


Novel Mechanism for Prolonged Retention of Topically Applied Steroid in Airway Tissue
Abstract
A high airway concentration might be required for the antiasthmatic efficacy of inhaled glucocorticosteroids (GCS). The topical uptake and retention of GCS in airway tissue were compared for GCS of the inhaled type [budesonide (BUD), fluticasone propionate (FP), and beclomethasone dipropionate (BDP)] and of the noninhaled type (dexamethasone and hydrocortisone). 3H-labeled GCS solutions were administered into rat airways by either perfusion of trachea in vivo, intratracheal instillation, or inhalation. Radioactivity was determined in the airway tissue, lung parenchyma, and plasma 20 min to 24 hr after exposure. Ethanol extracts of exposed tracheas were analyzed by HPLC. Exposed tracheas were also incubatedin vitro in buffer, and the released radioactivity was analyzed by HPLC. BUD, FP, and BDP were equally well taken up into the airway tissue; their uptake was 25–130 times greater than that of dexamethasone and hydrocortisone. BUD was shown to form very lipophilic intracellular fatty acid esters (at carbon 21) in the airway and lung tissue after topical application. In large airways 20 min after administration, approximately 70–80% of retained BUD was conjugated. BUD stored in esterified form in the tissue was retained in large airways for a prolonged time, compared with FP and BDP, which do not form such conjugates. The fatty acid conjugation of BUD is reversiblein vivo; BUD conjugates are gradually hydrolyzed and free BUD is regenerated. This reversible conjugation may improve airway selectivity, as well as prolong the local anti-inflammatory action of BUD in the airways and might be one explanation for why BUD is efficacious in the treatment of mild asthma when inhaled once daily.
GCS1used in asthma therapy are today primarily administered by inhalation, with the aim of achieving high local concentrations in the airway mucosa and limiting the increase of steroid concentrations in the rest of the body. The inhaled GCS can also ameliorate bronchial hyperresponsiveness, which is much less affected by oral GCS therapy (Jenkins and Woolcock, 1988). It seems that, in addition to high receptor affinity and high first-pass liver and gut inactivation, prolonged high local concentrations in the airways are necessary for the high antiasthmatic efficacy and airway selectivity of inhaled GCS (Brattsand, 1989).
GCS receptor affinity and the preferential inactivation of inhaled GCS by liver metabolism have been studied extensively (Barnes and Pedersen, 1993). In contrast, there are few kinetic data on peak tissue levels and retention of topically applied GCS in the airway and lung tissue (Van den Bosch et al., 1993; Esmailpour et al., 1997). We reported earlier (Miller-Larsson et al., 1994) a prolonged retention of BUD in rat airway tissue in vivo, compared with FP and BDP. These findings seemed to contradict the general positive correlation between the lipophilicity of the GCS and their tissue binding ability, because BUD is less lipophilic than FP and BDP.
In the present study, the prolonged dwell-time of BUD in airway tissue has been confirmed and explained in mechanistic terms. Radiolabeled GCS, at clinically relevant doses, were administered in vivoto rat airways by various methods. In addition, the release of GCS from the exposed airway tissue into the surrounding fluid in vitro was investigated. GCS of the inhaled type (BUD, FP, and BDP), as well as systemic GCS lacking airway efficacy (HC) or airway selectivity (DEX), were studied.
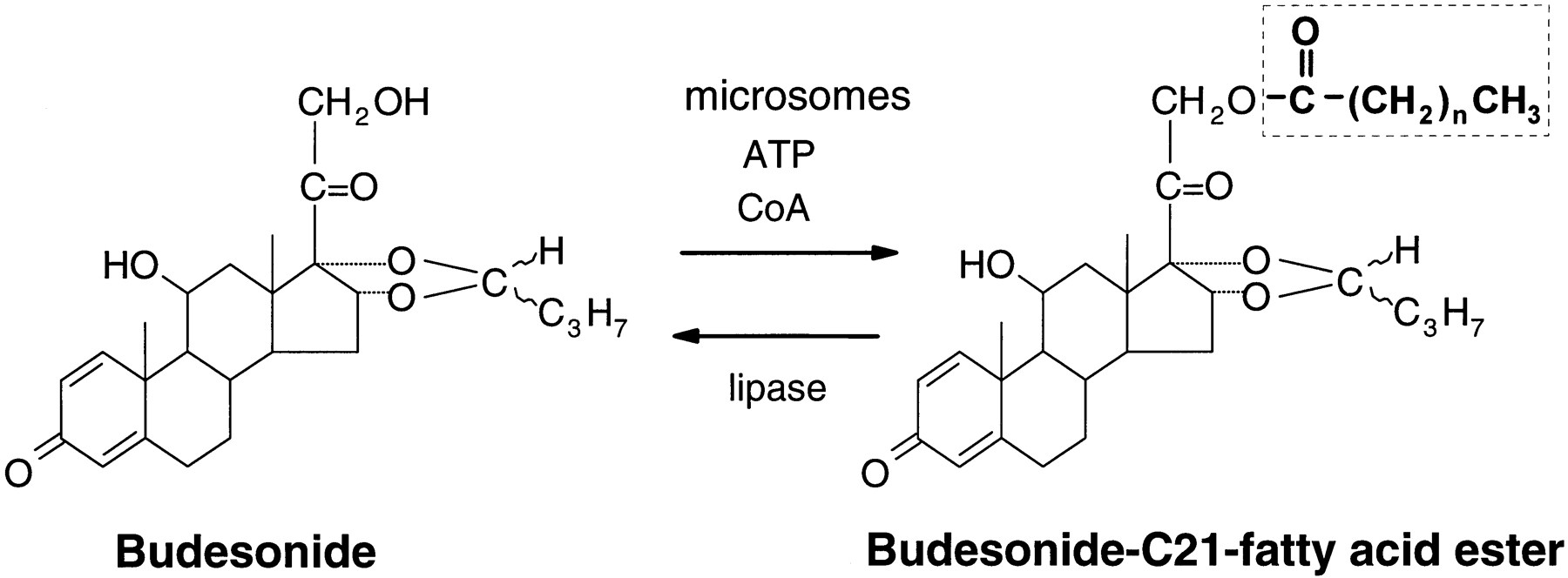
We report here that BUD is conjugated extensively with fatty acids within airway tissue and lung in vivo, resulting in the formation of BUD esters at the C21-hydroxyl group. The results are in agreement with the previously reported formation of BUD esters in vitro in human lung and liver microsomes, where oleate, linoleate, palmitate, palmitoleate, and arachidonate esters of BUD were identified (fig. 1) (Tunek et al., 1997). Fatty acid esters were not detected for FP or BDP. Fatty acid esters of BUD are much more lipophilic than FP or BDP, which explains the prolonged retention of BUD in airway tissue, compared with FP and BDP. These new findings describe a novel mechanism for attaining a high topical selectivity and prolonged activity of GCS at airway levels.

Structural formulas of BUD and BUD-21-fatty acid esters.
The conjugation is CoA and ATP dependent, and free BUD is regenerated by lipase-catalyzed hydrolysis [reproduced from Tunek et al. (1997), with permission].
Materials and Methods
Materials.
Male Sprague-Dawley rats were supplied by Møllegaard Breeding Center Ltd. (Skensved, Denmark). Unlabeled BUD was supplied by Astra Draco AB (Lund, Sweden). 3H-labeled GCS (radiochemical purity, >97.0%) were supplied in 99.5% ethanol by Astra Draco AB or by the Radiochemical Center (Amersham, UK). The following3H-GCS were used: [1,2-3H]BUD, [1,2-3H]FP, [1,2-3H]BDP, [1,2,6,7-3H]HC, and [1,2,4-3H]DEX. Specific radioactivity was 80 Ci/mmol for HC and 30–40 Ci/mmol for the other GCS used (1 tritium atom/molecule yields 29.6 Ci/mmol). One batch of BUD with a specific radioactivity of 17 Ci/mmol was also used.
Study Design.
Solutions of 3H-labeled GCS at concentrations between 10−8 and 10−5 M were administered into the rat airways by 1) perfusion of a tracheal segment in vivo, 2) intratracheal instillation, or 3) inhalation. The total radioactivity was measured in tissue and plasma at different times after administration. GCS were extracted from the exposed airways and lungs with ethanol, and the extracts were analyzed by HPLC. The release of GCS from the tracheal segments during incubation in vitro in buffer was studied, and buffer extracts were analyzed by HPLC.
Tracheal Perfusion.
Before administration, 3H-GCS stock solutions were diluted in 0.9% saline solution in glass vials (final concentration of ethanol, 0.1–0.5%). For concentrations of >3 × 10−7 M, ethanol solutions of labeled and unlabeled compounds were prepared and stored at −20°C. Dilution in 0.9% saline solution to the final concentration (0.5% ethanol) was performed before each application. Rats (300–400 g) were anesthetized ip with a mixture of fluanisone/fentanyl (Hypnorm veterinary preparation; Janssen Pharmaceutica, Beerse, Belgium), midazolam (Dormicum; Roche, Basel, Switzerland), and water (1:1:2), at a dose of 3.3 ml/kg. Anesthesia was maintained by im injections of fluanisone/fentanyl and occasional iv administration of the initial mixture. A section of trachea between the larynx and sternum was exposed in vivo and cannulated at both ends with two polyethylene catheters, to allow perfusion (Miller-Larsson and Brattsand, 1990). An additional catheter was inserted into the section of trachea connected to the lungs, to allow spontaneous respiration. For blood sampling and anesthesia, the jugular vein was catheterized. A thermostat and heated pad maintained the rat temperatures at 37.5 ± 0.5°C. 3H-GCS solutions were perfused (0.1 ml/min) for 10 min (t = 0–10 min), followed by continuous perfusion with 0.9% saline solution. All draining perfusate was continuously collected, and its radioactivity was measured. Rats were killed 20, 70, or 120 min after the start of perfusion. The following 3H-GCS were tested: BUD at various concentrations from 7.5 × 10−8 to 3.0 × 10−6 M, FP at 2.0 × 10−8 and 1.5 × 10−7M, BDP at 7.2 × 10−8 M, DEX at 2.8 × 10−6 M, and HC at 3.4 × 10−6 M.
Binding of GCS to Plastic Material.
To calculate the dose reaching the trachea (perfused dose), the binding of GCS to polyethylene inflow catheters was determined in separate experiments in which 3H-GCS solutions were perfused only through the system of inflow catheters. The binding of FP to inflow catheters was 41.2 ± 3.9% (mean ± SD); hence, FP applied at a concentration of 2.0 × 10−8 M reached the trachea at a concentration of 1.2 × 10−8 M. The binding of BDP was 18.9 ± 5.8%, whereas the binding of the other steroids used was below 5%.
Intratracheal Instillation.
Ethanol was removed from 3H-GCS stock solutions by evaporation under a N2 stream, 0.9% saline solution was added to yield the desired concentration, and the solution was sonicated in a glass vial for 1–2 min on ice. Rats (290–410 g) were lightly anesthetized with inhaled enfluran (Efrane; Abbot, Scandinavia AB, Kista, Sweden), which was delivered by vaporizer together with N2O/O2, and were placed in the supine position on a board tilted at 30°, with the head uppermost. A solution of either [3H]BUD (1.4 × 10−5 or 4.8 × 10−7 M) or [3H]FP (1.5 × 10−7 M) was instilled intratracheally, in 250 μl, through a metal cannula mounted on a plastic syringe. The amount of radioactive label remaining in the solution after instillation was used for calculation of the administered dose (therefore, there was no need to monitor the binding of GCS to the plastic material of the syringe). After instillation, rats were kept on the tilted board until they awoke (approximately 30 sec). The rats were killed 20 min, 2 hr, 6 hr, or 24 hr after intratracheal instillation.
Inhalation.
Rats (210–330 g) were anesthetized with inhaled enfluran as for intratracheal instillation and were intubated with an endotracheal tube (PE-200 tubing) connected to an inhalation chamber (Eirefelt et al., 1992). After intubation, rats breathed spontaneously and inhaled 3H-GCS aerosol (table1), together with anesthetic gases (delivered to the chamber at 2.6 liters/min), for 5 min. Rats were killed 20 min, 2 hr, or 6 hr after the start of aerosol exposure.
Concentrations and doses of GCS applied (arithmetic means ± SD)
Generation of GCS Aerosol.
3H-GCS stock solutions were diluted 10-fold in 99.5% ethanol, to the concentrations given in table 1. GCS aerosol was generated from the ethanol solutions with a MA2S nebulizer (flow rate, 4 liters/min; Viasol, Malmö, Sweden) connected to the inhalation chamber (chamber pressure, 0.4 kPa; total chamber flow, 6.6 liters/min). Ethanol evaporated during inhalation, and amorphous particles were deposited on the airway mucosa. To estimate the concentrations of 3H-GCS during exposure, samples were drawn from the exposure chamber, at a flow rate of 0.2 liter/min, through a filter with a pore size of 1 μm (FALP02500 filter; Millipore, Bedford, MA). 3H-GCS were then extracted from the filter with ethanol (99.5%), and radioactivity was measured. The inhaled doses of the 3H-GCS were calculated according to the formula ID =CC × ET × RMV(Dahlbäck and Eirefelt, 1994), where ID is the inhaled dose (in nanomoles), CC is the chamber concentration (in nanomoles per liter), ET is the exposure time (in minutes), and RMV is the respiratory minute volume (in liters per minute) [RMV = 4.19 × 10−3 × (body weight, in grams)0.66] (McMahon et al., 1977).
Tissue and Blood Sampling.
At the end of each experiment, rats were killed by heart puncture after administration of sodium pentobarbital (60 mg/ml Mebumal veterinary preparation; Pherrovet, Malmö, Sweden) iv (0.1 ml) or ip (1 ml). Blood from the right ventricle was collected, and plasma was separated after centrifugation. After intratracheal instillation and inhalation, the lung vascular system was perfused with two 60-ml aliquots of heparinized (50 IU/ml heparin) 0.9% saline solution, to reduce the impact of the blood contents of the lung. Tissue samples were rinsed briefly in 0.9% saline solution, dried on blotting paper, weighed, and frozen at −70°C.
In Vitro Release of GCS .
Segments of trachea were perfused for 10 min with either [3H]BUD (7.1 × 10−8 M), [3H]FP (1.2 × 10−7M), [3H]BDP (9.9 × 10−8 M), or [3H]HC (7.4 × 10−8 M), followed by perfusion with 0.9% saline solution for the next 10 min. Because FP and BDP markedly bound to inflow catheters, the concentration reaching the trachea was 7.1 × 10−8 M for FP and 8.0 × 10−8 M for BDP (see Binding of GCS to Plastic Material). Immediately after perfusion, the tracheal segments were excised and cut lengthwise into two halves, which were weighed. One half was incubated (37°C) in a glass vessel containing 10 ml of oxygenated (95% O2/5% CO2) standard Krebs buffer with 0.2% glucose and 10% rat plasma (to mimic extracellular fluid). The total radioactivity released into the buffer was monitored for 8 hr; 200-μl samples were withdrawn at various time points, and the volume was replaced with fresh incubation medium. After 8 hr, buffer extracts were analyzed by HPLC. The incubated tracheal segment was combusted in a sample oxidizer for determination of total radioactivity or was extracted with ethanol and analyzed by HPLC. The radioactivity present in the nonincubated segment of trachea was measured after combustion, to ensure that during the incubation procedure there was no loss of steroid resulting from binding to the glass vessels.
Extraction of GCS and Conjugates from Tissue.
The exposed trachea or the lung (with intrapulmonary bronchi) was frozen in liquid nitrogen and pulverized with a mortar. Ethanol (99.5%) was added (1 ml for the tracheal samples and 5 or 10 ml for the lung samples), and the mixtures were shaken for at least 6 hr, followed by centrifugation for 10 min at 8000g. Supernatants were stored at −70°C until HPLC analysis. Combustion of duplicate samples of either trachea or powdered lung (described below) demonstrated conclusively that complete extraction was achieved with this method.
Measurement of Radioactivity.
Tissue samples were weighed, dried overnight at room temperature, and combusted in a sample oxidizer (Packard 307; Packard, Groningen, The Netherlands). Recovery of sample label was >96%. Monophase-S (15 ml) and Ultimagold (10 ml) scintillation cocktails (Packard) were used for oxidized tissue samples and liquid samples, respectively. Radioactivity was measured in a liquid scintillation counter (Packard 460 CD or 300 CD).
The GCS concentration in the samples (picomoles per gram or picomoles per milliliter) was calculated from the following equation:Q = DPM/(C ×SA × W), where Q is the GCS concentration (in picomoles per gram or picomoles per milliliter),DPM is the mean number of disintegrations per minute in the measured sample, C = 2.22 × 106 dpm/μCi, SA is the specific activity of GCS (microcuries per picomoles), and W is the weight (grams) of tissue samples or the volume (milliliters) of plasma. This equation assumes that measured radioactivity represents unchanged GCS; the total radioactivity measured in 1 g of tissue or 1 ml of plasma is converted to the concentration of intact GCS equivalents.
HPLC. Sample Preparation.
Ethanol extracts of trachea and lung and buffer extracts of trachea (incubation buffer from in vitro experiments) were analyzed using two different HPLC systems. Aliquots (1 ml) of the incubation buffer were extracted with 2 × 2 ml of ethyl acetate, with virtually complete extraction of radioactivity. The pooled extracts were evaporated to dryness and redissolved in ethanol.
LC System 1.
Equipment consisted of a 9012 pump, 9010 solvent delivery system, 9100 autosampler, and 9050 variable-wavelength UV/visible detector (all from Varian, Walnut Creek, CA). Mobile phase A was water and mobile phase B was methanol; the gradient was as follows: 0–20 min, 40% A/60% B; at 20 min, stepwise change to 100% B; at 35 min, stepwise change back to the initial conditions. Ethanol extracts were made 60% water/40% ethanol before injection. The flow rate was 1.0 ml/min, and the column was a LiChrosphere® 100 (RP-18) column (125 × 4 mm, 5 μm; Merck, Darmstadt, Germany). Fractions were collected (0.5 min/fraction, for 50 min) and counted in a liquid scintillation counter (Packard Tri Carb 2200CA). Approximate retention times in this system were 17 min for the R-epimer of BUD, 18 min for the S-epimer of BUD, and 28–34 min for fatty acid esters of BUD.
LC System 2.
The equipment was as for LC system 1, but with radioactivity detected on-line with a FLO-ONE detector (Radiomatic, C-525-TRX, version 3.01), using Ultima FLO AP scintillation cocktail (HPLC flow/scintillation flow ratio, 1:4; Packard). Ethanol solutions were diluted to 20% water before injection. The column (Supelcosil LC-18-DB, 3.3 cm × 4.6 mm, 3 μm; Supelco Inc., Bellefonte, PA) was operated at a flow rate of 1 ml/min. A three-phase gradient was used, as follows: phase A, 5% ethanol and 0.1% acetic acid; phase B, 95% ethanol and 0.1% acetic acid; phase C, 0.1% acetic acid. Phase C (0.4 ml/min) was added to the HPLC flow, through a T-connection between the injector and the column, during the injection phase and the first 1 min of the gradient. The total flow rate of phases A and B was 0.6 ml/min for the first 1 min and 1 ml/min thereafter. The initial conditions (60% A/40% B) were maintained for 5.5 min and were then changed stepwise to 15% A/85% B. Between 5.5 min and 11.5 min, the conditions were changed linearly to 100% B; at 13.5 min, the system was returned to the initial conditions. In this system, approximate retention times were 5 min for BUD (with a separation between the two epimers of 0.5 min), 10.5 min for BUD palmitoleate, and 11.3 min for both BUD palmitate and BUD oleate.
Data Analysis.
The total radioactivity measured in the tissue and plasma was converted to the concentration of GCS according to the equation given above and was expressed as GCS equivalents (picomoles per gram for tissue samples and picomoles per milliliter for plasma samples) per administered nanomole. The tissue concentrations of GCS equivalents were compared among steroids, separately for each administration method, and for each airway level (trachea with main bronchi, bronchi of generations 3 and 4, and lung parenchyma). The analysis was based on analysis of variance with two factors [factor 1, treatment (i.e. steroid) or airway level (difference between steroids or airway levels); factor 2, time]. The interaction between steroid/airway level and time was also analyzed. Comparisons among steroids were performed for concentrations at t = 20 min and for percent decreases in concentration over time. The analysis was performed with a multiplicative model, which implies that the mean values of tissue GCS concentrations discussed are geometric means (presented with 95% confidence intervals). Data for in vitro experiments and for extractions with ethanol are given as arithmetic means ± SD.
Results
Demonstration of BUD-C21-Fatty Acid Conjugates in Airway and Lung Tissue.
HPLC analysis of ethanol extracts of airways and lungs from rats that had been topically treated with BUD revealed not only free BUD but also large fractions with much higher lipophilicity than BUD (fig.2), which had been previously shown to be fatty acid conjugates (Tunek et al., 1997). The fatty acid conjugation of BUD in airway and lung tissue was rapid. Within 20 min of topical administration, BUD conjugates represented the majority of total tissue radioactivity, whereas 20–30% of radioactivity represented free BUD (fig. 2A). The ratio between free BUD and the ester fraction decreased with the time between BUD administration and tissue excision (fig. 2); 24 hr after BUD administration, only a small percentage of free BUD was discernible in the HPLC radiochromatograms of tracheal extracts (fig. 2C). However, the tracheal concentration of BUD equivalents after 24 hr was only 3.2% of the level found after 20 min, showing that the bulk of the initially deposited BUD had been exported from the tissue within the 24-hr period (see fig. 6).

Adapted radiochromatograms (LC system 1) of ethanol extracts of trachea (A, B, andC) and lung (D).
Tissue was excised at 20 min, 2 hr, and 24 hr after intratracheal instillation of BUD. Already at 20 min, approximately 80% of total retained radioactivity was represented by conjugates and 20% by free BUD, in both trachea and lung. The fraction of free BUD decreased with time after BUD administration; at 24 hr, almost only BUD conjugates were discernible in the radiochromotograms (note different scales inA–D).

Tissue radioactivity (picomoles of GCS equivalents per gram of tissue), related to 1 nmol administered, at various times after intratracheal instillation of 3H-GCS solutions (250 μl) (BUD at 4.8 × 10−7 M or FP at 1.5 × 10−7 M).
Values are geometric means, with 95% confidence intervals (N = 3 or 4), for each GCS and time point. The values given as percentages express the ratio of tissue radioactivity at 24 hr to that at 20 min.
The ratio between free BUD and C21-conjugates did not vary greatly with different tissue concentrations of total BUD. In perfused tracheal segments, with the deposited radioactivity being equal to approximately 40 or 1500 pmol of BUD equivalents/g of tissue (after perfusion with [3H]BUD at 7.5 × 10−8 or 3.0 × 10−6M, respectively), the proportion of free BUD at t = 20 min was 17 ± 5% (mean ± SD) or 27 ± 1%, respectively. A similar relationship (20% free BUD/80% conjugate) was found in tracheal segments in which perfusion with [3H]BUD at 3 × 10−6 M was preceded by perfusion with unlabeled BUD at a 10-fold higher concentration, which is estimated to yield a tissue concentration equal to approximately 15 nmol of BUD/g of trachea (data not shown). Lipophilic conjugates of BUD were also formed in lung, in proportions similar to those in trachea, and there were indications of other, as yet unidentified, metabolites (fig.2D). Under the conditions used (topical application of BUD to the airways), no BUD conjugates were demonstrable in plasma or in peripheral tissue. For FP and BDP, no fatty acid conjugates were detected in airway or lung tissue even when HPLC fractions were collected for up to 60 min (LC system 1, maintaining 100% mobile phase B).
GCS Release In Vitro and Regeneration of Intact BUD from C21-Esters .
The rate of radioactivity release from tracheal segments into incubation buffer was lower for BUD than for FP, BDP, and HC (fig.3). After 2 hr of incubation, approximately 80% of radioactivity was released from tracheas perfused with FP and BDP and 100% of that from tracheas perfused with HC, compared with 40% release from tracheas perfused with BUD. During the next 6 hr, no further release of FP occurred, whereas the release of BUD was increased by an additional 25% and that of BDP by approximately 15%. The area under the curve describing the radioactivity released from the trachea as a function of time (0–8 hr) was nearly 2-fold lower (p < 0.001) for tracheas perfused with BUD, compared with other steroids.

Percentage of total tissue radioactivity released from tracheal segments in an 8-hr in vitroincubation in buffer.
Tracheal segments were perfused with 3H-GCS (BUD at 7.1 × 10−8 M, FP at 1.2 × 10−7 M, BDP at 9.9 × 10−8 M, or HC at 7.4 × 10−8 M) for 10 min, followed by perfusion with saline. The trachea was excised 20 min after the start of perfusion. Values are arithmetic means (N = 4) for each GCS. The BUD AUC is nearly 2-fold lower than those for other GCS (p < 0.001, analysis of variance, followed by Student′s t test).
At the beginning of the incubation, 70–80% of radioactivity in BUD-treated tracheas was present as BUD conjugates and 20–30% as free BUD. During the 8-hr incubation, approximately 65% of radioactivity was released (fig. 3); free BUD was decreased 5–15-fold and the conjugate fraction was decreased 2–3-fold (fig.4, A and B). HPLC analysis of the incubation medium revealed that >90% of the total radioactivity released into the buffer was in the form of free BUD (fig. 4C) and the conjugate fraction made up <3%. This indicates that efflux of BUD from the tracheal tissue was preceded by hydrolysis of conjugates and that at least 50% of the conjugate fraction was hydrolyzed. Nevertheless, the conjugate fraction represented >90% of the total radioactivity remaining in the tissue after incubation.

Adapted radiochromatograms (LC system 2) of trachea ethanol extracts (A and B) and trachea incubation buffer (C) from a single experiment.
Ethanol extracts were made of two halves of the same, longitudinally divided, tracheal segment, collected 20 min after intratracheal instillation of [3H]BUD; one half was extracted in ethanol directly after excision (A), and the second half was extracted in ethanol after an 8-hr incubation in buffer (B). In A, 15% of total radioactivity was represented by free BUD and 81% by BUD conjugates. During incubation in buffer, the fraction of free BUD was decreased 6-fold and that of BUD conjugates 2-fold (B). The total radioactivity remaining in trachea after incubation consisted of 91% BUD conjugates and 6% free BUD (B). Radioactivity released into the incubation buffer consisted of 93% free BUD and 2% BUD conjugates (C).
Radioactivity released from tracheal segments perfused with FP was identified as exclusively free intact FP; for tracheas perfused with BDP, free beclomethasone dominated in the buffer medium (data not shown). For HC, the concentration of radioactivity in the buffer was too low for separation by HPLC (because of the low uptake of HC into the tissue during the tracheal perfusion) (fig.5).

Tissue radioactivity in the perfused section of trachea (picomoles of GCS equivalents per gram of tissue), related to 1 nmol of GCS perfused, at various times after 10-min perfusion (0–10 min) with 3H-GCS solutions (BUD at 2.9 × 10−7 M, FP at 2.0 × 10−8 M, BDP at 7.2 × 10−8 M, HC at 3.4 × 10−6 M, or DEX at 2.8 × 10−6 M) (GCS perfusion was followed by saline perfusion for 10–120 min).
Values are geometric means, with 95% confidence intervals (N = 3–5), for each GCS and time point. The values given as percentages express the ratio of tissue radioactivity at 120 min to that at 20 min.
Uptake and Retention of GCS in the Airways and Lung.
The local uptake and retention of tritiated GCS in the airways and lung were expressed as the concentration of total tissue radioactivity (picomoles of GCS equivalents per gram of tissue) related to the administered dose (nanomoles). This was possible because the concentration of radioactivity in the airway and lung tissue was always directly proportional to the administered dose of GCS, regardless of the route of administration (data not shown).
The initial concentration of GCS equivalents (at t = 20 min) per administered nanomole in the airways and lung was similar for BUD, FP, and BDP (figs. 5– 7), whereas it was 25–130 times lower for DEX and HC (fig. 5). For all GCS tested, the concentrations of radioactivity in the exposed airways and lung were much higher than those in tissues (including plasma) not directly exposed to the steroids. For BUD and FP, the ratio of the concentration of radioactivity in trachea/main bronchi to that in plasma at 20 min was 103 to 104 after tracheal perfusion, 400–500 after intratracheal instillation, and 25–75 after inhalation. Radioactivity in the sc fat, 20 min after BUD instillation, was approximately 3 times higher than the levels in soleus muscle and plasma and equal to the level detected in colon (not tested for other GCS).
The radioactivity retained in the airways and lung decreased significantly with time after steroid administration (p < 0.0001 for the time factor). The tissue concentration of radioactivity as a function of time differed significantly among steroids (p < 0.0001 for the interaction between treatment and time). After tracheal perfusion, the dwell-time in the tracheal tissue was much longer for BUD and FP than for BDP, DEX, and HC. Two hours after perfusion, approximately 30–40% of initially (at t = 20 min) retained BUD and FP was still present in the tracheal tissue, compared with 3–4% for HC, DEX, and BDP (fig. 5). After inhalation, elimination of BUD from tracheal tissue was slower than for either FP or BDP (p = 0.002 for the interaction between treatment and time) (fig. 7A). Also, after intratracheal instillation (fig. 6), the elimination rate for BUD in trachea and main bronchi was significantly lower than that for FP (35-fold,p = 0.001 for the interaction between treatment and time). In spite of the prolonged retention of BUD in the tissue, >95% of BUD disappeared from airway tissue within 24 hr of administration (fig. 6).

Tissue radioactivity (picomoles of GCS equivalents per gram of tissue), related to 1 nmol administered, in trachea and main bronchi (A), bronchi of generations 3 and 4 (B), and lung parenchyma (C) after 5-min inhalation (0–5 min) of nebulized ethanol solutions of3H-GCS (BUD at 3.4 × 10−6 or 6.3 × 10−6 M, FP at 2.4 × 10−5 M, or BDP at 1.3 × 10−5 M).
Values are geometric means, with 95% confidence intervals (N = 4), for each GCS and time point. The values given as percentages express the ratio of tissue radioactivity at 6 hr to that at 20 min. The values of tissue radioactivity measured at 6 hr in parenchyma are given in parentheses because they probably represent mainly liver-derived metabolites with weak GCS activity.
The cellular and subcellular localization of the BUD-21-conjugate in the airways is not known. However, a pilot autoradiographic study examining tracheal segments 2 hr after perfusion with [3H]BUD revealed radioactivity over the entire cross-section of the trachea, with the highest levels in the mucosal and serosal compartments (fig. 8).

Tape section autoradiogram of a cross-section of a tracheal segment perfused with [3H]BUD at 2.8 × 10−7 M (10 μCi/ml) for 10 min, followed by continuous perfusion with saline for the next 110 min.
The dark areas identify the localization of radioactivity. Maximal radioactivity is seen in the mucosal and serosal compartments.Arrow, position of the tracheal smooth muscle.
Discussion
Reversible BUD Conjugation with Fatty Acids.
Biosynthesis of fatty acid esters of estrogens, ecdysteroids, and, to some extent, mineralocorticoids and GCS has been described in a variety of tissues and species (Pahuja and Hochberg, 1989). It has been proposed that esters of endogenous estrogens are body reservoirs of latent estrogens, requiring only lipase-catalyzed hydrolysis for activation (Pahuja and Hochberg, 1989; Hochberg et al., 1991).
The present study shows that topically administered BUD is reversibly conjugated, at its C21-hydroxyl group, with fatty acids within airway and lung tissue. In trachea and main bronchi, approximately 70–80% of retained BUD was conjugated within 20 min of BUD administration. The fraction conjugated appears to be dose-independent within a wide range, including clinically relevant doses. The enzyme system conjugating BUD seems to have considerable capacity, because no saturation of uptake or conjugation reactions was seen, even at concentrations that exceeded, by several orders of magnitude, the concentration required for 50% GCS receptor saturation. Therefore, the absolute conjugate levels depend on BUD availability, explaining why the highest conjugate concentration is seen in the large airways, where the deposition is greater per surface area and the absorption rate is probably slower than in peripheral lung.
Conjugation of BUD is a reversible process. The in vitroexperiments showed that BUD-21-conjugates in the tissue are hydrolyzed intracellularly, gradually releasing free BUD into the surrounding medium. The release rate of GCS from the tracheal tissue is lower for BUD than for FP, BDP, and HC, probably because it is partly dependent on the rate of hydrolysis of BUD conjugates (although the first pool to be released is probably free BUD). During incubation of tracheal segments in vitro, the tissue-bound BUD was released almost exclusively in the form of free BUD, although it was initially present mostly as fatty acid conjugates within tissue. In vivo, >95% of deposited radioactivity left the tracheal tissue within 24 hr of BUD administration, suggesting final hydrolysis of BUD conjugates and release of free BUD from target tissues.
We did not have at our disposal reference fatty acid conjugates of FP or 17-BMP/beclomethasone. However, conjugates of 17-BMP would be approximately as lipophilic as BUD conjugates, and conjugates of beclomethasone would be less lipophilic. Therefore, if formed in appreciable amounts, these would have been detected in our LC systems. C21-conjugates of FP are theoretically impossible, because of the molecular structure of FP. Conjugates at C11 are highly unlikely, as detailed previously (Tunek et al., 1997). If formed, these conjugates would be very lipophilic and would most likely elute at later retention times, compared with BUD conjugates, but none were detected. Rapid hydrolysis of C21-conjugates, as occurs with corticosterone (Pahuja and Hochberg, 1989; Hochberg et al., 1991), may also explain why no conjugates were found for beclomethasone, which contains an hydroxyl group at C21. Hydrolysis of BUD C21-conjugates may be slowed by the steric hindrance of the acetal group at C16α–17α, thus allowing the build-up of a depot of C21-fatty acid esters.
The BUD-21-conjugates are themselves inactive as a GCS (Wieslanderet al., 1998). This is in accordance with previous findings (Würthwein et al., 1992) that steroids esterified at C21 have negligible affinity for the steroid receptor. However, gradual release of free BUD from the C21-conjugate may prolong receptor saturation and cause protracted GCS activity. After inhalation, the major depot of BUD conjugate is formed within airways and lung and, thus, the prolonged activity of inhaled BUD is concentrated within the target tissues for asthma therapy. Two recent studies suggest that the fatty acid esterification of BUD results in prolonged anti-inflammatory action. In the Rat1 cell model, where a similar reversible conjugation of BUD occurs, a pulse of BUD results in a longer GCS effect than does a pulse of FP (Wieslander et al., 1998). In addition, functional studies in vivo in rat airways show that the topical anti-inflammatory activity of a single dose of BUD is prolonged, compared with that of FP (Miller-Larsson et al., 1997).
Nonspecific (Non-Receptor) Tissue Affinity.
The approximately equal initial local concentrations of BUD, FP, and BDP in the airway and lung tissue after inhalation of doses below or at the lower limit of the clinically relevant range (table 1) show that topical tissue uptake of inhaled GCS is not strictly related to the lipophilicity of the intact steroids (table2) or to steroid receptor affinity. The receptor affinity for BUD is approximately 2–3-fold lower than that for FP, approximately 1.5–2-fold lower than that for 17-BMP, and approximately 20-fold higher than that for BDP (Dahlberg et al., 1984; Hochberg et al., 1991; Högger and Rohdewald, 1994). Although there were only minor differences among the GCS in initial tissue uptake, BUD had a significantly longer dwell-time in large airway tissue than did FP and BDP, in spite of the shorter half-life ( Högger et al., 1993; Högger and Rohdewald, 1994) of the BUD-receptor complex in vitro (5–6 hr), compared with the receptor complex for FP (10 hr) or 17-BMP (8 hr). Therefore, the differences among BUD, FP, and BDP in local tissue binding are not determined at the receptor level but more likely reflect different degrees of nonspecific binding of GCS to cellular and subcellular membranes (directly related to the lipophilicity of the main GCS storage forms). BUD is approximately 6–8 times less lipophilic than FP and approximately 40 times less lipophilic than BDP (table 2). However, BUD-21-conjugates are 2–4 orders of magnitude more lipophilic than intact BUD, which probably explains the longer dwell-time of BUD in airway tissue.
GCS lipophilicity estimated by chromatographic capacity factor logk′(0)
Although BDP is more lipophilic than FP, its dwell-time in the airway tissue is shorter than that of FP and similar to that of DEX. This is probably the result of hydrolysis of BDP to monopropionates and even to beclomethasone, which has lipophilicity similar to that of DEX. The significantly longer dwell-time of radioactivity in the trachea for BDP after inhalation than after tracheal perfusion is probably explained by very slow dissolution of BDP crystals deposited in the respiratory lumen during inhalation (Högger et al., 1993).
The results of this study clearly show that GCS of the inhaled type reach concentrations in the airway tissue that exceed receptor saturation. The receptor affinity (Kd ) determined in vitro for BUD, FP, and 17-BMP is approximately 1 pmol/ml (Dahlberg et al., 1984; Högger et al., 1993; Högger and Rohdewald, 1994), meaning that 50% receptor saturation is achieved at this concentration. In the present study, the initial absolute (picomoles per gram) tissue concentration of GCS equivalents achieved in the airways after inhalation of clinically relevant doses was several times higher than the receptor affinity, e.g. 8 pmol/g of tissue was obtained in trachea and main bronchi 20 min after inhalation of [3H]FP at a dose 3.7 nmol/kg of body weight. Even higher tissue concentrations were achieved after intratracheal instillation, e.g. 400 pmol/g of tissue was obtained 20 min after instillation of [3H]BUD at 11.4 nmol/kg of body weight. Furthermore, a tissue concentration of 1500 pmol of BUD equivalents/g was measured in trachea after perfusion with [3H]BUD (at 3 × 10−6 M). In addition, the uptake of [3H]BUD during such perfusion was not decreased by pretreatment with unlabeled BUD, even at a 10-fold higher concentration (data not shown), indicating a final tissue concentration of 15 nmol/g. The finding that tracheal tissue was not saturated even at such a high tissue concentration supports the nonspecific nature of GCS tissue binding.
Clinical Situation.
We have shown that topically applied GCS of the inhaled type (BUD, FP, and BDP) are markedly better taken up from the respiratory lumen and are also better retained within airway tissue, compared with GCS of the noninhaled type (HC and DEX), which helps to explain the relatively poor antiasthmatic activity and selectivity of inhaled HC and DEX. The initial (at t = 20 min) concentrations of BUD equivalents and FP equivalents in the airway tissue were of the order of 10 pmol/g per inhaled nanomole and 100 pmol/g per instilled nanomole, reflecting airway deposition of approximately 10% of the inhaled dose (Eirefelt et al., 1992). Lung depositions of 10–15% are also achieved in human patients with the majority of inhalers (Borgström, 1993). Therefore, the instilled doses of 0.1–10 nmol/kg of body weight used in the present study (table 1) were equivalent to inhaled doses of 1–100 nmol/kg of body weight. The initial GCS equivalent tissue concentration of 10 pmol/g per inhaled nanomole in trachea (with approximately 4-fold lower concentrations in lung parenchyma) was obtained in the present study with rats of approximately 300-g body weight. Allowing for the 250-fold greater body weight and 250-fold larger alveolar surface area (Mercer et al., 1994) of 70–80-kg humans, one can calculate that the inhalation of clinically relevant GCS doses of 0.2–2 mg (400–4000 nmol) would result in initial GCS concentrations of approximately 16–160 pmol/g in the airway tissue and 4–40 pmol/g in lung parenchyma. According to our findings, these concentrations would decrease approximately 2–4-fold in the large airways and 3–10-fold in lung parenchyma 2–6 hr after inhalation. The tissue concentrations obtained are in very good agreement with the results of the human study by Van den Bosch et al. (1993), who reported a concentration of BUD in human peripheral lung averaging 5.5 pmol/g of tissue 1.5–4 hr after inhalation of 1.6 mg.
The initial concentrations calculated here would exceed the receptor affinity Kd by a factor of 16–160 in the airway tissue and 4–40 in lung parenchyma. Therefore, even with 70–80% of BUD conjugated to fatty acids, the local tissue concentrations of free BUD would mostly exceed the level of 50% receptor saturation. These calculations suggest that the minor differences in receptor affinities and immediate local tissue concentrations for BUD, FP, and BDP may be of no functional importance. Rather, differences among steroids in their local tissue dwell-times may be the crucial factors determining the duration of topical anti-inflammatory activity and airway selectivity.
Conclusion.
We have shown that intracellular fatty acid esterification of BUD within airway tissue results in a local depot of latent, slowly regenerable, free BUD. This esterification prolongs the exposure of airway tissue to active GCS, compared with the exposure achieved with FP or BDP. The prolonged tissue exposure, and thus protracted receptor saturation, may explain the prolonged anti-inflammatory activity of BUD within rat large airways, compared with FP. It is tempting to speculate that the described esterification of BUD contributes to the airway selectivity and to the efficacy of BUD in asthma treatment when it is inhaled once daily.
Acknowledgments
We acknowledge Professor Ingvar Brandt for performing the autoradiographic analysis of tracheal segments. We thank Karin Sjödin for contributing to HPLC analysis and Dr. Anders Källén for statistical analysis of the data. We are also grateful to Dr. Kevin Cheeseman and to Elisabet Wieslander for valuable comments on the manuscript.
Footnotes
-
Send reprint requests to: Anna Miller-Larsson, Astra Draco AB, Department of Pharmacology, P.O. Box 34, S-221 00 Lund, Sweden.
- Abbreviations used are::
- GCS
- glucocorticosteroid(s)
- BUD
- budesonide
- BDP
- beclomethasone dipropionate
- FP
- fluticasone propionate
- HC
- hydrocortisone
- DEX
- dexamethasone
- BMP
- beclomethasone monopropionate
- Received November 20, 1997.
- Accepted March 4, 1998.
- The American Society for Pharmacology and Experimental Therapeutics




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}