1.14). There was a statistically significant decrease in the risk of total CV disease (RR=0.88, 95% CI 0.79 to 0.97) and stroke (RR=0.80, 95% CI 0.66–0.96) when BBs were compared with placebo. However, there was no difference in the risk of CHD between BBs and placebo (RR=0.93, 95% CI 0.81 to 1.07) or total CV disease between BBs and diuretics or RAAS inhibitors. There was a higher risk of total CV disease (RR=1.18, 95% CI 1.08 to 1.29) and stroke (RR=1.24, 95% CI 1.11 to 1.40) when BBs were compared with CCBs. The risk of stroke was also higher with BB as compared with RAAS inhibitors (RR=1.30, 95% CI 1.11 to 1.53). Additionally, patients on BBs had a higher rate of discontinuation when compared with RAAS inhibitors (RR=1.41, 95% CI 1.29 to 1.54), but such a difference was not seen with the other drugs. This analysis shows that the benefit of BB therapy is only moderately superior to placebo and is significantly inferior to other anti-HTN drugs. However, these results with the older BB agents cannot be generalised to the newer vasodilating BBs (carvedilol and nebivolol).
The risk of development of new-onset DM with BBs was assessed in a systematic review.31 This review included 12 studies with a total of 94 492 participants and found that there was a 22% increase in the risk of development of new-onset DM with BB therapy as compared with non-diuretic anti-HTN therapy (RR=1.22, 95% CI 1.12 to 1.33). There was also an increased risk of DM with BB therapy as compared with placebo (fixed-effects model: 33% increase, RR=1.33, 95% CI 1.00 to 1.76, p=0.05; random-effects model: 44% increase, RR=1.44, 95% CI 0.69 to 3.00, p=0.33; heterogeneity χ2 6.18, p=0.013). The risk of DM was, however, less with BB therapy than with thiazide diuretics (fixed effect model: 26% decrease, RR=0.74, 95% CI 0.61 to 0.90, p=0.002; random effect model: 21% decrease, RR=0.79, 95% CI 0.45 to 1.41, p=0.43; heterogeneity χ2=23.18, p<0.0001). Among BBs, the risk of DM was greatest with atenolol treatment and the risk of new-onset DM increased with the duration of the treatment. BB therapy increased the risk of death by 4% (pooled RR=1.04, 95% CI 1.00 to 1.09, p=0.056; heterogeneity χ2 10.63, p=0.560) and the risk of stroke by 15% (pooled RR=1.15, 95% CI 1.01 to 1.30, p=0.029; heterogeneity χ2 27.8, p=0.001) compared with other anti-HTN agents. There was no effect on MI (pooled RR=1.02, 95% CI 0.92 to 1.12, p=0.769; heterogeneity χ2 19.30, p=0.023). The risk of DM, death and stroke is, therefore, increased by BB therapy as compared with other non-diuretic anti-HTN drugs and this effect was more pronounced with atenolol therapy.
In another meta-analysis, the role of BBs for the prevention of developing HF in patients with HTN was evaluated.32 This review included 12 RCTs with 112 177 patients with HTN and showed that the BP was reduced by 12.6/6.1 mm Hg by BB therapy as compared with placebo (systolic BP weighted mean reduction 12.6±7.8 mm Hg; diastolic BP weighted mean reduction 6.1±4.4 mm Hg). As compared with other anti-HTN agents, the BP lowering efficacy was similar across all groups (vs diuretics 0.0/−1.0 mm Hg; vs RAAS inhibitors−0.3/−0.6 mm Hg; vs CCBs −0.1/+0.7 mm Hg) and the decrease in the HF risk was also similar (RR=1.00, 95% CI 0.92 to 1.08). When compared with placebo, BBs showed a 23% decrease in the risk of HF (p=0.055). However, comparison between BBs and other anti-HTN agents showed no statistically significant difference (BB vs others, 2.1% vs 2.1%, p=0.91). In trials comparing atenolol with other anti-HTN agents, atenolol had a similar effect in preventing HF (1.8% vs 1.7%; p=0.72) and the risk of stroke was increased by 19% in the BB group. In addition, there was no additional anti-HTN benefit of BB therapy when compared with other anti-HTN drugs. Moreover, there was a higher incidence of stroke in this elderly population. Therefore, this evidence confirms that first generation BBs should not be prescribed as first-line anti-HTN agents, especially in the elderly.
Heart failure
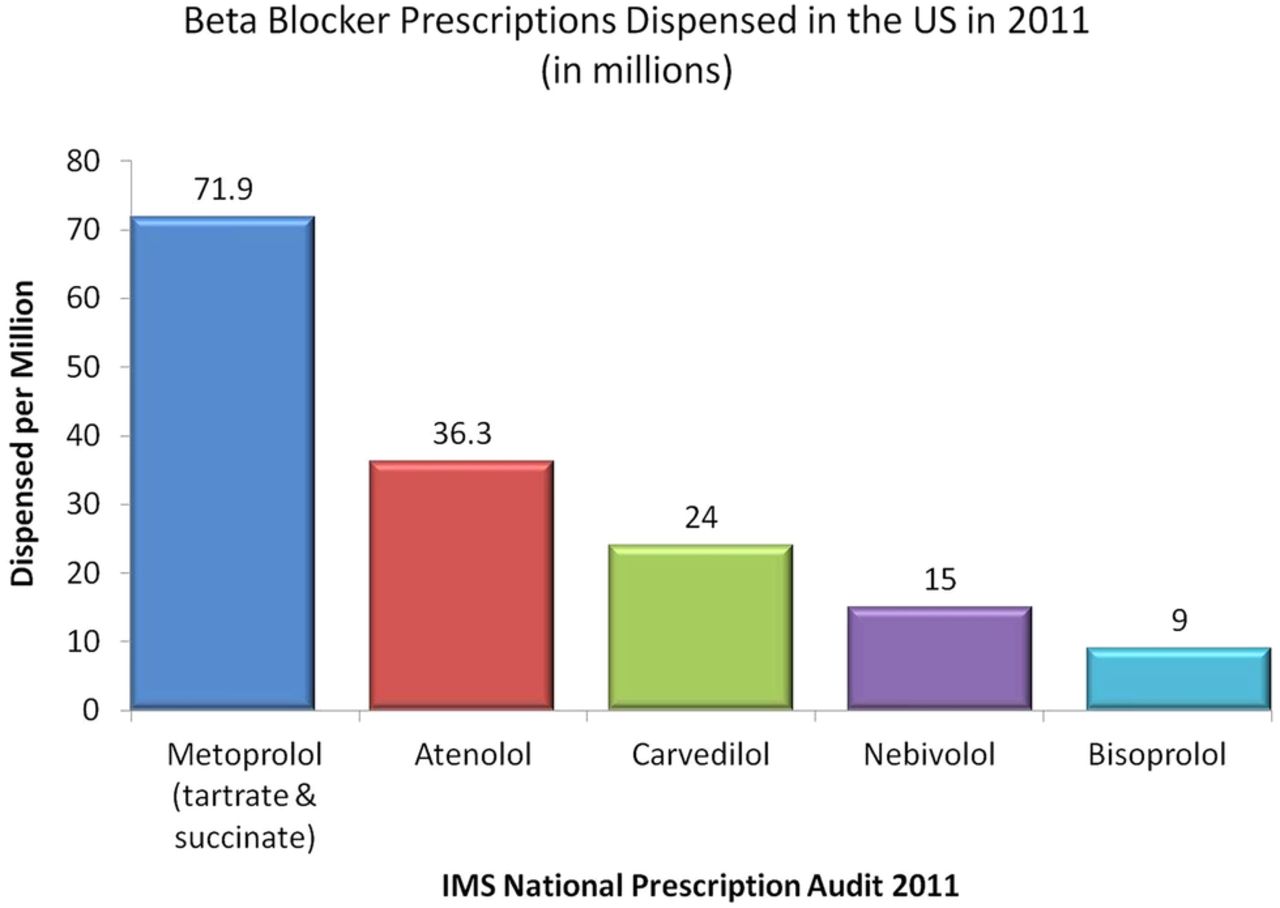
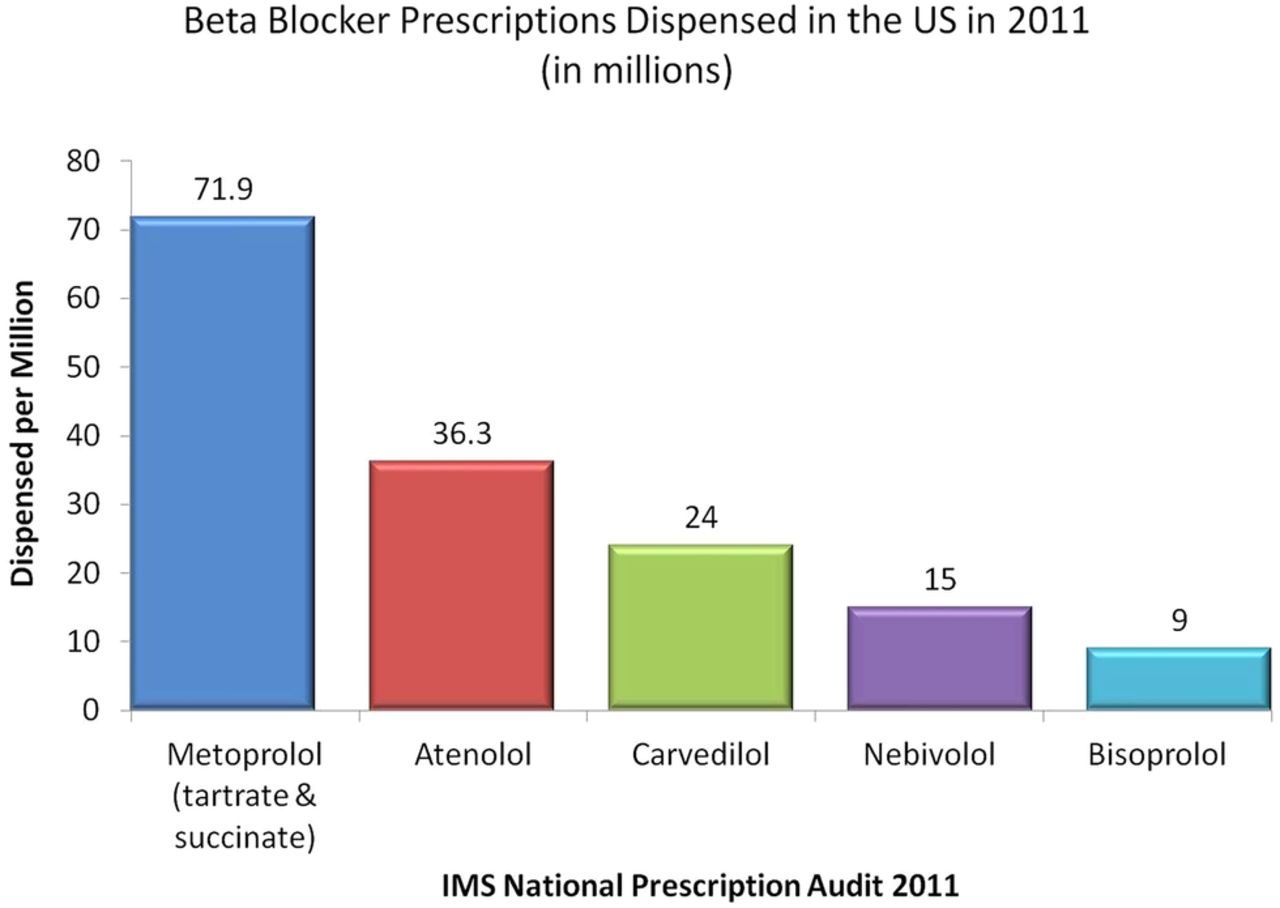
An estimated 5 million people in the USA have HF and more than 550 000 people are diagnosed with this condition each year.33 ,34 During the past two decades, based on impressive RCT data, BBs have become one of the most important pharmacological treatments for improving the CV prognosis for patients with systolic HF. It has been shown that the most frequently prescribed BBs in patients with HF in the USA and in Europe are metoprolol and atenolol.35 ,36 Among 11 326 adults who survived a hospitalisation for HF, pharmacy records revealed that the most commonly prescribed BBs in descending order were metoprolol tartrate (43.2%), atenolol (38.5%), carvedilol (11.6%) and other BBs (6.7%).36 A recent national prescription audit of BBs dispensed in the USA in 2011 indicated that the most commonly prescribed BBs in descending order are metoprolol tartrate/succinate (71.9 million), atenolol (36.3 million), carvedilol (24 million), nebivolol (15 million) and bisoprolol (9 million; figure 1). Disturbingly, these BB choices in the patients with HF are not evidence-based.
{kind=link}
β-Blocker prescriptions dispensed in the USA in 2011 (in millions).
Atenolol
Clinical trials testing atenolol on outcomes in patients with HF are lacking. Atenolol (mean dose 50 mg daily) was compared with metoprolol tartrate (mean dose 65.5 mg daily) in a RCT in 150 patients with mild-to-moderate HF (aged 70 or less) with New York Heart Association (NYHA) functional class II and III, and a left ventricular ejection fraction (LVEF) ≤40%.35 ,36 During a follow-up of 12 months, atenolol significantly reduced the combined end point (all-cause death plus CV hospitalisation) versus control (p=0.0001); however, significantly more patients had a combined end point on control (n=19) and on atenolol (n=8) versus metoprolol (n=4; p=0.0428 for the difference between atenolol, p=0.0002 for the difference between control). Moreover, the hospitalisation rate was significantly reduced with metoprolol (4%) versus atenolol (12%) and placebo (26.3%). Additionally, the combined end point (all-cause mortality and CV hospitalisation) was significantly reduced with metoprolol (RR reduction (RRR) 77%) versus atenolol (RRR=53%). This trial indicated that both atenolol and metoprolol are beneficial in patients with HF but that metoprolol is more effective than atenolol.
In another study, 100 patients with class II or III HF (LVEF ≤25%) already receiving high-dose enalapril (40 mg daily) were randomised to atenolol (maintenance dose 89 mg/day) or placebo for 395 days.39 The primary combined end point (worsening HF or death) was significantly reduced with atenolol versus placebo (p<0.01). Despite this fact, there was no significant reduction in death or worsening HF with atenolol versus placebo when these end points were individually assessed (death: 5 vs 8, worsening HF: 8 vs 19, respectively). However, hospitalisations for CV events (6 vs 21, p=0.07), hospitalisations for worsening HF (5 vs 12, p=0.05) and hospitalisations for arrhythmias (1 vs 9, p<0.01) were all reduced with atenolol.
Metoprolol
Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF) was a double-blind, randomised, placebo-controlled study testing metoprolol CR/XL (target dose was 200 mg once daily) in 3991 patients with chronic HF (NYHA functional class II–IV and LVEF of 40% or less).40 Metoprolol significantly reduced all-cause mortality by 34% (RR=0.66, 95% CI 0.53 to 0.81, p=0.00009). However, there was an increase in mortality with metoprolol versus placebo in the US geographical region (HR=1.05, 95% CI 0.71 to 1.56), which included almost one-third of the mortality events in MERIT-HF. An increase in mortality with metoprolol versus placebo is also supported by the Metoprolol in Dilated Cardiomyopathy (MDC) trial, which showed an 18% increased risk of death, although not statistically significant, with metoprolol versus placebo in patients with dilated cardiomyopathy (RR=1.18, 95% CI 0.66 to 2.09, p=0.57).41 Thus, while geographical disparity must be interpreted with caution, there does not seem to be evidence in the USA (US patients and how clinicians treat them in the USA may differ from that outside the USA) supporting the use of metoprolol in patients with HF.
Bisoprolol
The Cardiac Insufficiency Bisoprolol Study (CIBIS)-I trial was conducted in 641 patients with a history of HF and a LVEF of <40%.42 These patients were randomised to receive either bisoprolol or placebo in addition to diuretic and vasodilator therapy. There was no significant difference between the groups’ mortality (RR=0.80, 95% CI 0.56 to 1.15, p=0.22), SCD or death due to ventricular tachycardia (VT) or ventricular fibrillation (VF). Conversely, the rate of hospitalisation for CV decompensation was lower in the group receiving bisoprolol (p<0.01). Non-lethal events, such as acute pulmonary oedema, HF without pulmonary oedema and cardiogenic shock, that is, pump failure, were less commonly seen in the bisoprolol group (p<0.001). Documented cases of VT and VF were also fewer (p=0.03) in the bisoprolol group and treatment withdrawals were similar across both groups. This study supports the beneficial effects of bisoprolol in patients with a history of HF.
The CIBIS-II trial was conducted to assess the effect of BBs on the survival of patients with HF.43 This study randomised 2647 patients with CHF NYHA class III or IV and LVEF of less than 35% to receive either bisoprolol or placebo in addition to diuretics and ACE inhibitors. This study was stopped early because bisoprolol showed a significant reduction in the incidence of all-cause mortality. As compared with the placebo group, the group receiving bisoprolol had significantly lower mortality rates (11.8% vs 17.3%, HR=0.66, 95% CI 0.54 to 0.81, p<0.0001) and the incidence of SCD was also lower in the bisoprolol group (3.6% vs 6.3%, HR=0.56, 95% CI 0.39 to 0.80, p=0.0011). Similarly, CV deaths (p=0.0049), hospitalisations for any cause (p=0.0006) and the combined end point of CV death and hospitalisation for CV event (p=0.0004) were also seen more infrequently in the group treated with bisoprolol. Hospitalisations due to VT and fibrillation (p=0.006), and hypotension (p=0.03) were also less common in the bisoprolol group, whereas hospitalisations due to bradycardia (p<0.004) and stroke (p=0.04) were more common with bisoprolol.
Carvedilol
Several major trials have established the CV benefits of carvedilol over traditional non-vasodilating BBs in patients with HF. A meta-analysis of 19 placebo-controlled RCTs tested the efficacy of carvedilol versus metoprolol in terms of LVEF in patients with chronic HF. Carvedilol significantly increased LVEF when compared with metoprolol (placebo-corrected increases of +0.065 vs +0.038, p=0.0002) as well as in the four active-controlled trials which directly compared carvedilol versus metoprolol (+0.084 vs +0.057, p=0.009), and these benefits were derived in both patients with and without CHD.44
A randomised trial of 51 patients with HF with a mean LVEF of 37% and chronic obstructive pulmonary disease were treated with carvedilol, bisoprolol and metoprolol, and subsequently returned to their original BB treatment. N-terminal prohormone brain natriuretic peptide (NT-proBNP) levels, which are elevated in HF and have been shown to be a better predictor of major CV events than C reactive protein, were measured.45 Carvedilol reduced NT-proBNP levels significantly better than did either metoprolol or bisoprolol (mean NT-proBNP level were: 1001, 1371, 1349 ng/L, respectively (p<0.01).46
An investigation of 136 patients with HF on cardiac resynchronisation therapy showed that on carvedilol there was a 7% mortality whereas the mortality was 18% and 36% on metoprolol succinate and placebo, respectively.47 Moreover, in the MADIT-CRT (multicentre automatic defibrillator implantation trial with cardiac resynchronisation therapy), patients with HF with NYHA functional class I and II with wide QRS complexes derived a significant 30% reduction in hospitalisation for HF or death with carvedilol when compared with metoprolol (HR=0.70, 95% CI 0.57 to 0.87, p=0.001), as well as a 39% reduction in the subgroup with implantable cardioverter-defibrillator (CRT-D; HR=0.61, 95% CI 0.46 to 0.82, p=0.001) and a 49% reduction in CRT-D patients with left bundle branch block (HR=0.51, 95% CI 0.35 to 0.76, p<0.001).48 Additionally, there was a marginally significant reduction in ventricular arrhythmias with carvedilol versus metoprolol (22% vs 26%, HR=0.80, 95% CI 0.63 to 1.00, p=0.050).
In patients with HF with DM, the Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) trial was a double-blinded, placebo-controlled trial, which enlisted 2289 patients within the group to carvedilol or placebo.49 ,50 In this trial, it was shown that the annual mortality rate in the carvedilol group was reduced by 35% (12.8% vs 19.7%, p=0.00013) and risk of death or hospitalisation reduced by 24% (p=0.00004) as compared with the placebo group. Owing to the overwhelming benefit of carvedilol as compared with placebo, the study was terminated early due to the mortality benefit in the carvedilol group. In patients with recent or recurrent CV decompensation or depressed cardiac function, the risk of death or hospitalisation due to a CV cause was reduced by 33% (95% CI 14% to 48%, p=0.002) and the risk of death or hospitalisation due to HF was decreased by 33% (95% CI 13% to 49%, p=0.002) in the group receiving carvedilol. In the group receiving carvedilol, patients also showed a lower incidence of hospitalisations due to HF (17.1% vs 23.7%, p=0.0001), for a CV reason (21.3% vs 27.7%, p=0.0003) or for any reason (32.2% vs 38.1%, p=0.003) as compared with the placebo group. Additionally, carvedilol in comparison with placebo showed a reduced incidence of all adverse effects (39.0% vs 45.5%, p=0.002), HF (p<0.0001), SCD (p=0.016), VT (p=0.019) and cardiogenic shock (p=0.003).
The US Carvedilol HF study was a RCT enrolling 1094 patients with chronic HF to receive either carvedilol or placebo.51 The mortality rate in the carvedilol group was reduced by 65% (3.2% vs 7.8%, 95% CI 39% to 80%, p<0.001), the risk of hospitalisation for CV causes was reduced by 27% (14.1% vs 19.6%, p=0.036), and the combined risk of hospitalisation and death was reduced by 38% (24.6% vs 15.8%, p<0.001). Owing to the clear survival advantage with carvedilol treatment, the trial had to be terminated early. There was also a greater decrease in the mean heart rate with the carvedilol group as compared with placebo (12.6±12.8 vs 1.4±12.2 bpm, p<0.001). This study confirms that carvedilol provides profound survival benefit over placebo in patients with chronic HF.
In the Australia-New Zealand HF trial, the researchers randomised 415 patients with chronic stable HF to receive either carvedilol or placebo.52 The results of this trial showed a 5.3% increase in the LVEF (p<0.0001) and decrease in the end-diastolic and end-systolic heart dimensions by 1.7 mm (p=0.06) and 3.2 mm (p=0.001) in the carvedilol group compared with the placebo group. The incidence of death or hospitalisation was also lower in the carvedilol group as compared with the placebo group (104 vs 131, RR=0.74, 95% CI 0.57 to 0.95). This trial showed beneficial effects of carvedilol on LVEF and cardiac dimensions in patients with HF.
A recent network meta-analysis comparing the BBs carvedilol, atenolol, metoprolol, bucindolol, bisoprolol and nebivolol indicated that carvedilol showed the greatest reduction in mortality (6.6% reduction) with a number needed to treat of 15 to prevent one death in patients with systolic HF.53 Moreover, carvedilol had the best tolerability (lowest pooled discontinuation rates) versus the other five BBs.
Finally, a systematic review and meta-analysis of randomised direct comparison trials of carvedilol versus β1 selective BBs was performed.54 Compared with β1 selective BBs used in HF (8 trials; n=4563), carvedilol significantly reduced all-cause mortality (RR=0.85, 95% CI 0.78 to 0.93, p=0.0006; table 2). This meta-analysis provides some rationale for the preferred use of carvedilol in patients with systolic HF versus β1 selective BBs. Despite this fact, larger RCTs are required to confirm these results as most of the benefit of carvedilol came from one trial (Carvedilol Or Metoprolol European Trial, COMET), which has been critiqued for comparing carvedilol to metoprolol tartrate (instead of succinate), and the use of a lower dose of metoprolol than what was used in MERIT-HF. However, heart rate was quite similar between carvedilol and metoprolol in COMET and thus somewhat diminished the credibility of this argument.
Carvedilol reduces all-cause mortality versus β1-selective BBs in patients with systolic heart failure and AMI54
Nebivolol
Nebivolol is a recently approved β1 selective BB with the unique effect of enhancing NO effects; decreased NO synthesis can exacerbate myocardial ischaemia through NO-dependent endothelial vasodilation.8 Furthermore, nebivolol inhibits the process of endothelial proliferation, which leads to the formation of atherosclerosis. The positive haemodynamic effects of increased NO synthesis include decreased peripheral vascular resistance and increased stroke volume, which can benefit the patient with HF.55 The Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors With Heart Failure (SENIORS) trial was a randomised study of elderly patients >70 years of age with HF. Nebivolol was effective in reducing the combined end point of mortality and morbidity irrespective of LVEF;8 ,56 ,57 however, this agent has relatively little data on CV event reduction in large cohorts with CHD. Two smaller trials have also concurred with the findings in the SENIORS trial in HF management. These studies looked at LVEF and exercise tolerability as their end points; nebivolol did show a significantly improved LVEF at 2 and 12 months.8 Among the commonly prescribed BBs, only carvedilol and nebivolol have vasodilating effects, thereby not causing reductions in CO and unlike the other BBs, neither of these drugs increases insulin resistance or risk for new-onset T2DM.58 ,59
Acute myocardial infarction
Approximately 715 000 people in the USA have an AMI per year.60 ,61 Moreover, CHD kills more than 385 000 people in the USA annually.59 ,60 As the cost of CHD in the USA is approximately $109 billion per year,59 ,61 medications that can reduce this burden are of utmost importance.
It has been shown that metoprolol and atenolol are frequently prescribed BBs in patients with MI.62 In the COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial), a randomised trial involving 45 852 patients with AMI, patients were randomised to receive intravenous and then oral metoprolol or placebo.63 The treatment group received up to 15 mg of intravenous metoprolol and 200 mg orally daily, thereafter. There was no statistically significant reduction in the primary composite end point of death, recurrent AMI or cardiac arrest (OR=0.96, 95% CI 0.90 to 1.01, p=0.10) or death alone (OR=0.99, 95% CI 0.92 to 1.05, p=0.69). Cardiogenic shock was seen in 5.0% of the patients randomised to metoprolol and 3.9% in the placebo group (OR=1.30, 1.19 to 1.41; p<0.00001). Reinfarction (2.0% vs 2.5%, OR=0.82, 95% CI 0.72 to 0.92, p=0.001) and VF (2.5% vs 3.0%, OR=0.83, 95% CI 0.75 to 0.93, p=0.001) were less frequently seen in the metoprolol-treated group. This study concluded that the early use of the BB metoprolol in patients who had experienced an AMI, though it reduced the risk of reinfarction and VF, it increased the risk of cardiogenic shock.63
The Carvedilol Post Infarction Survival Control in Left Ventricular Dysfunction (CAPRICORN) trial enrolled 1959 patients in this multicentre, randomised, placebo-controlled trial. Patients with a LVEF <40% and who had an AMI were randomised to carvedilol 6.25 mg twice daily or placebo.64 The primary end point was all-cause mortality or CV readmissions. All-cause mortality was lower in the carvedilol group compared with placebo (116 (12%) vs 151 (15%), 0.77 (0.60 to 0.98), p=0.03). Additionally, carvedilol caused a 76% reduction in arrhythmias (VT and VF/flutter, p<0.0001), a 52% reduction in supraventricular arrhythmias (p=0.0015) and a 26% reduction in SCD (p=0.098) compared with placebo.
The Carvedilol Acute Myocardial Infarction Study (CAMIS) trial enlisted 232 patients with post-MI to receive carvedilol or atenolol for a 12-month period. Patients received therapy within 24 h of onset of chest pain. There was no difference in the LVEF between the two groups and no significant reduction in the occurrence of a first serious CV event with carvedilol versus atenolol (RR=0.88, 95% CI 0.59 to 1.30, p=0.524).63 However, compared with atenolol, carvedilol was better tolerated (20% vs 33%; p=0.025) and there were numerically fewer deaths (2 vs 5, RR=0.39, 95% CI 0.08 to 1.95, p=0.25). This trial highlights the fact that carvedilol might be better tolerated than atenolol, but a larger trial is required to know if carvedilol is superior to atenolol in patients with post-AMI with normal LVEF.
A systematic review and meta-analysis of randomised direct comparison trials of carvedilol versus β1 selective BBs was performed on patients with AMI.54 Compared with β1 selective BBs (three trials, n=644), carvedilol significantly reduced all-cause mortality by 45% (fixed-effects model: RR=0.55, 95% CI 0.32 to 0.94, p=0.03) but not when the random-effects model was used (RR=0.56, 95% CI 0.26 to 1.12, p=0.10; table 2). Thus, carvedilol may improve outcomes compared with β1 selective BBs in patients with AMI; however, further RCTs are required. A more complete list covering the cornerstone trials in HTN, HF and AMI are provided in table 3.
Cornerstone hypertension, HF and AMI trials with atenolol, metoprolol and carvedilol
Conclusion
Numerous trials in patients with HTN indicate that atenolol should not be used as a first-line anti-HTN agent. Further trials are required to determine the optimal BB for use in patients with HF and AMI. Until then, the evidence strongly suggests that carvedilol may have an advantage over the first generation BBs in patients with HF and AMI, as carvedilol has the greatest amount of evidence for reducing CV morbidity and mortality in these settings and is effective in HTN with less adverse effects on lipids and promotion of DM.
References
Footnotes
Contributors JJD conceived the manuscript, performed the literature review and wrote parts of the paper. HF, AKN and DSB wrote parts of the manuscript and contributed select citations. SC, FD, EC, GB-Z, DSB and JHO reviewed and edited the manuscript.
Competing interests CJL has served as a consultant and speaker for GlaxoSmithKline (but not regarding β-blockers) and JHO has been a speaker for GlaxoSmithKline and Forest Pharmaceuticals. DSB has been a consultant for GlaxoSmithKline but not in the past 8 years.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.