Article Text

Abstract
Background Non-invasive ventilation (NIV) is an efficient method for treating respiratory failure in patients with amyotrophic lateral sclerosis (ALS). However, it requires a process of adaptation not always achieved due to poor compliance. The role of telemonitoring of NIV is not yet established.
Objectives To test the advantage of using modem communication in NIV of ALS patients.
Design Prospective, single blinded controlled trial.
Population and methods According to their residence, 40 consecutive ventilated ALS patients were assigned to one of two groups: a control group (G1, n=20) in which compliance and ventilator parameter settings were assessed during office visits; or an intervention group (G2, n=20) in which patients received a modem device connected to the ventilator. The number of office and emergency room visits and hospital admissions during the entire span of NIV use and the number of parameter setting changes to achieve full compliance were the primary outcome measurements.
Results Demographic and clinical features were similar between the two groups at admission. No difference in compliance was found between the groups. The incidence of changes in parameter settings throughout the survival period with NIV was lower in G2 (p<0.0001) but it was increased during the initial period needed to achieve full compliance. The number of office or emergency room visits and inhospital admissions was significantly lower in G2 (p<0.0001). Survival showed a trend favouring G2 (p=0.13).
Conclusions This study shows that telemonitoring reduces health care utilisation with probable favourable implications on costs, survival and functional status.
- motor neuron disease
- respiratory medicine
- telemetry
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is a progressive and fatal neurodegenerative disease in which respiratory insufficiency is the most common terminal event. Non-invasive positive pressure ventilation (NIV) has become the standard management to respiratory impairment by increasing quality of life and reducing the likelihood of resorting to tracheostomy.1–8 Improved rate of survival and quality of life seem to correlate with the earlier prescription of NIV, before diurnal signs of respiratory failure have been established, with a forced vital capacity (FVC) of >50% of the predicted value or at detection of early signs of impending nocturnal respiratory insufficiency.7 9–11
NIV requires a dynamic process of adaptation which is achieved in an unknown proportion of patients. Probably, patients with severe bulbar weakness and marked sialorrhoea have the highest rate of poor compliance.12 13 In fact, compliance with NIV is a complex issue and a recent matter of debate.9 14–17 Certainly, improved tolerance and compliance can only be reached by continuous customised setting of the device, which depends on many factors, such as lung mechanics,16 18 inspiratory and expiratory triggers, breathing frequency,19–21 effective correction of blood gases12 22 and different metabolic demands. Compliance with NIV in ALS has only been evaluated in terms of the number of hours of usage a day, which is very limited. Nevertheless, most authors have reported longer survival in patients using NIV for more than 4 h per day.3 22–24
Recent technological advances have allowed for more extensive control of the relevant sets in addition to analysis of the number of hours/day of utilisation. It is possible to assess breath pressures and volumes, the percentage of utilisation of a predetermined target pressure, respiratory rate, peak flow, number of apnoeas, percentage of leaks and oxygen saturation on pulse oximetry. It is also possible to perform online checking and correction via modem connection, hopefully increasing patient comfort, tolerance and compliance.25 Nonetheless, the advantages of these new technologies have scarcely been evaluated in neuromuscular patients.26
To the best of our knowledge, only one study has compared the effectiveness of an outpatient initiation protocol with the standard inhospital model for NIV.22 No study has evaluated the impact on compliance, function, survival and healthcare utilisation of ALS patients submitted to wireless telemetry to control NIV settings, compared with the office visit approach. We aimed to investigate this relevant problem.
Patients and methods
From January 2003 to September 2006, all consecutive ALS patients ventilated with a Goodknight 425ST bi-level device (Tyco Healthcare Group LP, California, USA) were screened and considered for inclusion in a prospective and controlled trial if at diagnosis they had no signs or symptoms of respiratory insufficiency with an FVC ≥75% of the predicted value, Pao2 ≥80 mm Hg and Pco2 ≤45 mm Hg, and age between 18 and 75 years. Patients with gastrostomy, cognitive impairment or other significant disorders were also excluded from this trial. Patients were randomly assigned to one of two groups according to their residential area. Patients included in group G1 (control) were living in Lisbon; in this group managing of NIV settings and assessment of compliance were performed through regular office visits on admission, 2–3 weeks later and then every 3 months. Patients included in group G2 (intervention) were living outside Lisbon and follow-up was performed by weekly modem telemonitoring, in addition to regular office visits at each 3 month interval. All participants were evaluated with the ALS Functional Rating Scale (ALSFRS) every 3 months by a physician blinded to the study group. Respiratory functional tests were performed every 6 months by a technician unaware of the study. All received a helpline number, in addition to regular office visits.27 28 Trial duration was established from NIV adaptation to a follow-up period of 3 years or death.
ALS patients were ventilated in accordance with a set of criteria that included clinical symptoms, conventional respiratory function tests, as recommended by the American Academy of Neurology2 (including FVC and maximal inspiratory pressure), neurophysiological studies and nocturnal pulse oximetry.9 10 NIV was indicated as early as patients agreed after the first symptoms and signs of changes, in an office based setting. NIV is optimised to improve clinical symptoms and nocturnal pulse oximetric changes. The procedure includes slow increments in inspiratory positive air pressure (IPAP) in order to achieve a steady state with normal breathing patterns, normal pulse rate and Spo2 >95%, with the backup rate slightly lower than the patient's own respiratory frequency.
For NIV compliance follow-up and flexible parameter settings changes, all participants received a helpline to clarify any doubts or to seek medical advice whenever difficulties arose. Patients in G1 were, in addition, also observed 2–3 weeks after entry and patients in G2 had a modem pre-installation programmed to communicate every week. Anticipating difficulties and constraints imposed by continuously monitoring and storing data, patients in G2 were further instructed to activate the system once a week or whenever they felt uncomfortable with the device, after phoning the physician in charge, and were instructed to call the helpline when needed.
A crucial element of the telemedicine instrument functionality is the remote transmission of data. The instrument is equipped with an internal modem, allowing direct access to the internet via a TCP/IP protocol along with data storing at the patient's home. The bidirectionality of the system allowed us not only to register compliance data but also to introduce modifications in parameter settings, thus permitting real time evaluation of its impact on ventilatory mechanics. Regarding the device used in this study, the bi-level instrument included backup rate/assist control as well as patented FlowSens technology that allow the physician to customise the inspiratory and expiratory settings for greater patient comfort and synchronicity.
In addition, an intermediate level of care was set up to detect and flag alarm signs requiring an immediate revision of settings. This monitoring was performed by one of the authors (JP) who, after reviewing the synthesis report or night calendar, was instructed to send a message to the physician who would then decided on possible setting changes, schedule an office visit, schedule a phone call or conduct a real time communication. As there are no published or established alert signs for home ventilation in rapidly progressive neuromuscular disorders, we considered all data that were ±1 SD of the mean values of IPAP, expiratory positive air pressure, inspiratory/expiratory ratio, backup rate, inspiratory sensitivity, expiratory sensitivity and rise time as alert signs. These limits were defined by data analysis of 67 ALS patients with regular NIV use ≥6 h a day followed in our unit (unpublished data). In addition, we also considered as an alert sign all data conflicting with the preceding ventilation profile of the patient.
Primary outcome
We considered two primary outcomes measurements: (1) the number of office and emergency room visits, and hospital admissions during the entire period of NIV use; and (2) the number of parameter setting changes during the period (number of days, DTC) needed to achieve full compliance (defined as NIV use >6 h) and throughout all periods of NIV use.
Secondary outcomes
As secondary outcome measures we considered clinical and functional disease progression, as defined by ALSFRS total score, respiratory, spinal and bulbar subscores (every 3 months), respiratory functional tests (very 6 months), total survival (total number of days from symptoms onset to death or the end of the study), survival from first visit (total number of days from diagnosis to death or the end of the study) and survival with NIV (total number of days from NIV adaptation to death or the end of the study). In addition, we also recorded the type of parameter setting change and compliance, assessed by the number of hours of usage a day; percentage of spontaneous breathing; backup respiratory rate; average, minimum and maximal respiratory rates; and percentage of attained predetermined pressures.
In this study, all patients gave written informed consent after protocol approval by the local ethics committee. As this was a pilot study, sample size considerations were not based on a predefined clinically significant difference in health resource utilisation and survival probability but rather on studying the minimum number of subjects (20 per group) that would allow the application of large sample statistical methods.
Statistical analysis
Demographic and baseline clinical and respiratory function data were analysed for homogeneity between groups with two sample t tests and Fisher's exact test. Event count data, such as healthcare utilisation data (number of office visits, hospital admissions and emergency room admissions, number of parameters changes and number of DTC) were analysed with the person years method and reported as incidence rate ratios with exact Poisson confidence intervals and significance tests. Repeated measurements data (panel data) on parameters settings and patient compliance were analysed with random effects regression. Survival was analysed with the Kaplan–Meier method and survivor functions were compared with the log rank test. Student's t tests and Fisher's exact test were used throughout as appropriate. Differences were considered statistically significant at p<0.05. All tests are two tailed. Statistical analysis was performed with STATA 10 (Stata Corporation).
Results
Of 155 consecutive home ventilated ALS patients, 51 were excluded because they were ventilated with devices that did not allow compliance analysis through modem communication. A group of 62 additional patients were excluded because they had FVC values lower than 75% of the predicted value. Among the 42 eligible patients, two refused to participate and were excluded. The final analysis set comprised 20 patients in the control group (G1) and 20 patients in the intervention group (G2), but one patient in G2 was lost to follow-up and hence was excluded from the analysis. (figure 1) No difference was found in terms of demographic data, clinical characteristics and respiratory function tests between the groups at diagnosis or at NIV adaptation, except for FVC which was significantly higher in G1 at diagnosis (p=0.04) (tables 1 and 2). Moreover, mean values for the initial parameter settings of NIV at the time of non-invasive ventilation onset were not different, showing that the procedure was similar in both groups.

Population and methods (flowchart). ALS, amyotrophic lateral sclerosis; FVC, forced vital capacity; NIV, non-invasive ventilation.
Demographic and baseline clinical characteristics at diagnosis
Respiratory evaluation at NIV adaptation
Primary outcome
Table 3 shows the incidence data regarding the number of office and emergency room visits and inhospital admissions. The incidence rate was 3–6 lower in G2 patients (p<0.0001). Random effects regression analysis of the overall difference in the type of parameter setting changes throughout the ventilation period showed no differences between the groups. The same negative results were observed in comparison of compliance data although a trend towards a greater number of daily hours of NIV use in group G2 was observed (p=0.17).
Results of the primary outcome—healthcare utilisation
Secondary outcomes
The number of changes in parameter settings during DTC and over the entire period of NIV showed a slightly higher incidence rate in G2 during the initial period of adaption (20%, p<0.01%) but a clearly lower rate over the entire period of NIV (50%, p<0.0001) (table 4).
Results of the secondary outcome—incidence rate of parameters setting number of changes
The clinical progression rate prior to NIV adaption showed no differences between the groups for total ALSFRS score or for bulbar and spinal subscores. Respiratory subscore tended to progress faster in G1 (p=0.04). However, after NIV adaptation, the random effects general linear model regression analysis did not show statistically significant differences in clinical progression, despite a trend for slower progression of the spinal subscore in G2 (p=0.15).
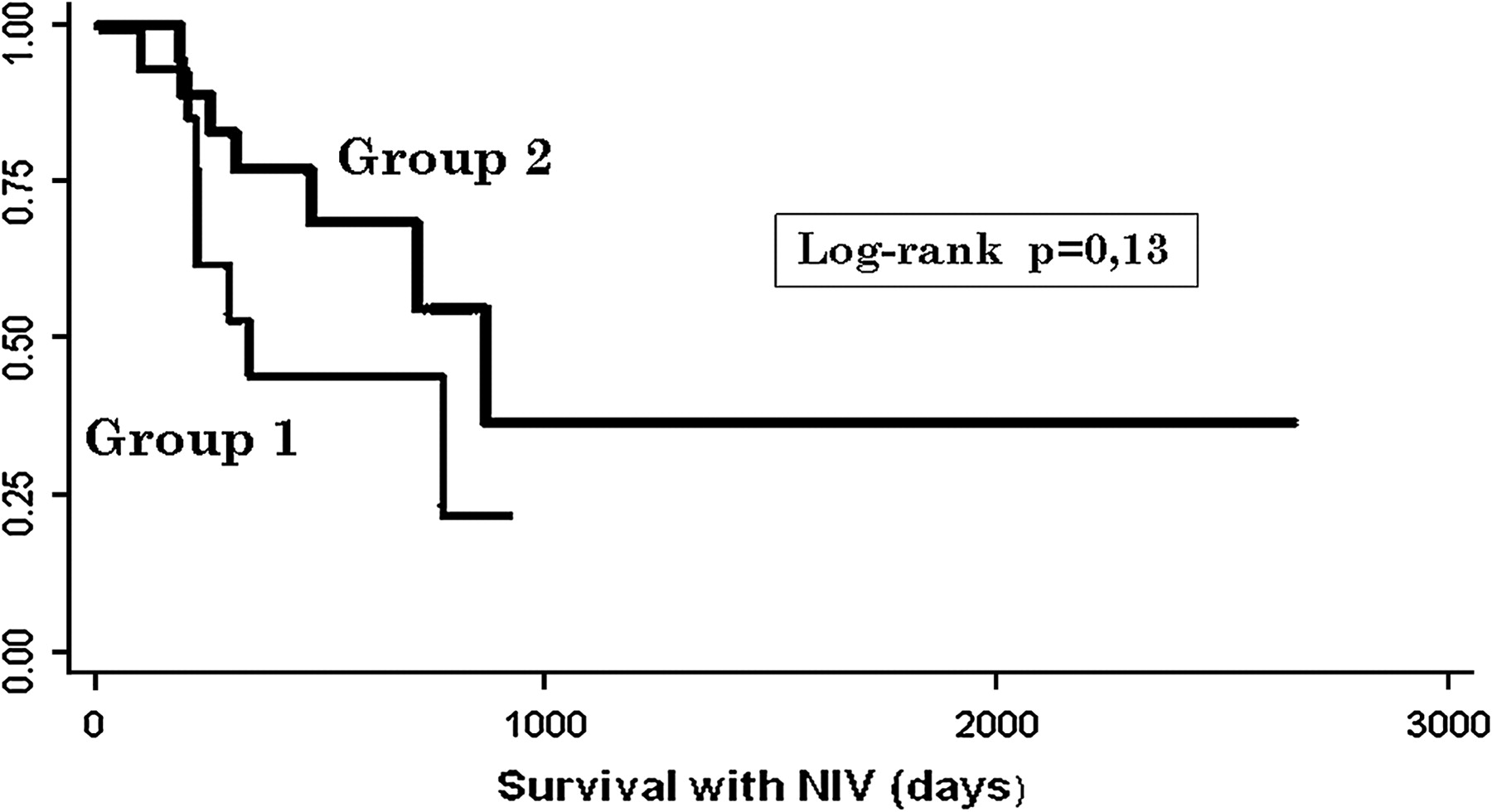
For survival evaluation, at the end of the study, 12 patients were still alive in each group and differences did not reach statistical significance at the 5% level. However, patients in G2 tended to have a longer survival (table 5, figure 2).
Survival analysis
{kind=link}
{kind=link}
Kaplan–Meier survival curves. Group 1 included 20 patients whose compliance with non-invasive ventilation (NIV) was office based. Group 2 included 19 patients to whom a remote control of their equipments was offered. At the end of the study 12 patients were alive in each group.
Discussion
ALS is a devastating neurological condition with a low incidence of 2–4/100 000 inhabitants, a short survival and low prevalence of 5–7/100 000, according to different epidemiological studies.29 The relatively small number of patients supports some difficulties in the randomisation of patients based on computer generation in a single centre in our country. Thus the present study is a prospective single blinded quasi randomised clinical trial that included consecutive patients, aimed at testing the feasibility, efficacy and efficiency of telemedicine for home monitoring NIV. In addition, patient selection based on geographical residence was not considered biased and was probably appropriate for our purpose.
The feasibility of telemedicine for home monitoring patients with chronic respiratory failure discharged from hospital with a mean follow-up time of 176 days has been assessed and it was found that home monitoring was feasible and useful for titration of ventilation settings.30
To the best of our knowledge, the present study is the first trial of NIV compliance using a new technical method that enabled us to monitor remotely registered data in the equipment software.
Before the present trial, in the run-in period, we had an exploratory phase to test safety, acceptance and accuracy. The system was suitable, worked well and served our investigational purposes. The main limitations were related to the need for a fixed telephone line and speed of data extraction.
Our study supports the role and use of telemonitoring in eliminating difficulties imposed by geographical distances and lack of resources. We observed objective gains in terms of healthcare utilisation (table 3), reflecting the efficiency of the system.
Cost analysis is underway but our preliminary data indicate significant cost reduction using telemonitoring (approximately 50%), as expected from the lower number of hospital visits and admissions. Therefore, in view of the limited resources of health systems,31 32 this study strongly supports the fact that frequent virtual visits to the patients by modem communications may become current practice, as an alternative to the office based control of compliance to NIV.
Indeed, the control of compliance is a critical issue because, despite recommendations, the rate of NIV use is poor and highly variable (range 0–70%) in European and American ALS centres. Chiò et al showed that the use of NIV ranged from 50% to 70% depending on the size of the ALS clinics. More recently, Jackson reported 36% use in ALS patients with FVC lower than 50% of the predicted value, and correlated tolerance with respiratory symptoms. Other factors such as age, race, type of insurance, forced vital capacity, disease duration, ALSFRS, caregiver burden or quality of life were not predictors of compliance.17 33–36
Other factors may influence the possible relationship of compliance to settings of the ventilators. The possible role of setting changes through modem communications in increasing compliance was not confirmed in the present study, probably due to the identical procedures that took place in both groups, all performed by one of the authors (AP), or the small sample size. However, our results showed a trend towards a greater number of hours of NIV use in G2, suggesting a marginal effect on compliance. Probably associated with this marginal effect, we observed a trend towards survival benefit (p=0.17) in G2 (table 5).
In addition, in G2 we were able to show a 50% reduction in the number of parameter setting changes during the survival period with NIV, but a 20% increase during the DTC period (exact Poisson p<0.001). This result represents a tighter follow-up during the initial period of NIV adaptation, thus driving a reduction in the total time needed to adjust settings over the whole period of ventilation.
Regarding the functional and survival outcome measures, median survival with NIV was 334 days in G1 versus 865 days in G2 (p=0.13). Considering survival from symptom onset, the benefit in median survival time was >1500 days (figure 2). Further calculations of the sample needed to achieve 90% statistical power indicated that 40 patients in each arm would be needed to show a significant survival impact.
Moreover, a trend was also observed towards improved functional outcomes in G2 patients in terms of the ALSFRS spinal subscore (p=0.15). This was not anticipated, as ALS patients in G1 had a closer follow-up provided by physiotherapy in our specialised centre. Exercise was suggested to all patients, included to the limits of perceived fatigue (Borg scale), simultaneously with NIV if needed,14 but patients in G1 were supervised by physiotherapists with special training in ALS. We hypothesised that timed and adequate intervention due to early detection of alert signs might allow patients to perform more daily physical activities. Ventilation subtleties may be not fully understood without quantifying measurements related to lung mechanics, meaning that clinical judgement may not be sensitive enough to early detect deviations from a ventilation profile otherwise detected by the regular observation of the night calendar. The increased speed of these communications with faster data transmission and improved alarm signs would certainly reassure patients, caregivers and physicians, with benefits to all.37
Whether our positive results are related to closer vigilance and faster correction of respiratory changes or to other undisclosed factors remains to be clarified. Future studies should evaluate the impact of telemonitoring on the quality of life of patients and caregivers.
Acknowledgments
The authors are grateful to Linde Sogas Co for technical support.
References
Footnotes
Linked articles 212720.
Funding This work was supported by ‘Fundação para a Ciência e Tecnologia’—PIC/IC/82765/2007.
Competing interests None.
Ethics approval The study was approved by the local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.