Article Text

Abstract
Objective: To report 8 years’ data from a UK-wide audit of acute wheeze/asthma management in children carried out annually since 1998.
Design: Paediatricians were invited to complete a simple form based on British Thoracic Society (BTS) asthma guidelines for any child over 1 year of age admitted with acute wheeze/asthma each November from 1998 to 2005. Information was collected about patient demographics, initial hospital severity assessment, in-hospital treatment, asthma education and emergency planning, discharge treatment and follow-up.
Results: Data on 9429 admissions were available, with between 53 and 67 centres participating each year. The majority of children were under 5 years of age (median age 3 years). Nearly all were treated with bronchodilators, and around 90% received systemic steroids. Vital signs (pulse and respiratory rate) and oxygen saturation on admission remained stable over the audit period. However, the proportion of admitted children given bronchodilators exclusively by spacer increased from 7% to 44% between 1998 and 2005. The proportion discharged with written asthma plans increased from 24% to 41%. Wide variations were noted between centres in the proportions of children receiving chest x rays and written asthma plans. Children admitted under the care of a respiratory specialist were more likely to have documentation that they had been given written asthma information and a written asthma plan and had had their inhaler device technique checked than if under the care of a general paediatrician.
Conclusions: In many areas, hospital treatment closely followed published guidance. However, some important deficiencies were noted and variations remain. As well as monitoring guideline implementation, national audit can highlight opportunities for research and improving care locally and nationally.
Statistics from Altmetric.com
Hospital admissions for childhood asthma increased markedly from the 1970s until the early 1990s. Although there is some evidence that the number of acute asthma episodes in children has fallen slightly,1 they remain one of the most common medical reasons for hospital admission.
The first international guidelines on the management of asthma in children were published in 1989.2 UK national guidelines on the management of asthma in adults followed in 19903 4 and in 1993 included childhood asthma.5 Since then there have been many revised and updated versions, both nationally and internationally.6–9 However, throughout this period the key elements in the management of acute severe asthma in children have remained unchanged.
Previous studies have shown that acute asthma care deviates from guideline recommendations.10–12 An audit of hospital care of adults with acute severe asthma in the UK found many deficiencies and confirmed wide variations between hospitals and between respiratory and non-respiratory specialists.12
Earlier attempts to establish a national paediatric asthma audit system in the UK were largely unsuccessful, partly because of dataset complexity and partly because of the long delay in providing feedback to participants. A six centre pilot study encountered major problems in question design and data recording,13 while long delays between data collection and feedback militated against using the data to improve care.
We report data from an on-going annual UK-wide audit of children admitted to hospital with acute wheeze/asthma using a simpler paediatric dataset based on the UK asthma guidelines.6 Using this dataset, paediatricians throughout the UK have provided data on children admitted with acute wheeze/asthma each November from 1998. This paper details the findings.
METHODS
Dataset and audit form
A simple dataset was developed based on British Thoracic Society (BTS) guidelines for the management of acute asthma.6 Information was collected in six key areas: patient demographics, initial asthma severity assessment, in-hospital treatment, asthma prophylaxis (if any), asthma education and emergency planning, and follow-up arrangements.
The dataset was incorporated into a simple machine readable form. This was extensively piloted before use to ensure that information was likely to be easily available from clinical notes, and that the form was unambiguous and easy to complete. From 2002, centres could also submit their responses on-line using an electronic version. Entering the required information takes around 5 min per child. Where there was no information in the clinical notes, for example about checking inhaler device technique, answers were coded as not done.
Participating centres and subjects
In 1998, all 89 paediatricians with a respiratory interest listed in the BTS handbook were written to inviting them to take part in an audit of acute wheeze/asthma in children admitted during the month of November. In addition, consultant paediatricians in all acute paediatric units in Scotland were invited to take part.
Those clinicians (one per centre) who agreed to take part were asked to provide data on children over 1 year of age with wheeze/asthma admitted at their centre (including those not directly under their care) using the form. An admission was defined as more than 4 h in hospital from triage to discharge. Children under 1 year of age were excluded because bronchiolitis due to respiratory syncytial virus infection, a common cause of wheezing in young children, is most common in the first year of life. There was no specific upper age limit cut-off.
In the first year, paediatricians from 56 centres returned data. In subsequent years, clinicians who had already participated as well as clinicians in other centres who asked to take part have repeated the audit each November. Not every centre has returned data every year.
Data analysis
Completed forms were returned to Glasgow and machine read using optical character recognition software (Formic v 3.4) into an Access database (Microsoft). In later years, data submitted using the electronic form were incorporated into the database directly.
Standard reports presenting each centre’s results and comparisons with the aggregated national data for that year were returned to the participating centre around the end of the following January, two calendar months after the end of data collection.
Statistical analysis
Relationships between categorical variables were investigated using χ2 tests. χ2 Tests for trend were performed on binary variables to determine changes over the time period of the audit. Binary logistic regression was used to determine which variables were associated with the number of previous admissions and discharge planning documentation. All tests were carried out using Minitab (v 14) at a significance level of 5%.
Ethics
The data form only involved the collection of routinely available data from review of case notes. Patient identifiers were used locally to identify the relevant patients but were removed when submitted to the central database. Because of this, ethical consent was not sought.
RESULTS
Participating centres and subjects
Data from 9429 admissions between November 1998 and November 2005 were returned (table 1). A data completeness table is available as a supplementary table online. In total, 98 different centres have been involved. Of these, 15 have submitted data for all 8 years and 76 for ⩾3 years. The median number of admissions submitted per centre per year was 17 (range 1–100, interquartile (IQ) range 12–25). Between 74% and 82% of admitted children were under the care of general paediatricians with the remainder under the care of respiratory specialists (table 1).
Patient demographics
The median age of children admitted was 3 years (range 1–18 years). This has remained unchanged. Overall, 62% were boys and 38% girls. More than one in five admissions were for children aged 12–24 months (table 1). The median length of stay was 1 day. While for the majority of children the recorded episode was their only admission that year, 34% were recorded as having had at least one other admission in the 12 months prior to the current admission (20% one previous admission, 7% two previous admissions and 7% three or more previous admissions). Children under the care of paediatric respiratory specialists were more likely to have had previous admissions in the previous 12 months and to be aged ⩾6 years.
Clinical severity assessment
Pooled data for the entire audit period reporting initial heart rate, respiratory rate and pulse oximetry readings are shown in table 2. Data are not shown for each year of audit individually, but in the youngest age group the median respiratory rate on admission has seen a small downward trend over time. There has been no change for older children. There has been a small rise (from 94% to 95%) in the median arterial oxygen saturation (in air) at admission over the period of audit for the 12–24-month-old age group. Median values for older children have remained static at 94% in air.
In-hospital treatment
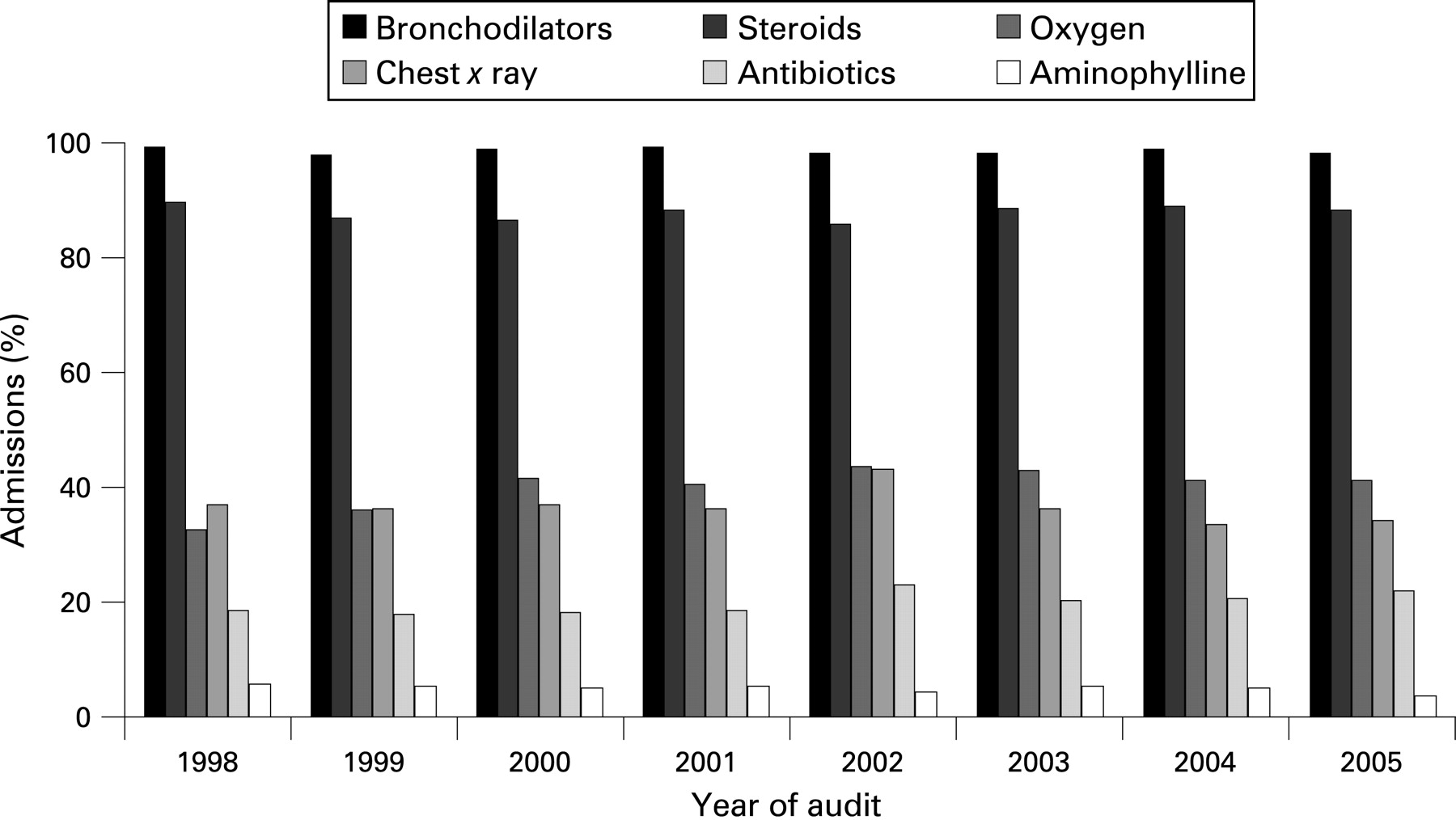
Overall, almost 90% of children received systemic corticosteroids, either oral or intravenous, during their admission with no change over time (χ2 test for trend, χ2 = 0.05, p = 0.8) (fig 1). The median percentage of children being given systemic steroids in the 45 centres submitting data for ⩾10 admissions in 2005 (to reduce skewing of results from centres returning smaller numbers of admissions) was 91% (IQ range 80–96%). Only 4–5% of admitted children each year were treated with intravenous aminophylline.

While the percentage of children receiving bronchodilators at all ages has always been close to 100%, the method of delivery has changed substantially (fig 2). A spacer device for bronchodilator delivery was used exclusively for only 7% of admitted children in 1998. By 2005, 44% of bronchodilators were administered in this way (χ2test for trend, χ2 = 833.4, p<0.001), a change accompanied by a marked decline in the use of nebulisers. Over the audit period, those children treated with bronchodilators delivered exclusively by nebuliser were more likely to have an initial oxygen saturation <92% in air than those whose bronchodilators were delivered by spacer device alone (26.0% vs 9.8%; χ2 test, χ2 = 139.0, p<0.001) and more likely to be given oxygen during their admission (33.5% vs 17.1%; χ2 test, χ2 = 101.4, p<0.001). However, conversely 66.5% children who were treated exclusively with nebulisers during their admission never received oxygen treatment (for any period) during their stay.

{kind=link}
{kind=link}
Around one in five children were given antibiotics as part of their in-hospital management (fig 1), with a small upward trend between 1998 and 2005 suggesting increasing antibiotic use.
Over the audit period, the proportion of admitted children having a chest x ray has ranged from 33% to 43% per year with no significant change over time (χ2 test for trend, χ2 = 3.2, p = 0.08). Having a chest x ray was associated with antibiotic prescription. In 2005, 49% of children who had a chest x ray were given antibiotics; in those not x rayed, only 8% of children were given antibiotics. This pattern has remained constant over time.
While the overall proportion of children x rayed has remained relatively constant, wide variations exist between individual centres. In the 46 centres submitting data for ⩾10 admissions in 1998, 0–83% of admissions per centre were x rayed (IQ range 21–52%). Similarly, across 45 such centres in 2005 the range was 0–78% (IQ range 20–52%).
Asthma prophylaxis and discharge planning
Being on regular prophylaxis medication at admission or discharge was associated both with the number of previous admissions and with age. Any previous acute admission in the preceding 12 months was associated with a higher likelihood of being on asthma prophylaxis (table 3).
Between 48% and 56% of admitted children each year were documented as having had their inhaler device technique assessed, but this has decreased over time and in 2005 was the lowest since the audit started. In contrast, the proportion of children documented as receiving a written asthma plan increased from 24% in 1998 to 41% in 2005 (χ2 test for trend, χ2 = 109.4, p<0.001). Despite this overall improvement, substantial variation was noted between individual centres. The proportion of children given a written asthma plan in centres submitting ⩾10 admissions ranged from 0% to 100% (IQ range 1–32%) across 46 centres in 1998 and 0–100% (IQ range 8–66%) across 45 centres in 2005. Between 34% and 43% of admitted children each year were given written asthma information. Children with previous admissions were less likely to have documentation of their inhaler technique being assessed (table 3).
Children admitted under the care of a respiratory specialist were more likely to have documentation of being given written asthma information/leaflets and a written asthma plan and having their inhaler device technique checked prior to discharge (table 4).
Follow-up
The proportion of children who were recorded as having been recommended to see their general practitioner within 1 week following discharge rose from 19% in 1998 to 32% in 2005 (χ2 test for trend, χ2 = 107.0, p<0.001). Conversely, the proportion of children for whom secondary care follow-up was arranged fell over time to 47% of all admissions in 2005 (χ2 test for trend, χ2 = 17.7, p<0.001).
In comparison to a child being admitted for the first time, children with one or more previous admissions in the last 12 months were significantly more likely to have secondary care follow-up arranged (table 3). Overall, 45% of children with no previous acute admissions had secondary care follow-up arranged, in comparison to 86% of children with three or more previous admissions.
Children aged 12–24 months
Children in this age group accounted for over 20% of admissions. There was no difference in the proportion having a chest x ray in comparison to older children. They were less likely to have been given systemic steroids than children aged ⩾2 years, with 75% of them given steroids in comparison to 90% of 2–5-year-olds and 95% of those aged ⩾6 years (χ2 test, χ2 = 416.2, p<0.001). Children aged 12–24 months were less likely to be on prophylaxis medication than older children. In total, 26% of admitted children aged 12–24 months were already on prophylaxis medication at admission in comparison to 46% of those aged 2–5 years and 68% of those aged ⩾6 years (χ2 test, χ2 = 816.7, p<0.001). At discharge from hospital, 43% of children aged 12–24 months were on prophylactic medication. This age group was also less likely to have follow-up arranged in secondary care.
DISCUSSION
In this report, we present data from 1998–2005 from a large, ongoing UK audit of children admitted to paediatric units with acute wheeze/asthma each November. Using national hospital episode statistics on children admitted with acute asthma exacerbations, we estimate that the data returned equate to around 37% of total UK paediatric wheeze/asthma admissions during November.14 15
Strikingly, the characteristics of children presenting with acute wheeze/asthma in terms of age, sex, previous admissions, severity (as reflected in physiological parameters at admission) and length of stay has remained relatively stable over the 8 years. Our data therefore provide a benchmark against which current guidelines can be calibrated and against which changes in care can be assessed. For example, using severity criteria from the UK BTS/SIGN (Scottish Intercollegiate Guidelines Network) asthma guidelines,7 25% of children aged 2–5 years would have been categorised as having a “severe” exacerbation on the basis of respiratory rate. This increases to 75% if heart rate is used as the defining parameter (table 2), a degree of discordance that suggests that the sensitivity and specificity of these widely used severity cut points need to be reviewed.
It is clear that in important aspects current emergency asthma management in children has changed in line with published guidelines. For example, almost 90% of admitted children received systemic steroids, higher than the 78% reported by Hilliard et al in their 1-year prospective study between 1995 and 1996 of acute asthma admissions in children from 10 centres in the UK10 and more recently by Kelly et al in their prospective study of emergency asthma care in Australia.16
A very high proportion of children have always received bronchodilator treatment, but there has been a progressive change in delivery method with many more children now only receiving bronchodilators via spacer and fewer receiving nebulised treatment. This perhaps reflects a gradual and cautious assimilation of the evidence concerning the efficacy and safety of high dose bronchodilator delivery via spacer into acute asthma care in routine clinical practice.17
Not unexpectedly, there are aspects of care where care is not soundly evidence based. Chest x rays in children with acute asthma rarely produce additional useful information18 and are not routinely indicated.7 Yet we noted that consistently over one third of children were reported to have had a chest x ray, with wide variation between centres. Furthermore, the number of children x rayed is an important measure because it appeared to be strongly linked to antibiotic prescription. Since most childhood asthma exacerbations are triggered by viral infection, the proportion of children prescribed antibiotics is likely to have been inappropriately high. Therefore, local strategies that successfully reduce unnecessary chest x rays19 20 may also reduce inappropriate antibiotic prescribing.
Many young children will have virally induced exacerbations with no interval chronic asthma symptoms. While the effect of maintenance therapy with inhaled corticosteroids in children with persistent wheezing is well documented, recent studies have found that that early intervention with either intermittent21 or continuous inhaled corticosteroid therapy22 has no effect on the development of persistent wheezing or asthma in young children. Consequently, in such children with a first or second exacerbation, many paediatricians would not immediately start prophylactic therapy but would review the situation if more exacerbations occurred. In keeping with this developing evidence base, we found that the proportion of children on regular prophylaxis increased with the number of previous admissions and with the age of the child.
The data collected also highlight areas where current guidance is deficient. It is striking that children aged between 12 and 24 months accounted for over one in five admissions. Yet this is a group where the evidence base is limited and guideline recommendations sparse. Such a lack of guidance may partially explain why children in the 12–24-month-old age group were less likely to be given systemic steroids. Nevertheless, it is of interest that 26% of these young children were already on regular asthma prophylaxis at the time of admission and 43% were discharged home on regular prophylaxis medication.
A hospital admission is often viewed as, in part, a failure of chronic asthma management.23 Several studies have shown that despite publication of asthma guidelines, standards of care continue to fall short of that recommended, particularly in the proportions of children prescribed regular inhaled corticosteroids, given written management plans and asthma education, and followed-up.24–27 Overall, the proportion of children with documentation of having received written asthma information, written asthma plans and inhaler technique checks were disappointingly low. It was also disappointing that children with previous acute admissions were even less likely to have had their inhaler device technique checked.
A previous study also found wide variation in elements of discharge planning between centres.10 Our results confirm that such variations still exist despite the widespread dissemination of up-to-date asthma guidelines.28 Our data also provide evidence that for some important aspects of care children were more likely to receive management in line with guideline recommendations under the care of a paediatric respiratory specialist. Differences in asthma management between specialists and non-specialists have previously been described for adults admitted with acute asthma in the UK12 29 and for US children according to whether their usual source of asthma care was a specialist or generalist.30
To minimise the variation seen between centres and between specialists and non-specialists, quality improvement (QI) processes beyond clinical audit will be required to accelerate change. Audit and feedback alone can only be expected to have small to moderate influences on practice.31 32 The most successful interventions often include multiple strategies, including provider education and reminder systems, decision support, patient education, organisational change, and financial incentive, regulation and policy.33
What is already known on this topic
Acute wheeze/asthma is a common reason for childhood admission to hospital in the UK.
UK national guidelines exist for the management of acute asthma in children.
What this study adds
There has been a significant increase in the use of spacers to deliver bronchodilators in the hospital setting over an 8-year audit period despite asthma severity (as reflected in vital signs at admission) remaining stable.
In several key areas, particularly around components of discharge planning, care continues to fall below that recommended by national guidelines, with differences seen between centres throughout the UK and between respiratory and general paediatricians.
This audit only used feedback as a potential mechanism for change. We fed back the results of local centre data and their comparison with aggregated national averages. Where change has occurred (such as in the use of written asthma plans), we are unable to comment on the influence of any additional local QI strategies beyond feedback of audit results alone. Although data have not been collected by this audit to date, we are aware that several centres use integrated care pathways (ICPs) for acute wheeze/asthma and reminder systems for discharge planning. Their use may potentially explain some of the differences seen between centres. Clinical care pathways for children admitted with acute asthma are effective in reducing length of admission to hospital and improving care (including provision of asthma education and prophylaxis medication),34 35 as illustrated by a recent study in which Cunningham et al found that children were more likely to receive asthma education and a discharge plan when an ICP for acute wheeze/asthma was used.36
Many aspects of the present audit document the process of care rather than its outcome. However, there are examples in the wider literature where documentation of the process of care reflects practice that impacts on outcomes such as mortality.37 For asthma care, practices promoted by guidelines, for example written management plans, are associated with lower rates of hospitalisation and emergency care.38 39 Health-related quality of life measures are also associated with whether or not adult patients with asthma are treated according to guideline recommendations.40 In Finland, implementation of their National Asthma Programme has been successful in reducing the morbidity and economic costs associated with asthma.41
Limitations
These data rely on the quality and completeness of information documented in case notes. Accurate documentation is not only imperative for good clinical care but also for maximising the validity of audit data. It is also always likely that some actions that were not documented were actually completed, with consequent underestimation of these aspects of care. However, we think it unlikely that care that is not recorded is consistently delivered. Incomplete data may also mean that some of the statistical analyses suggesting associations may in fact have arisen by chance. We also acknowledge that by inviting paediatricians with a respiratory interest to submit data from their centre (whether the patients were admitted under their care or not), we may have under-represented district general hospitals in which there is no respiratory specialist and potentially overestimated the true national averages for some elements of care.
CONCLUSION
This national UK audit of acute wheeze/asthma in children has shown that in many areas care either reflects or has changed in line with national guidelines and evolving evidence. However, variations in clinical management apparently unrelated to differences in asthma severity persist between individual centres. National asthma audits can provide an important tool for benchmarking care and potentially improving the quality and consistency of hospital care to ultimately ensure consistent, high quality care is delivered to all.
Acknowledgments
We are grateful to all the staff – senior and junior paediatricians, nurses and audit staff – throughout the paediatric centres in the UK that took part in these audits.
REFERENCES
Footnotes
▸ An additional table is published online only at http://adc.bmj.com/content/vol93/issue11
Competing interests: None.