





Abstract
Tuberculosis (TB) is considered to be a disease of poverty, since its incidence is exacerbated by socioeconomic factors, inconsistent or partial treatment practices, and immigration from endemic countries.
A prospective country level study, using a comprehensive dataset of TB incidence and prevalence taken from countries within the World Health Organization (WHO) European region, was conducted. We employed quintile regression to investigate the prospective association between baseline (measured in 2000) and a nation’s wealth, level of egalitarianism, migration rate, health-related lifestyle and social capital with TB incidence and prevalence over a 10-yr period (2000–2009).
We found that ∼50% of TB variation is accounted for by a nation's wealth and level of egalitarianism. We observed a negative prospective association between logged gross domestic product and TB rates, and a positive prospective association between income inequality and TB.
National income levels per capita and income inequality are important predictors for TB incidence and prevalence in the WHO European region. They account for 50% of country-level variation, indicating the importance of a combined absolute and relative socioeconomic disadvantage in the development of TB. These findings also provide a tool for forecasting potential fluctuations in the level of TB epidemics in the WHO European region, with respect to socioeconomic changes.
In Europe, where all countries are past the epidemiological transition [1], the majority of deaths (86%) are attributed to chronic disease, with the shift in mortality rates from infectious disease to chronic disease occurring due to the successful control of communicable disease [2]. However, substantial inequalities or disparities in the health of different socioeconomic groups remain. Mortality and morbidity rates differ systematically by socioeconomic status throughout Europe; higher education, income, and social class are associated with a healthier lifestyle and a longer life expectancy [3–5]. With respect to communicable diseases, a systematic review on socioeconomic factors and infectious diseases in Europe highlighted the presence of differentials and attributed these to low levels of education, low occupational class, or low income level [6], as well as a high-risk health-related behaviour, which has also been linked to a low socioeconomic position [7].
Among communicable diseases, tuberculosis (TB) remains a global emergency. In 2009 TB was responsible for an estimated 1.9 million deaths worldwide with a further 9.4 million reported new cases of TB [8]. TB is considered to be a disease of the socially and economically disadvantaged, since its incidence is exacerbated by socioeconomic factors, inconsistent or partial treatment practices and immigration from countries in which the disease is endemic [6, 9, 10]. Reducing inequalities in TB incidence in Europe is, therefore, a goal that needs to be addressed, especially since the recent global financial crisis is expected to exacerbate health inequalities [11, 12]. However, the relatively small contribution of TB to overall mortality and morbidity makes the statistical analysis not feasible on the individual level and an ecological study is needed. Macro-level variation and especially country-level differences provide us with an excellent opportunity to study the effect of social determinants on TB incidence and prevalence in Europe. In general, national differences in health indices may be valuable in providing insights into macro-level determinants of health, including structural and policy influences [13]. Further study might show which macro-level factors are most influential and maybe identify those that could be modified through intervention. Country-level health differences in Europe have been widely reported and the presence of country-level variation is consistent, despite the various health outcomes that have been used [4, 14–17], and Country-level health differences have also been reported with respect to TB prevalence [18]. Several explanations for the observed country-level variation have been suggested: a leading explanation concerns economic growth and development, which are viewed as important predictors of population health. In accordance with this hypothesis, gross domestic product (GDP) per capita has been consistently linked with population health [19], with wealthier countries in general having a better population health. Furthermore, income inequality, which is prevalent to varying degrees in all European countries, is thought to influence country-level variation, with several studies reporting an association between the Gini coefficient and population health [20]. Consistent with the lifestyle explanation of health inequalities, differences in health-related lifestyles have been found across Europe [21], and these are thought to be contributing to health differences between countries. Finally, from a psychosocial perspective, social capital and its dimensions, such as social trust and social participation, have been suggested as important predictors for country-level variation in health [22]. To this explanatory framework we added net migration rates for each country, since, to a certain extent, immigration in Europe originates from countries where TB is endemic [23, 24].
Motivated by finding that European countries present a highly heterogeneous situation in terms of TB epidemiology and control [25], our major aim in this macro-level ecological study is to investigate the concurrent and prospective effect of country-level social determinants on the prevalence and incidence of TB in 55 countries of the World Health Organization European region, using a comprehensive country-level dataset spanning 10 yrs (2000–2009).
METHODS
Data sources and measures
In table 1 we present the descriptive statistics and sources of information for all variables in the model. With respect to the predictors at baseline (2000), we employed an indicator of the prevalence of smoking as a proxy measure of health-related lifestyle, since there is a well-known association between smoking and TB outcome [31]. The Gini coefficient was employed as a measure of income inequality; it is the most commonly used measure of inequality and varies between 0, which reflects complete equality and 1, which indicates complete inequality [20, 32, 33]. Logged GDP per capita was used as a measure for the standard of living, whereas a social trust index was used as an indicator of social capital. In our models we included countries with complete information on all predictors as well as the two outcomes (n=42).
Statistical modelling
Once the appropriate indicators were derived we employed appropriate quintile regression models to obtain the adjusted for other country-level predictor effect of education, wealth distribution and other indicators of social inequalities on TB rates. In ecological studies, where country-level aggregated data is used, the distributional assumptions of linear regression rarely hold. Therefore, quintile regression offers an attractive alternative that relaxes such assumptions since no parametric distributional form is assumed for the error distribution and, therefore, can be used with skewed distributions since the median of the dependent variable instead of the mean is modelled. All models were estimated with STATA statistical software package (version 11.1; STATA Corporation, College Station, TX, USA).
RESULTS
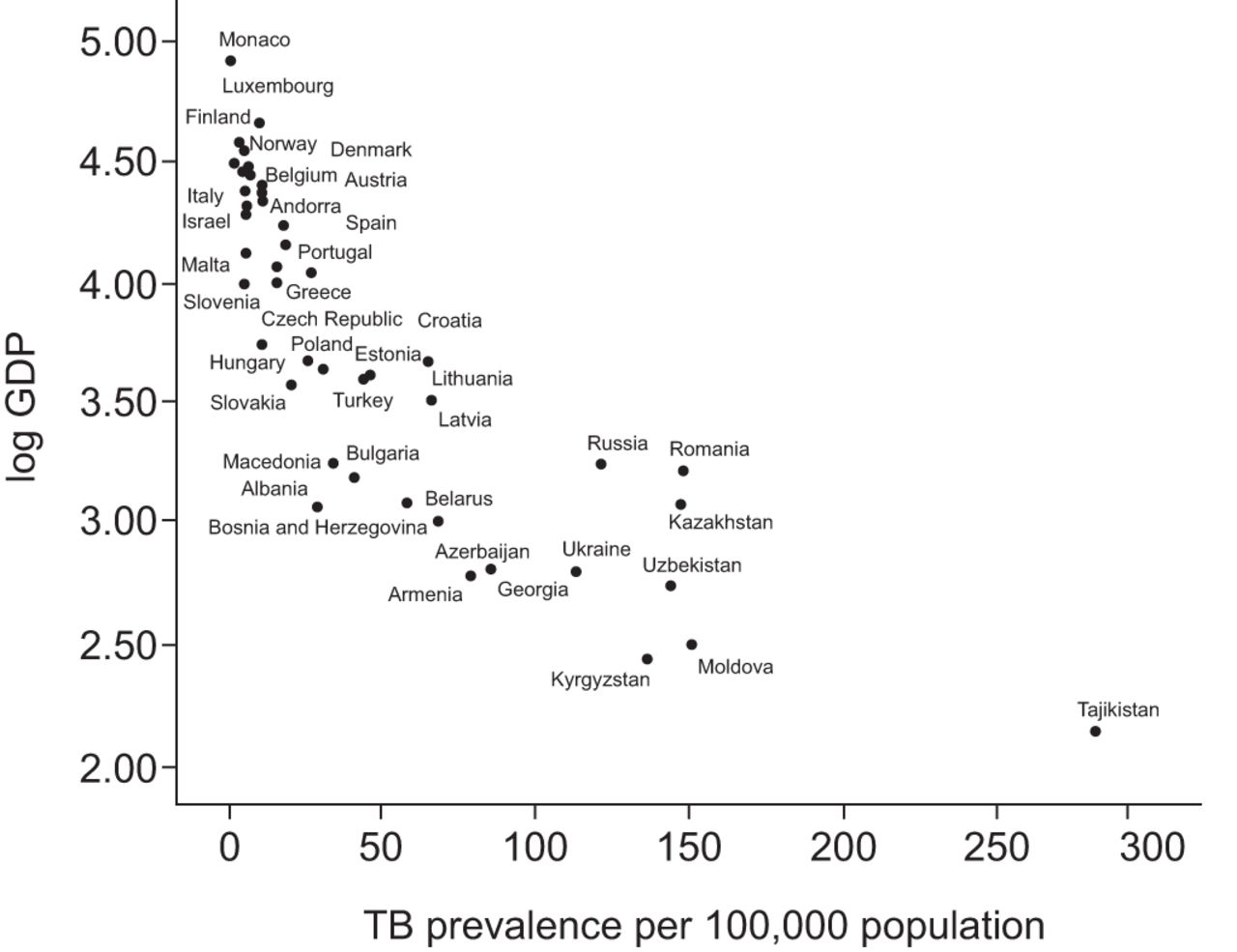
There is considerable country-level variation with respect to TB incidence (1.7–225 per 100,000) and prevalence (2.8–382 per 100,000) in Europe (table 1). In table 2 we present quintile regression parameter estimates, their respective confidence intervals, p-values derived from bootstrapped standard errors (10,000 replications) and pseudo R2 for each model. Our models accounted for ∼50% of the variation in both outcomes either at baseline or prospectively (pseudo R2 for each yr presented in table 2). Logged GDP per capita measured at baseline (2000) was negatively associated with the prevalence and incidence of TB, indicating both cross- sectional and prospectively that countries with higher GDP per capita have lower TB incidence and prevalence (table 2 and fig. 1). On the contrary, income inequality as approximated by the Gini coefficient measured at baseline was negatively associated with TB incidence, both concurrently and also prospectively. We observed a lagged effect of income inequality on TB prevalence, since the Gini coefficient measured at baseline had a prospective negative association with TB prevalence (3 yrs after baseline). This was an expected finding since the influence of inequality on incidence from the baseline onwards would eventually be expressed on the association between income inequality and TB prevalence (table 2 and fig 2). We did not observe any significant association between the remaining three predictors, net migration, social trust, and smoking with either incidence or prevalence of TB.

Scatter plot of the association between the baseline (2000) logged gross domestic product (GDP) and tuberculosis (TB) prevalence in 2005.

{kind=link}
{kind=link}
Scatter plot of the association between baseline Gini coefficient 2000 and tuberculosis (TB) incidence in 2004.
DISCUSSION
There is a large heterogeneity in TB prevalence and incidence in the WHO Europe region, a finding in accordance with previous studies [25]. We found that ∼50% of this variation is due to a nation's wealth and level of economic development, but it is also driven by the income distribution within nations, indicating that both absolute and relative socioeconomic disadvantage are influential in the development of TB. We observed a strong negative association between GDP and both TB outcomes, a finding in accordance with previous research on TB [18, 34] and other health outcomes [15], but not in line with previous studies where a non-linear association between GDP and health was suggested, with diminishing marginal effects of economic development once a certain standard of living had been achieved [35]. It appears that as a country grows wealthier it has more resources to spend on health-promoting social programmes, such as public sanitation, potable water, and health awareness initiatives. Furthermore, individuals are able to purchase healthier food, improved housing, live in safer environments and have better access to healthcare [36, 37] compared with their counterparts in poorer countries, as a result aggregated TB rates and other population health statistics are improved.
Income inequality was a significant predictor of country-level variation in TB rates, with less inequality being associated with lower incidence and prevalence. The finding that country-level variation in health is largely associated with differences in the level of egalitarianism of each country, as measured by the Gini coefficient, is in accordance with some previous findings [20, 38], but not with others [38–41]. However, these studies had a global, rather than European, focus [35]. It appears that in the European countries considered here, more unequal distribution of income leads to a larger proportion of individuals with incomes less than the minimum required for healthy living [42, 43], or below the poverty line. Thus, despite the overall wealth and level of economic development within a nation, income inequality increases the numbers of individuals within a country that have low vaccine coverage, engage in high-risk health behaviour, and have limited access to healthcare. These are all factors which are relevant for or correlate with the incidence and prevalence of TB. Another potential explanation of the effect of income inequality on TB is that income inequality results in increased urban poverty, which is associated with well-known risk factors for TB, such as overcrowding and polluted environments [44].
We did not observe an association between migration and smoking with either TB incidence or prevalence, despite the fact that both predictors are thought to be associated with TB outcomes [23, 45]. We speculate that any potential effect of the two predictors is being picked up by income inequality; since immigrants from countries where TB is endemic are more likely to be disadvantaged with respect to income and the same can be argued for smokers. To further elucidate this issue we conducted sensitivity analysis replacing net migration in our models with available information on the proportion of TB cases that were foreign born (2007 and 2009). Similarly with net migration, the proportion of foreign born TB cases was not associated with overall TB incidence or prevalence. Income inequality remained a strong predictor of both TB incidence and prevalence, supporting our speculation that the effect of net migration on TB is being picked up by income inequality. On the contrary, the effect of GDP became nonsignificant, a finding due to the tendency of affluent countries to receive a relatively high number of migrants from countries where TB is endemic [46]; this idea is supported by the high correlations (r>0.8) between GDP and the proportion of foreign born TB cases (unpublished data).
We did not observe an association between social trust and country-level variation in TB, a finding in agreement with some previous studies [15, 47]. Although it has been suggested elsewhere that income inequality leads to more violence, less social cohesion and lower levels of social trust [20], it appears that the mechanism, through which income inequality influences TB outcomes, is not related to social trust. Considering that differences in social capital that have been reported in Europe [48, 49], an explanation for the lack of association between social trust and TB may be that social capital dimensions do not have, perhaps as yet, any theoretical links to TB and other infectious diseases, but are mostly relevant to chronic diseases, which have known links to negative psychosocial processes according to the social stress hypothesis [50].
The major limitation of this study is the reliance on ecological, country-level data, which is subject to well-known ecological fallacy. In other words, we cannot be certain that the aggregate effects we have found apply to the population at the individual level. Furthermore, our statistical analysis was carried out using countries with complete data. We estimated several multiple, imputation models for sensitivity purposes in order to increase the analytic sample (unpublished data). The results of these models were similar with the one we present here, suggesting that the exclusion of missing data in our statistical analysis did not bias our results.
Conclusion
This study is based on the comprehensive prospective dataset of country-level predictors of TB rates and the use of appropriate models to quantify their association. However, despite the strong predictive associations between logged GDP, the Gini coefficient and the two TB outcomes, our models accounted for ∼50% of the country-level variation in TB rates and it is plausible that unmeasured confounders may have biased our estimates. Further research is needed to identify these country-level predictors that account for the remaining variance, for example it has been proposed that characteristics of the welfare states, such as social benefits and generally high social expenditure, are related to improved population health [51] and this may be relevant to TB rates in the European and neighbouring countries, considered here. Finally, regardless of these uncertainties, the findings suggest that measures of wealth, inequality and the magnitude in their variation at regional and national level could be used to forecast changes in TB epidemics when facing socioeconomic changes at the European and global level.
Footnotes
Statement of Interest
None declared.
- Received October 21, 2011.
- Accepted December 14, 2011.
- ©ERS 2012
REFERENCES










