Article Text

Abstract
We assessed whether long-term exposure to air pollution is associated with all-cause and cause-specific mortality during a period of declining particulate matter concentrations.
Approximately 4800 women aged 55 years from North Rhine-Westphalia, Germany, were followed for up to 18 years. Exposure to air pollution was assessed in two ways: (1) using the distance between the residential address and the nearest major road, as calculated from Geographic Information System data and (2) calculating 1-year average particulate matter concentrations below 10 µm (PM10) and nitrogen dioxide (NO2) levels using data from the nearest air-monitoring station data to the subjects’ residences. Ninety-two per cent of all subjects lived in the same community during the entire follow-up period. Associations between mortality and exposure were assessed using Cox's proportional hazards models, including confounder adjustment.
Sixteen per cent of women passed away during the follow-up period. An increase of 7 μg/m3 PM10 (IQR) was associated with an increased HR for all-cause (HR 1.15, 95% CI (1.04 to 1.27)), cardiopulmonary (HR 1.39, 95% CI (1.17 to 1.64)), and lung cancer mortality (HR 1.84, 95% CI (1.23 to 2.74)). An increase of 16 μg/m3 (IQR) NO2 exposure was associated with all-cause (HR 1.18, 95% CI (1.07 to 1.30)) and cardiopulmonary mortality (HR 1.55, 95% CI (1.30 to 1.84)). The association between cardiopulmonary mortality and PM10 was reduced for the extended follow-up period, during which PM10 concentrations (but not NO2 concentrations) were lower. Living close to a major road was associated with an increased relative risk for all-cause, cardiopulmonary and respiratory mortality. These associations were temporally stable.
Long-term exposure to ambient PM10 and NO2 was associated with increased mortality rates.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
The epidemiological evidence for the effects of long-term exposure to ambient air pollution on mortality during adulthood comes from 5 American,1–5 2 Canadian,6 ,7 4 European8–11 and 3 recently published Asian studies.12–14 In addition to these 12 prospective cohort studies, a recent systematic review reporting on the effects of long-term exposure to ambient air pollution on chronic diseases15 identified 20 case-control studies. A pooled relative risk (RR) of 1.06 (95% CI 1.03 to 1.10) for a 10 μg/m3 increase in PM2.5 was reported for all-cause mortality, with little heterogeneity observed between the six studies examined.15 The recently published results from a Canadian study reported an even higher adjusted hazard rate of 1.15 (95% CI 1.13 to 1.16), although air pollution concentrations were low.7 The combined RR across three studies2 ,4 ,8 was null for PM10 and TSP (total suspended particulate matter). The pooled RR for an increment of 10 μg/m3 NO2 was 1.00 (95% CI 0.99 to 1.02), but the heterogeneity across studies was substantial. Of the three studies which used ‘distance to major roads of less than 50 m’ as a proxy for exposure, two European studies found an increased risk for all-cause mortality,10 ,16 but the American study reported null findings.17 Cardiopulmonary causes of fatalitiy were not associated to NO2 in four cohorts,4 ,9 ,17 ,18 however, positive associations were observed in a German cohort of women.10 The pooled RR for the association between cardiopulmonary causes of fatality and PM2.5 across several publications6 ,11 ,16 ,19–21 was elevated (RR 1.14 (95% CI 1.09 to 1.18)).15 Suggestive evidence for an increased risk of cardiopulmonary causes of fatality attributable to living close to major roads was found in a few studies.15 Lung cancer mortality was not linked to NO2 exposure as the pooled RR for this association was null (RR 1.01 (95% CI 0.94 to 1.09)). Furthermore, substantial heterogeneity in the effect estimate was observed across the five studies.15 Conversely, the risk of lung cancer mortality was consistently found to be associated with PM2.5 (pooled RR: 1.21 (95% CI 1.1.0 to 1.32)), with little heterogeneity between studies. No clear association was found between living close to a major road and lung cancer mortality when the results from three cohorts were compared.15 Despite their similar underlying study designs, the 13 prospective cohort studies differed in their composition, size, space and time-related settings, exposure assessments, follow-up duration, outcome definitions and confounder control. Most of the cohorts were population-based and used area-specific levels of air pollutants assessed by one or more routine monitoring stations or a combination of urban background and local sources as the exposure. However, one study11 used a dispersion modelling technique, and another used satellite observations7 to estimate the ambient air concentrations at each subject's address. The methodological differences in the study designs of the 13 cohorts, the restricted follow-up duration, the small size of the European studies compared with some of the much larger American studies (eg, the American Cancer Society Study),2 and the lack of European data suggest that more long-term European studies are required. The German Women's Health Study in North Rhine-Westphalia is one of the nine cohorts assessing the effects of long-term exposure to ambient air pollution on mortality worldwide. Results for the first follow-up period (up to 2003) were published previously.10 Because of the substantially longer follow-up period currently available for this cohort, we are now able to report on causes of fatality with long latency periods. Furthermore, as the number of fatalities recorded in this cohort has doubled, we can also now consider rarer causes of fatality in our analyses.
Materials and methods
Study population and study area
This study was designed as a follow-up of a series of cross-sectional studies which examined the effect of air pollution on the health of women. All the cross-sectional studies were performed in the 1980s and 1990s in North Rhine-Westphalia.10 This area includes the Ruhr area, which is one of Europe's largest industrial zones. Online supplementary figure 1 shows the timing and number of participants recruited in each of the cross-sectional studies, as well as the number of participants who were successfully followed-up till 2008.
For each cross-sectional study, approximately 450 women in their mid-50s with German nationality, living in a number of industrial and two non-industrial reference areas (Borken, Dülmen), were randomly selected and asked to participate. The overall response rate for these cross-sectional studies was 70%. Combined, these cohorts consisted of 4874 women, although complete address information is only available for 4752 women. Geographically, this study population spans 10 areas in seven cities. The first follow-up period ended in 2003 and had a median and maximum follow-up time of 12.9 years and 18.2 years, respectively.10 The second follow-up period finished in October 2008, at which time information on vital status and migration had been collected for all 4752 women included in the current study.
Residential mobility, vital status and causes of fatality
Residential mobility, vital status and address information were obtained for the 4752 women by contacting the residential registration offices. Information as to whether the subject was still living at the same address as during the baseline survey was provided by the residential registration offices. These offices also provided the new addresses of subjects who had moved, as well as the location of fatality when appropriate. In total, 74.5% of participants had not moved since recruitment, 17.5% had only moved within the community at which they were initially registered, and only 7.8% moved outside their community at baseline. For those who had moved to a different community, more than 150 local residential registration offices were contacted in order to obtain information on the vital status of participants. This procedure was repeated for subjects who had moved several times. Of the 4752 women with complete address information at baseline, only 10 could not be traced at the time of follow-up. In total, 740 (16.0%) of the participants had passed away by the end of 2008. Data on cause of fatality were provided by the ‘North Rhine-Westphalia state agency for data processing and statistics’. Only 15 of the 740 (2.0%) fatalities were due to unknown causes. For one woman, the date of fatality could not be determined. Women who passed away outside the State of North Rhine-Westphalia were more likely to have an unknown cause of fatality. Causes of fatality were coded according to the International Classification of Diseases, Ninth Revision (ICD-9), using the underlying causes of fatality in part 1 of the death certificate. All-cause mortality and cause-specific mortality (which includes cardiovascular (ICD-9 codes 400-440.9), pulmonary (ICD-9 codes 460-519.9), cardiopulmonary (ICD-9 codes 400-440.9 or 460-519.9), lung cancer (ICD-9 code 162-162.9) and respiratory causes (ICD-9 codes 460-519.9)) were the primary outcomes of interest, as defined according to Gehring et al.10
Estimation of exposure
We used NO2 and PM10 (derived from TSP as surrogates for air pollution, as previously described elsewhere.9 One-year average concentrations for each pollutant were calculated for the year of the baseline examination (which was from 1985 to 1994; see online supplementary figure 1) using continuous air pollution measurements (half-hourly measurements for NO2 and 24 h measurements for TSP). NO2 concentrations were measured by means of chemiluminescence, and TSP levels were measured at state routine monitoring sites by β absorption. PM10 was calculated as 0.71×TSP for all monitoring sites. The factor of 0.71 was derived from parallel measurements of PM10 and TSP at seven monitoring sites in the study area. Further details are available in Gehring et al.10 Since the same conversion factor was used for all monitoring sites, the reported mortality effects for PM10 are the same as that for TSP. Each participant's exposure at enrolment was defined as the annual average recorded at the monitoring station closest to the residential address. Online supplementary figure 2 shows the locations of the participants’ baseline addresses and the monitoring stations. The majority of the subjects (65.2%) were living within a distance of less than 5 km from a monitoring site (see online supplementary figure 2). Air pollution levels measured in Borken (which is close and comparable with Dülmen) were used for Dülmen, as no monitoring station data were available for this area. The measurement of air pollution in Borken only began in 1990 and 1991 for NO2 and TSP, respectively. Therefore, air pollution concentrations prior to these dates were imputed by adding an ‘average’ difference in air pollution levels between 1990 and 1991 and the respective year to NO2 and TSP concentrations measured in 1990 and 1991. The ‘average’ difference was estimated by a linear regression model with air pollution concentration as the dependent variable, and year of measurement as the independent variable. An autoregressive (AR(1)) correlation between repeated measurements taken at the same site was calculated. Since 1998, PM10 is directly measured at several monitoring stations in the study area.
We were able to geo-code 4615 (97.1%) of the participants’ baseline addresses. The proximity of the home to major roads (defined as roads with at least 10 000 cars/day) was calculated for 4230 (91.7% of the geo-coded addresses) participants using a geographic information system which incorporated traffic count data provided by the North Rhine-Westphalia State Environment Agency. We were unable to calculate the distance to a major road for participants with unknown addresses at the time of enrolment, or for those living close to the German border or the border of the State of North Rhine-Westphalia. For these latter two cases, the buffer around the residential address includes areas for which road network data are unavailable.
Confounding variables
As part of the cross-sectional studies, all participants completed a self-administered questionnaire on education, current symptoms/diseases, medication use, smoking, occupational exposures and use of gas for cooking and/or water heating. In addition, 81% of the women underwent a physical examination that included height and weight measurements, which were subsequently used to calculate body mass index (BMI). Confounder variables were selected a priori, and are the same as those considered in Gehring et al. Socioeconomic status (SES) was defined as the maximum education level achieved by the study participant or her partner, and was classified into three categories: low (compulsory school only), medium (lower and upper secondary education), and high (postsecondary education, including university). Environmental tobacco smoke (ETS) exposure at home and/or at the workplace was considered passive smoking. Current smokers were classified into three categories according to the number of cigarettes smoked. Smokers with missing information on the number of cigarettes smoked were assigned to the highest category. Participants who provided no information on smoking were classified into a separate category. BMI was classified as underweight/normal (<25 kg/m2), overweight (25–30 kg/m2), and obese (≥30 kg/m2), according to WHO classifications.22
Statistical analysis
Correlations are presented as Spearman's rank-order correlation coefficients. Associations between mortality and exposure were analysed using Cox's proportional hazards models including adjustment for potential confounders (age and smoking history). Hypertension and asthma were included in some models as potential confounders in sensitivity analyses. For participants who passed away, the time in the study was calculated as the difference between the date of the baseline cross-sectional study and the date of fatality. For those alive at the end of follow-up, the time in the study was calculated as the difference between the start and end of follow-up. For participants who moved during follow-up and were subsequently lost, the time in the study was calculated as the difference between the start of follow-up and the last date when the vital status and place of residence were known. For the Herne study area, no data on moving was available beyond 2003. In the analysis of cause-specific mortality, participants who passed away from causes other than those analysed were excluded. We conducted sensitivity analyses to assess differences between movers and non-movers, subjects recruited between 1985 and 1987, and those recruited in 1990, and subjects included in the first follow-up (until 2003) and those also included in the second follow-up (2004–2008). Results are presented as crude and adjusted HR with 95% CI. Statistical analyses were calculated with the survival package of the R statistical program, V.2.13. Geographic information system calculations were completed with Arcinfo (ESRI Inc, Redlands, California, USA).
Results
Description of the study population and exposure
Complete address information was available for 4752 participants. The 122 women without address information at baseline did not substantially differ in sociodemographic and health characteristics from those with known baseline addresses (data not shown). Table 1 shows the baseline characteristics of the study participants. In total, 84% of women reported living 5 years or longer at their current address. Seventy-five per cent of all participants had not moved since baseline and less than 8% had moved outside their community during the entire follow-up (from baseline to 2008). The median and maximum lengths of follow-up were 18.4 and 21.9 years, respectively. Sixteen per cent of the cohort passed away (n=740) during follow-up (table 1). Survivors were of higher SES compared with the deceased, and had a lower prevalence of current smoking. Asthma, hypertension and obesity were less common in the survivors. Furthermore, survivors tended to have homes further away from major roads. Out of the 740 deceased women, 715 (96.6%) passed away from natural causes, 1.4% passed away from unnatural causes, and the cause of fatality is unknown for 15 (2.0%) women (see online supplementary table 1). One-third of the deceased passed away from cardiovascular causes. Respiratory causes (4.7%) and lung cancer mortality (5.5%) were uncommon. There was a considerable range in exposure to PM10 (34.8–52.5 µg/m3) and NO2 (20–60 µg/m3) (see online supplementary table 2). PM10 and NO2 were significantly correlated (Spearman's correlation coefficient r=0.5). A considerable decrease, especially in PM10 concentrations, was observed after 1985.
Description of the study population: n=4752 woman aged 50–59 years recruited at the baseline investigation (from 1985 to 1994), followed-up until 2008
Associations between mortality and air pollution exposure
Estimates for the associations between all-specific and cause-specific mortality and long-term exposure to PM10 and NO2 are shown in table 2. Higher NO2 annual averages significantly increased the risk of all-cause and cardiopulmonary mortality, but not of lung cancer and respiratory mortality after adjustment for educational level (SES) and smoking history. An IQR-increment of 7 µg/m3 PM10 significantly increased the risk of all cause-specific death rates, except respiratory (table 2). Additional adjustments for hypertension and asthma only marginally changed the results (data not shown), and all-effect estimates remained statistically significant. All-cause and cardiopulmonary mortality risks increased slightly when the analysis was restricted to the 75% of study participants who never moved during follow-up (see online supplementary figure 3; The corresponding numbers for lung cancer and respiratory mortality were too small to show stratified effect estimates with sufficient precision).
Hazard rate ratios (95% CI) between all-cause, cardiopulmonary and lung cancer mortality, and an IQR* increase in air pollution concentrations and distance to roads with >10 000 cars/day
Across the whole population, hazards for all-cause and cardiopulmonary mortality were lower for women living farther than 50 m from a road to the nearest road with a median daily traffic volume above 5000 cars at enrolment (for figure 1, a 5000 car cut-off was used instead of 10 000 in order to get sufficiently large numbers) (figure 1). More pronounced effects for all-cause and cardiopulmonary mortality were found among non-movers (see online supplementary figure 3). No association between the rate of mortality and the distance to the nearest major road was observed for lung cancer, and this result was also not statistically significant for respiratory causes of fatality (data not shown).
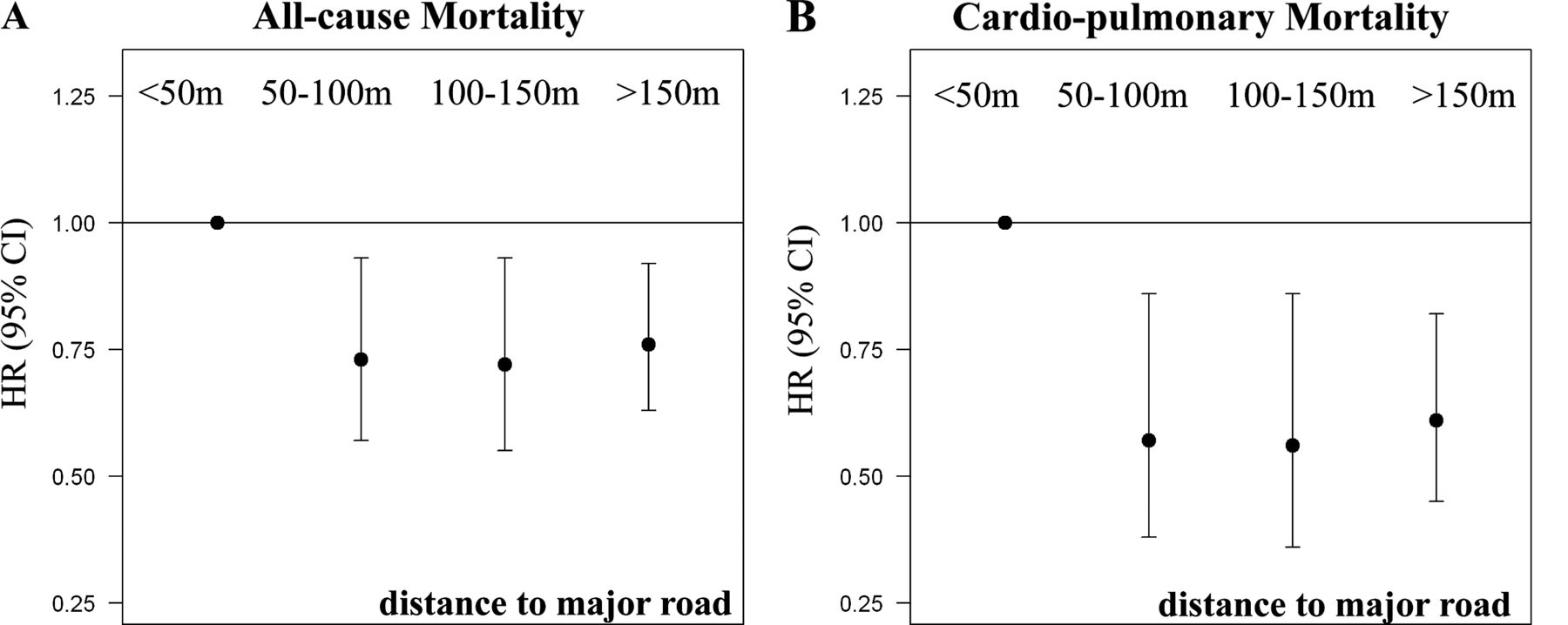
Decreasing HR for mortality with increasing distance of residential address to major roads (>5000 vehicles/day) at baseline. Cox proportional hazard models adjusted for age, educational level and smoking status.
Comparisons between mortality effects assessed at the first follow-up (up to 2003) and those assessed at the extended follow-up (up to 2008)
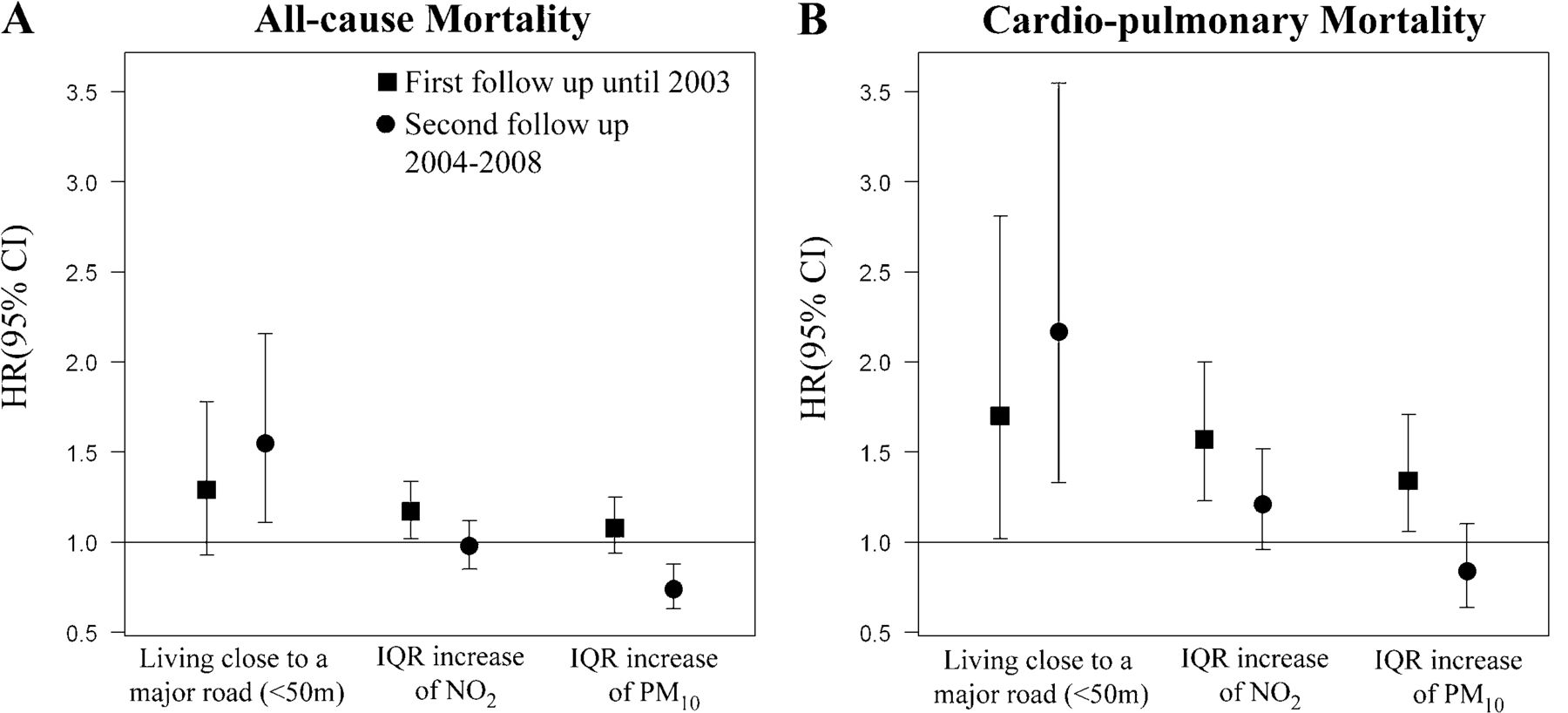
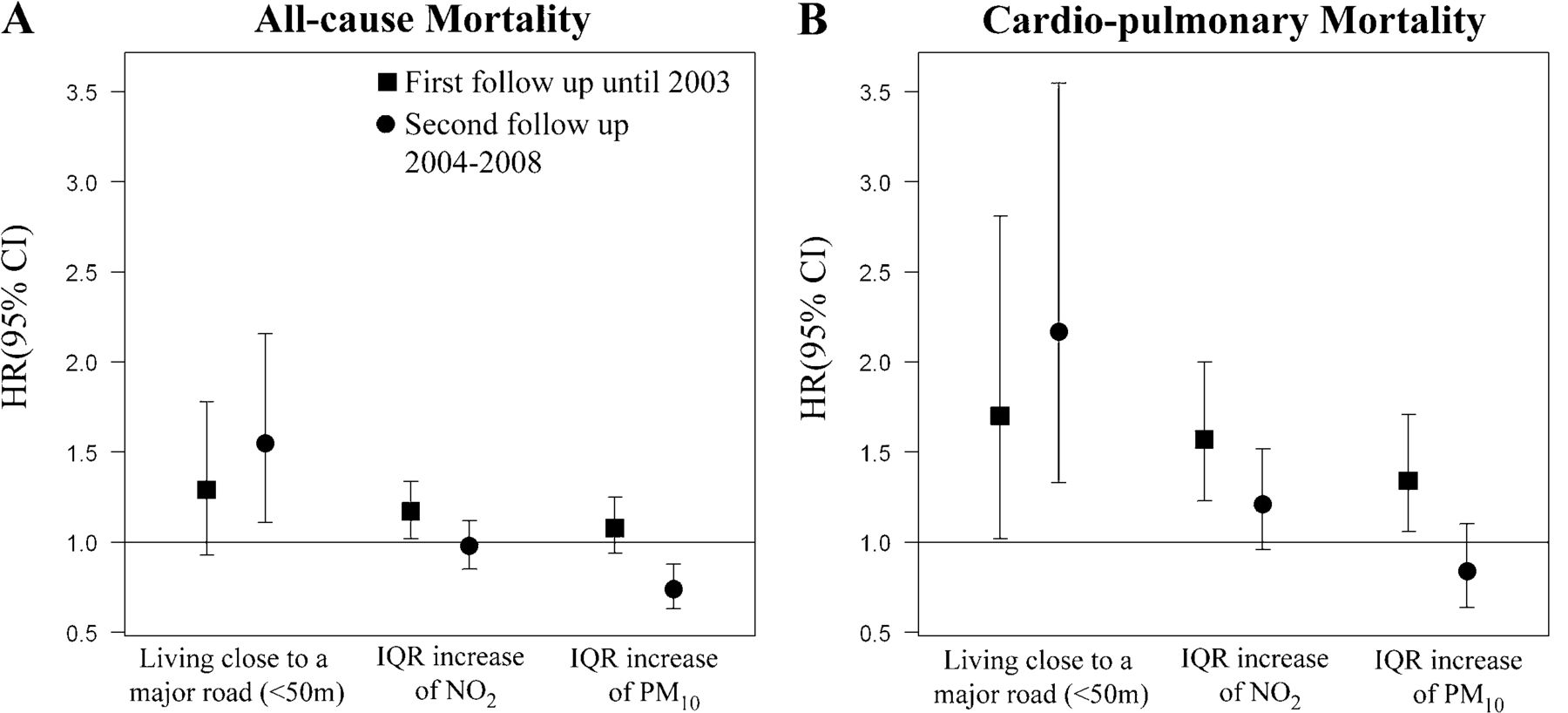
We compared the mortality risks within the cohort at two time periods: up to 2003 and from 2003 to 2008 (figure 2). The effect estimates for the associations between all-cause and cardiopulmonary mortality and PM10 and NO2 were lower for the extended follow-up. However, the effect estimates were greater when considering the distance from a participant's home to a major road and the same two outcomes. The number of fatalities due to respiratory causes and lung cancer are too small to allow a similar comparison.
{kind=link}
{kind=link}
Comparison of adjusted HR for all-cause and cardiopulmonary mortality between the first (up to 2003) and second follow-up (2004–2008), excluding subjects who passed away before 2004.
Sensitivity analysis for potential cohort effects
Sensitivity analyses for the subcohorts recruited in 1985–1987 (8 subcohorts) and in 1990 (8 subcohorts), were performed to disentangle spatial differences from temporal changes of ambient air pollution levels (table 3). We restricted the follow-up for all subcohorts to 18 years in order to increase comparability. The HR for PM10 in relation to all-cause and cardiopulmonary mortality were substantially lower for the 1990 subcohorts compared with the 1985 subcohorts, and were no longer statistically significant. For the two indicators of traffic-related air pollutants, NO2 and living close to busy roads, the HRs were generally higher in the 1990 subcohorts than in the 1985–1987 subcohorts. The sample sizes are too small for lung cancer and respiratory mortality to allow any meaningful comparisons.
Sensitivity analysis comparing the adjusted (education, smoking status) hazard rate ratio* for the subcohorts recruited between 1985–1987 and those recruited in 1990, restricted to a similar follow-up duration of 18 years
Discussion
Using the women's cohort in North Rhine-Westphalia, we found an association between increased all-cause mortality and long-term exposure to PM10 and NO2. In addition, we found an inverse association between the distance of the residential address to a major road and all-cause mortality. The same trends were found for cardiopulmonary mortality. Furthermore, lung cancer mortality was associated with increasing exposure to PM10, but not NO2.
Comparisons with findings of other cohort studies
Our results on all-cause mortality and PM10 are consistent with the findings of five other cohorts which used PM2.5 as their exposure of interest, as well as7 ,15 with the extended follow-up of the Harvard Six Cities Study.19 However, two other cohorts have reported null findings for PM10. The association between NO2 exposure and all-cause mortality that we observed has been already documented.10 However, the other cohort reported no associations between NO2 and mortality,15 except in two Asian cohorts.12 ,14 Among the three studies which used distance to roads as the metric of exposure, positive associations were found for living within 50 m of a major road in a Dutch study (RR: 1.05 (95% CI 0.93 to 1.78))16 and in the previously published first follow-up of this current study.10 The results in an American study were null.17
Our findings of a statistically significant effect of PM10 exposure on cardiopulmonary mortality confirms previous findings reported in eight cohorts,7 ,9 ,12 ,14 ,16–19 as well as the findings from the first follow-up of this cohort.10 The pooled-effect estimate for NO2 and cardiopulmonary mortality, using data published up until 2007, was not significantly different from 1.0.15 However, a recently published large study from Japan reported significantly increased risk for this association (adjusted HR 1.16 (95% CI 1.06 to 1.26 per increment of 10 µg/m3 of NO2)).12 Another recent and large cohort study from China also reported significantly increased risks for cardiopulmonary causes of fatality associated with NO2 exposure.14 These recently published findings are consistent with the results of this study. There is also suggestive evidence for increased cardiopulmonary and cardiovascular mortality risks associated with living close to busy roads.15 ,23
Most previous cohort studies have used PM2.5 as an exposure metric to investigate the long-term effects of ambient particulate matter on lung cancer.7 ,15 ,19 Four cohorts found positive associations between exposure to PM10 or PM2.5 and lung cancer mortality,4 ,11 ,13 ,19 but not all estimates reached statistical significance. For PM2.5, the pooled-effect estimates of studies published before 2007 were statistically significant, and there was little heterogeneity across studies.15 Our study adds substantial evidence to the current body of knowledge regarding the effects of PM10 on lung cancer, and is in line with the known adverse effects of PM2.5 exposure. Furthermore, our null finding regarding the effects of NO2 exposure on lung cancer mortality is consistent with a previously published combined null estimate of 1.01 (95% CI 0.94 to 1.09), which is based on five other cohorts.16
Using NO2 and distance to major roads as surrogates for exposure to traffic sources, our study strengthens the evidence that long-term exposure to particulate matter and traffic-related air pollution increase the risk of all-cause, cardiopulmonary and lung cancer mortality. When comparing adverse health effects of a fixed site monitoring exposure strategy with a distance to major road scenario, we have to consider that these assessments capture within urban variation of ambient air pollutants differently. While the distance to a major road is a better method of assessment than using data from a fixed monitoring site, land use regression models are superior to both exposure assessments used in this paper.
Due to a long median follow-up of 18.4 years, we are able to evaluate and quantify the mortality risks for diseases with long latencies, such as lung cancer. Our study results and the findings of other cohorts are strongly consistent, despite differences in study design, study populations, sources of ambient air pollution, exposure assessments, climatic conditions and more general differences regarding space and time, which highlights the robustness of the association between long-term exposure to ambient air pollution and mortality.
Strengths and limitations
This study has several strengths, but also limitations which need to be cautiously considered before drawing conclusions.
The restriction of the study population to women with German nationality has several strengths. Women are less exposed to air pollutants at the workplace, and smoking was not very common in women born between the middle of 1930 and the middle of 1935. Furthermore, women of this age were mostly working within their homes during follow-up. Thus, potential mortality effects due to ambient air pollutants were less likely diluted by air pollution exposures at places other than the home. A further major strength of this study is the low rate of moving. From all 4752 enrolled women, 92.2% lived in the same community until the end of follow-up. Furthermore, more than 80% of the women had already lived longer than 5 years at the same place of residence at the time of enrolment. Therefore, we consider our exposure assessment of ambient air pollution at the residential address at enrolment to be well justified. Another major strength of this study is the ability to adjust for individual level risk factors. This detailed adjustment is usually not possible in larger cohort studies examining long-term effects. This strength helps compensate for the relatively small sample size of our study. Sensitivity analyses restricted to non-moving women had only very limited impact on the effect estimates. However, the restriction of this cohort to such a specific population does weaken the generalisability of the study results with respect to men.
Due to the fact that the cohort was enrolled over the period of a decade, there are differences in the duration of follow-up and also in the time-dependent composition and level of ambient air pollution exposures.
A major limitation of the exposure assessment is that two non-industrial reference areas (Borken and Dülmen) had only one central fixed monitoring site located at Borken. Thus, the data derived from this Borken site was also used for the Dülmen region, despite the fact that the distance between Borken and Dülmen is similar to the distance between the other areas. Moreover, air pollution measurements only started in 1990/1991, and we had to impute pollutant concentrations prior to this date. Therefore, the exposure assessment in the non-industrial reference areas is based on assumptions which may be biased. During the study period of 1985 through 2008, a strong decline of ambient particulate matter concentrations occurred in the study area (see online supplementary figure 4), mostly due to clean air actions within industries. Local traffic also changed with respect to traffic volume, composition of car fleets, number of diesel cars, volume of inner-city traffic due to increases in bypasses and so on. Most of the temporal source and emission level changes are difficult to quantify. Findings based on estimates of air pollution concentrations at the time of enrolment should be interpreted with caution, especially with respect to health outcomes with long latency periods. The decreased hazard rate ratio for PM10 observed during the second follow-up (figure 2) could be attributed to the decreasing PM10 levels seen over time. Likewise, the similar effect sizes found for the traffic indicators may reflect the fact that no major temporal trends in traffic-related air pollutants occurred. Table 3 compares mortality risks between the subcohorts recruited in 1985–1987 and 1990. For the 1990 subcohort, no increased risks were found for PM10, but positive associations were found for living close to busy roads. We speculate that air pollutants originating from motor vehicle traffic dominate air quality and, consequently, potential mortality risks. Our exposure assessment approach, which included urban background levels derived from fixed monitoring sites and local traffic-related pollution estimated using distance to major roads, is a major strength of this study. However, recently developed land use regression models are better at capturing spatial variations in exposure than using an exposure assessment based solely on fixed monitoring sites. Several studies have shown the importance of within-urban variation, in particular for fine particulate matter, which are not always captured by fixed monitoring sites.17 This limitation needs to be considered when effect estimates based on fixed monitoring sites are compared with those calculated using distance to roads as the exposure.
The study population consists of women living in a number of industrial and non-industrial cities in the Ruhr area. Cities were chosen to represent a large range in air pollution concentrations. One potential limitation of this design might be that women from industrial zones differ from women living in non-industrial zones, not only in terms of air pollution concentrations (which is the case in the current study for NO2 and proximity to roads, but not for PM10), but also with respect to socioeconomic and lifestyle factors that are associated with mortality. We controlled for confounding by socioeconomic factors by adjusting for education and also for occupational exposures. However, no detailed information on lifestyle factors, such as diet, is available. Therefore, we cannot completely rule out the possibility that our results may be affected by residual confounding attributable to other lifestyle factors that are risk factors for cardiovascular disease or lung cancer, and which may vary by study area. However, a sensitivity analysis with additional adjustment for BMI categories only slightly attenuated the mortality effect estimates, which remained statistically significant.
The assessment of cause of fatality using official death certificates could be considered a limitation, as using only this method to assign cause of fatality is often criticised.24–27 However, the degree of error is greatest when the causes of fatality are coded in great detail (such as for rare cancer locations and other rare diseases), and is likely to be a major limitation in our study which used highly aggregated classifications. Using death certificates to assign lung cancer mortality was judged as sufficiently sensitive and specific in the USA.28
A further strength of this study is the low rate of loss of follow-up. On average, almost all women could be tracked over a period of 18.4 years.
Conclusion
The association between cardiopulmonary mortality and PM10 was less pronounced in this extended follow-up study compared with that previously reported during the first follow-up of cohorts, possibly due to lower PM10 concentrations in general, as well as smaller differences in air pollution concentrations across the study areas over time. This convergence effect was less pronounced for NO2. Living close to major roads was associated with increased RRs for all-cause and cardiopulmonary mortality, and this result was temporally stable.
What this study adds
-
This study provided estimates for mortality effects of long-term exposure to ambient air pollution from Germany. These estimates should be considered when re-evaluating European guidelines for air quality standards.
-
All-cause, cardiopulmonary and lung cancer mortality increased with increasing exposure to PM10.
-
Increased NO2 exposure was associated with a significantly elevated hazard rate ratio for all-cause and cardiopulmonary mortality.
-
Living close to major roads was associated with an increased relative risk for all-cause, cardiopulmonary and respiratory mortality.
Acknowledgments
The authors thank Peter Bruckmann, Ulrich Pfeffer and Alfred Doppelfeld (LANUV-NRW, Essen) for providing air pollution monitoring data; Thomas Kuhlbusch (IUTA, Duisburg) for calculating the conversion factor used to obtain PM10 from TSP; Brigitte Wirsig (State Office for Statistics, NRW, Duesseldorf) for providing data on causes of fatality; Bernhard Schwertner for the identification of life status; Elke Link (IUF, Duesseldorf) for her assistance with the GIS data; and Elaine Fuertes for editing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
- Data supplement 2 - Online table
Footnotes
-
Contributors JH wrote the manuscript, ET did the final statistical analysis and is responsible for the modelling, while PR and UG were involved in statistical analysis planning, MH did the GIS work. In addition to these contributions, UK, KR and H-EW helped with discussion and interpretation of the results.
-
Funding This study was exclusively funded by North Rhine-Westphalia State Environment Agency (LANUV-NRW) of the Ministry of the Environment and Conservation, Agriculture and Consumer Protection North Rhine-Westphalia (MUNLV), Duesseldorf, Germany.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Landesaerztekammer Bayern.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/