





Abstract
The present study describes a case of pulmonary arterial hypertension (PAH) associated with multicentric Castleman's disease in a patient infected with HIV type 1 and human herpes virus 8.
Therapy included highly active antiretroviral therapy, warfarin, diuretics, continuous i.v. epoprostenol and 12-monthly pulses of cyclophosphamide.
The patient's condition improved dramatically with complete reversibility of PAH, allowing weaning of continuous i.v. epoprostenol therapy. After 5 yrs, both Castleman's disease and PAH have not relapsed. This supports the hypothesis that control of inflammation and retroviral replication may be of interest in the context of PAH, complicating the course of an inflammatory condition associated with viral infection.
In conclusion, further studies should help in characterising the best candidates for anti-inflammatory treatment in the setting of pulmonary arterial hypertension.
Pulmonary arterial hypertension (PAH) is a rare condition characterised by elevated pulmonary arterial resistance leading to right heart failure and death 1. PAH can be sporadic, familial or related to other conditions, including connective tissue disease, congenital systemic-to-pulmonary shunts, portal hypertension, HIV infection and appetite suppressant exposure 2. Treatment of PAH allows improved survival, although current therapies do not achieve a cure for this devastating disease 3. Complete reversibility of PAH has been exceptionally reported, mostly in the setting of active autoimmune diseases, such as systemic lupus erythematosus treated with corticosteroids and/or immunosuppressive agents 4.
Castleman's disease is a rare clinical-pathological entity, belonging to the lymphoproliferative disorders and responsible for lymph node enlargement 5, 6. It can be classified into two forms: localised and multicentric. Localised disease is generally asymptomatic or presents as an isolated enlarged lymph node. Multicentric Castleman's disease often results in diffuse lymphadenopathy, frequently associated with hepatosplenomegaly and systemic manifestations (asthenia, weight loss and fever). Castleman's disease is defined by lymphocytic angiofollicular hyperplasia usually associated with polyclonal lymphocytic proliferation. There are no specific biological markers of Castleman's disease. However, in the multicentric forms, an elevation of the sedimentation rate, anaemia, thrombopenia and polyclonal hypergammaglobulinaemia can be observed 5, 6. Multicentric Castleman's disease has been associated with HIV infection 7. The treatment of choice of localised forms is complete surgical resection with a strong possibility of cure without relapse. In multicentric forms there is no current therapeutic consensus, but most authors recommend chemotherapy. The prognosis of the multicentric forms is less favourable, with a cure in only 20% of cases 5, 6.
Only two cases of PAH and Castleman's disease have previously been reported in HIV sero-negative patients 8. In the present report, an additional case of severe PAH and multicentric Castleman's disease in an HIV-infected patient is described. The clinical course of this patient was remarkable with complete PAH reversibility with medical treatments, which included highly active antiretroviral agents, 12 cyclophosphamide i.v. pulses and transient continuous i.v. epoprostenol.
CASE REPORT
A 31-yr-old female was admitted to the intensive care unit (Hôpital Antoine-Béclère, Assistance Publique Hôpitaux de Paris, France) in September 1997 after an episode of syncope. She was known to have had HIV-1 infection since 1988, presumably contracted after a blood transfusion. The patient did not have any history of opportunistic infections and had not received any antiretroviral treatment.
The electrocardiogram at admission showed sinus tachycardia, right ventricular hypertrophy and incomplete right bundle branch block. A chest radiograph demonstrated cardiac hypertrophy and enlarged pulmonary arteries. Echocardiography detected elevated systolic pulmonary arterial pressure (Ppa) of 11.97 kPa (90 mmHg) and a paradoxal motion of the interventricular septum. Clinical examination revealed dyspnoea of functional class III of the New York Heart Association (NYHA), signs of right-heart failure and diffuse lymphadenopathy.
High-resolution computed tomography of the chest revealed enlarged pulmonary arteries and cardiomegaly without enlargement of the thoracic lymph nodes. A ventilation and perfusion lung scan was normal, ruling out a possible diagnosis of pulmonary thrombo-embolic disease. Right-heart catheterisation established the diagnosis of severe PAH with a mean Ppa of 8.51 kPa (64 mmHg), pulmonary artery wedge pressure of 1.06 kPa (8 mmHg) and a decreased cardiac index (2.4 L·min−1·m−2; table 1⇓; fig. 1⇓). An acute vasodilatator challenge was negative (0% change in mean Ppa and 1% increase in pulmonary vascular resistance after a 10-min inhalation of 10 ppm nitric oxide through a face mask). The 6-min walk distance (6MWD) was 295 m.

{kind=link}
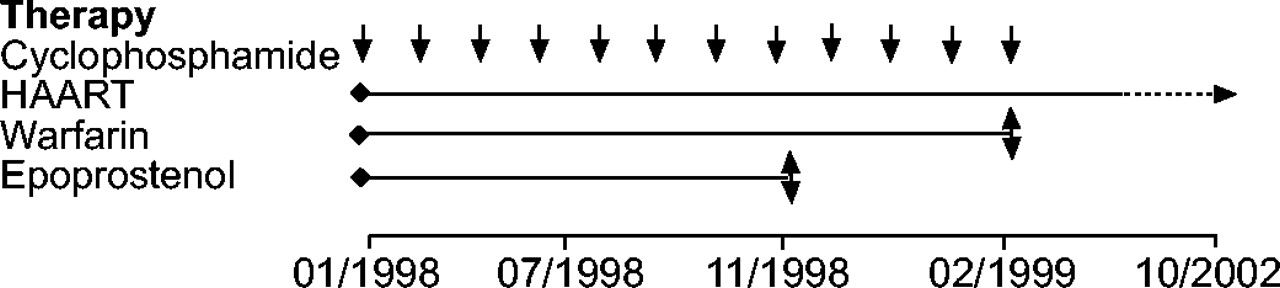
Treatment of a 31-yr-old HIV-positive patient with severe pulmonary arterial hypertension and Castleman's disease. Therapy included 12-monthly cyclophosphamide pulses, highly active antiretroviral therapy (HAART), warfarin and continuous i.v. epoprostenol.
Haemodynamic parameters and functional status of a 31-yr-old HIV-positive patient with severe pulmonary arterial hypertension and Castleman's disease
Biological analysis found a polyclonal hypergammaglobulinaemia (91.4 g·L−1). CD4 lymphocyte count was 640 mm−3 and HIV-1 viral load was 4.9 log10 copies·mL−1. Abdominal ultrasound revealed hepatomegaly and renal cortico-medullary de-differentiation. Hepatic and renal biopsies showed plasmocyte infiltrates and renal arterial hyalinosis. The association of diffuse lymphadenopathy, polyclonal hypergammaglobulinaemia and plasmocytic infiltrates established the diagnosis of a multicentric Castleman's disease in an HIV patient, with severe PAH. Human herpes virus 8 (HHV8) serology was positive using a lytic immunoflurescence assay (HHV8 immunoglobulin G IFA; Biotrin, Dublin, Ireland).
Therapy included highly active antiretroviral therapy (initially AZT, 3TC, saquinavir, ritonavir, allowing full control of viral replication within 3 months), warfarin, diuretics, continuous i.v. epoprostenol and specific treatment of Castleman's disease, consisting of monthly i.v. pulses of 600 mg·m−2 cyclophosphamide. After 3 months of therapy, the patient improved dramatically (NYHA functional class II and 6MWD of 440 m). At 6 months, the patient's condition had clinically and haemodynamically normalised (NYHA functional class I, 6MWD of 490 m, mean Ppa of 2.52 kPa (19 mmHg) with a normal cardiac index of 3.40 L·min−1·m−2; fig. 1⇑). After 10 months, the haemodynamic and clinical parameters were still stable, and epoprostenol was gradually weaned. A further 6 months later, the haemodynamic parameters remained stable (fig. 1⇑). After 12 pulses of cyclophosphamide, the patient presented with complete remission of Castleman's disease and normal myelogram. Thus, cyclophosphamide therapy was discontinued. At present, 5 yrs after epoprostenol weaning, the patient is still asymptomatic and both Castleman's disease and PAH have not relapsed. Control echocardiography shows a stable systolic Ppa of 4.65 kPa (35 mmHg) with a normal right-heart morphology.
DISCUSSION
Two cases of PAH in patients with multicentric Castleman's disease have previously been reported in the literature 8. Both cases tested negative for HIV. The first patient presented with severe PAH and multicentric disease, but died of right-heart failure despite continuous i.v. prostacyclin therapy and complete remission of Castleman's disease. PAH improved in the second patient with dual endothelin receptor antagonist bosentan, without complete remission of the Castleman's disease. The patient in the present study is remarkable for two reasons: 1) this is the first case of PAH related to HIV infection in a patient with multicentric Castleman's disease; and 2) this patient had completely normalised pulmonary haemodynamics after treatment, including highly active antiretroviral agents, 12 cyclophosphamide i.v. pulses and transient continuous i.v. epoprostenol.
PAH and Castleman's disease are two rare conditions. Previous case reports in three patients raise several hypotheses linking these diseases. In Castleman's disease, interleukin (IL)-6, a multifunctional pro-inflammatory cytokine, is produced in large quantities in the germinal centres of hyperplastic lymph nodes 9. Clinical manifestations of Castleman's disease are closely related to serum levels of IL-6, and IL-6 overproduction could explain hypergammaglobulinaemia and increased serum levels of acute phase proteins 9. Indeed, systemic manifestations of multicentric Castleman's disease and its biological markers of inflammation can be alleviated after anti-IL-6 receptor antibody therapy 10, 11. IL-6 may also play a role in angiogenesis and could play a role in human, as well as experimental models of pulmonary hypertension 10, 12, 13. These facts raise the possibility of IL-6 being a common pathogenic factor in both PAH and Castleman's disease.
In addition, a viral link could explain why both conditions may coexist. Indeed, HIV and HHV8 have been reported to be involved in the pathophysiology of PAH and Castleman's disease. HHV8 is a vasculotrope virus associated with Kaposi's sarcoma and lymphoproliferative disease, including HIV-associated Castleman's disease and primary effusion lymphoma. HHV8 encodes genes homologous to human genes involved in cell proliferation, anti-apoptosis and angiogenesis. Viral genes, such as v-Cyclin or LANA-1 induce transcription of cell cycle genes via interaction with retinoblastom protein freeing a gene regulation protein, E2F 14, 15. Furthermore, HHV8 genes are able to block apoptosis by inhibition of p53-induced apoptosis (LANA-1) 16, inhibition of Fas-induced apoptosis (v-FLIP) 17 or inhibition of bax-mediated virally induced apoptosis (v-bcl2) 18.
In multicentric Castleman's disease, genetic sequences of HHV8 have been detected in >60% of HIV-infected patients and in 20–40% of HIV sero-negative cases 19. Moreover, a strong correlation between HHV8 viral load and clinical symptoms, as well as elevated C-reactive protein and plasma IL-6 concentrations, was shown in multicentric Castleman's disease occurring in HIV-infected patients 20. In PAH, HHV8 antigen and gene sequences have been found in plexiform lesions raising the possibility that HHV8 could be involved in the misguided angiogenesis characteristic of the disease 21. Indeed, it has recently been demonstrated that HHV8 is able to produce a viral homologue of IL-6 which shares many biological activities of human IL-6 and promotes angiogenesis by inducing vascular endothelial growth factor (VEGF) expression 22–24. Interestingly, VEGF has also been involved in the pathobiology of PAH 25, 26. However, recent analyses on plasma samples and lung tissues of patients with PAH do not plead in favour of an association between PAH and HHV8 27–30. Thus, additional information is still necessary to establish the true link between HHV8 infection and PAH.
The present study shows an unusual complete reversibility of both multicentric Castleman's disease and severe PAH, with a treatment regiment including a potent immunosuppressive agent (cyclophosphamide), together with highly active antiretroviral therapy and continuous i.v. epoprostenol. The respective role of each of these therapies in this unusual patient outcome needs to be discussed further. First, epoprostenol improves haemodynamics and exercise capacity in PAH 3. However, haemodynamic and clinical improvements are far from complete. PAH reversibility leading to weaning of vasodilator therapy has not been reported in large cohorts of PAH patients, including idiopathic PAH and PAH related to HIV infection 31–34. Therefore, it is recommended that PAH patients in NYHA functional class III or IV should receive life-long vasodilator therapy 3. Secondly, highly active antiretroviral therapy may result in significant clinical and haemodynamic effects in PAH related to HIV infection 33, 34. However, these positive results are not sufficient to reverse this severe condition and it is recognised that NYHA functional class III or IV patients with PAH related to HIV should receive combined vasodilator therapy and highly active antiretroviral therapy 3, 33, 35. Finally, inflammatory mechanisms appear to play a significant role in PAH of various origins in humans, such as systemic lupus erythematosus, mixed connective tissue disease, HIV infection or plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein and skin changes (POEMS syndrome) 36. Interestingly, some patients with severe PAH associated with systemic lupus erythematosus and POEMS syndrome have experienced significant improvements with corticosteroids or immunosuppressive therapy, emphasising the relevance of inflammation in a subset of patients presenting with PAH 4, 37. The present study supports the hypothesis that control of inflammation and retroviral replication may be of interest in the context of PAH, complicating the course of an inflammatory condition associated with HIV infection.
In conclusion, further studies should help in characterising the best candidates for anti-inflammatory treatment in the setting of pulmonary arterial hypertension.
- Received November 23, 2004.
- Accepted April 26, 2005.
- © ERS Journals Ltd
References









