Article Text

Abstract
Objective: Assays based on interferon γ (IFNγ) are an exciting new development for screening for latent tuberculosis infection (LTBI) in adults, but there are limited data on their effectiveness in children. Nevertheless new National Institute for Health and Clinical Excellence (NICE) guidelines recommend their use when screening paediatric tuberculosis (TB) contacts. We evaluated the potential effect of the new NICE guidelines on current paediatric practice.
Design: Children screened for TB who had had an IFNγ assay performed (QuantiFERON-TB Gold (QFG)) were included. Actual outcomes from existing guidelines were compared with those that would have been obtained using NICE guidelines.
Results: QFG assays were performed on 120 children, 103 as part of TB contact tracing. Six of the 120 (5%) were QFG positive, and seven of the 120 (6%) were indeterminate. Where both Mantoux and QFG results were available, these agreed in 62/104 (60%) of cases. QFG tests were more likely to correlate with a negative Mantoux (98% agreement) than with a positive Mantoux (11% agreement). Management outcomes differed for 23/103 children seen as part of TB contact tracing. Only one (1%) of these had an indeterminate QFG result. 17 (85%) fewer children would have been given LTBI treatment (chemoprophylaxis) and two (2%) children with possible TB would not have been identified using NICE guidelines.
Conclusion: New NICE guidelines for the use of IFNγ-based tests for TB screening will reduce the number of children treated for presumed LTBI. Long-term prospective studies are needed to determine the number of children with positive Mantoux tests but negative IFNγ results who are not given LTBI treatment yet later develop TB.
Statistics from Altmetric.com
In March 2006 National Institute for Health and Clinical Excellence (NICE) tuberculosis (TB) guidelines1 replaced the British Thoracic Society (BTS) guidelines,2 introducing the first new diagnostic tests for detecting infected TB contacts for 100 years.
Two new commercially available in vitro tests, QuantiFERON-TB Gold (QFG), (Cellestis Ltd, Victoria, Australia) and T Spot TB (Oxford Immunotech, UK), use the fact that T cells stimulated by antigens specific to Mycobacterium tuberculosis (MTB) produce interferon γ (INFγ).3 Either IFNγ (QFG) or IFNγ-secreting cells (T Spot TB) are measured. Compared with the tuberculin skin test (TST) they are less subjective, and by using MTB-specific antigens the risk of false positive results owing to cross-reactivity with BCG or non-tuberculous mycobacterium (NTBM) is reduced.3 False positives may still occur with other less common NTBM species.3
Data in adults suggest that IFNγ tests are sensitive to active TB and are as good or better than the TST in detecting LTBI.3 4 There are little data exploring their use in children5–7 14or routine clinical practice.8 9 The actual effect of introducing these tests on screening procedure and outcomes is unknown.
Under NICE guidelines, patients with positive Mantoux results (or for whom Mantoux testing may be unreliable) undergo IFNγ testing, if available. The results determine further clinical decision-making.
After using QFG as an additional test in our children’s TB clinic for 18 months we compared practice and outcomes under current local TB guidelines against those that would have occurred if NICE guidelines had been followed.
METHODS
Children on whom QFG tests were performed in Newcastle General Hospital between March 2004 and November 2005 were identified from Health Protection Agency (HPA) laboratory records. Age and BCG status, reason for testing, Mantoux result, CXR result and clinical details were obtained from hospital records and our children’s TB database.
QFG was performed according to the manufacturer’s instructions. Whole blood was incubated with both a negative (nil) and positive (mitogen) control as well as with MTB antigens. IFNγ was detected using an enzyme-linked immunosorbent assay. Results were recorded as positive, negative or indeterminate. A large response to the negative control (>8.0 IU/ml) or failure to respond to the positive control (<0.5 IU/ml) in the face of a negative TB antigen result (<0.35 IU/ml above nil control or ⩾0.35 and <25% of nil value) was designated indeterminate.
Expected treatment outcomes for each child were defined using NICE TB guidelines and Newcastle’s Paediatric TB guidelines (table 1). Newcastle TB guidelines are adapted from the BTS 2000 guidelines;2 the assessment process differs but outcome and management points are the same. Although all children underwent a QFG test, in the analysis of comparative management outcomes, those who would not be offered an IFGγ test following the NICE algorithm were assigned to “no QFG test”.
The audit was registered with The Newcastle upon Tyne Hospitals NHS Trust.
RESULTS
The QFG test was performed on 120 children (table 2), aged 4 months–16 years, mean 10 years; 56/120 (47%) had previously received BCG. Of these 120, six (5%) were QFG positive, and seven (6%) indeterminate (table 3). All but one of those with non-tuberculosis mycobacterial lymphadenitis (NTBML) were QFG negative, with one indeterminate, and two out of three with BCG lymphadenitis were negative, and one indeterminate.
Complete clinical details including concurrent Mantoux result were found for 108/120, 11 had no Mantoux result available, and one had QFG performed a long time after Mantoux and treatment for TB disease (fig 1). Of the 46 Mantoux-positive children, five (11%) were also QFG positive. Of the 62 Mantoux negative, one (2%) was QFG positive.

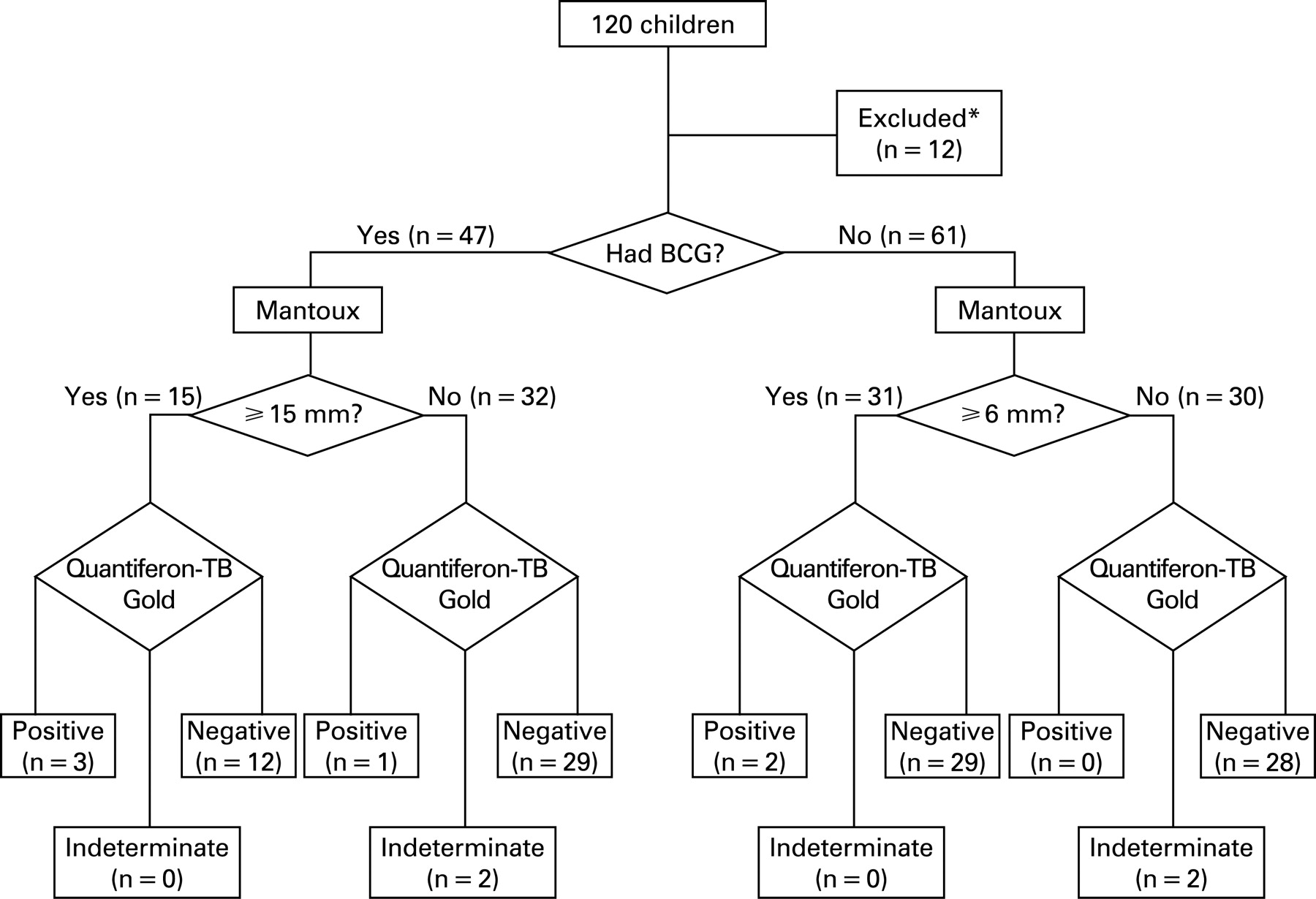{kind=link}
QFG and Mantoux results were the same in 32/45 (71%) cases with prior BCG, and 30/59 (51%) without BCG and in 60% overall. Discordant results included 41 (39%) Mantoux-positive but QFG-negative children and one (1%) Mantoux-negative, QFG-positive child.
Seven (6%) had indeterminate results, five of these seven were under 5 years (table 3). Indeterminates were found in two out of seven (29%) of under 2 years olds, three out of 10 (30%) of under 3 year olds and five out of 18 (28%) under 5 year old. However, only one, a 12-year-old child, was tested as part of contact tracing. Four children were re-tested, two were QFG negative, two remained indeterminate.
Audit of local current practice and NICE guidelines
Actual and expected outcomes for 103 children who were seen as part of TB screening and for whom both QFG and Mantoux results were available were compared (table 4). Local guidelines were followed in 99/103 (96%) cases; two children were discharged when guidelines suggested chemoprophylaxis, and two who should have been given BCG were lost to follow up.
Had NICE guidelines been followed QFG tests would have been offered to 51/103 (49%); five (10%) of whom were QFG positive, one (1%) QFG indeterminate. There would have been no difference compared to actual outcome in 80/103 (78%), with three treated for TB, two receiving LTBI treatment, 22 offered BCG and 53 discharged with only information and advice about their TB risk. However, in 23 (22%) outcomes the treatment would have been different; treatment for LTBI was given in 18 where NICE would have given advice and information only, in one advice only was given where NICE recommended LTBI treatment, and two were not given BCG as they were lost to the follow up. Seventeen (85%) fewer LTBI treatments would be given under NICE than actually given.
Lastly, we treated two children for TB where NICE would have given advice only. Both children had prior BCG and were close contacts of a smear-positive TB case. One had a negative Mantoux, thus QFG would not have been offered (and was negative). Hilar lymphadenopathy was noted on CXR, but neither CXR nor a full examination was advised by NICE. The other had a positive Mantoux (29 mm), but a negative QFG hence CXR and again a full examination would not be advised by NICE; CXR was abnormal with hilar lymphadenopathy and consolidation.
DISCUSSION
This is the first study to evaluate the potential effect of the new NICE diagnosis guidelines on current paediatric practice.
Applying algorithms retrospectively gives a realistic indication of expected outcomes; the specific guidelines used for screening for TB in our clinic are extremely well adhered too, and any new guidelines would be equally well followed.
Had NICE guidelines have been followed, 85% fewer children would have been given chemoprophylaxis for LTBI after contact with TB. This would make a significant reduction in prescribing costs and unnecessary treatment for children. Nevertheless two children treated for TB would have been “missed”. However neither was unwell despite significant CXR changes, and it is not certain that they had TB. This reflects the difficulties in diagnosing primary TB in children, and a trial of treatment is often part of the diagnostic process.
Indeterminate results were less frequent than recently reported8–10, and at 1% of those seen in the context of community TB screening, they make the QFG test a feasible routine test. Indeterminates were more common in the younger child, although this may also be because of confounding factors such as immunosuppression.8
The Mantoux test is well recognised as having good sensitivity and specificity for TB disease, but in a low prevalence population it has a positive predictive value as low as 0.27.11
IFNγ tests are at least as sensitive and specific as Mantoux tests in adults.4 There is far fewer data on their use in children, although an ELISPOT IFNγ test has shown 83% sensitivity for children from South Africa, with 73% in HIV-positive children.5 As recognised by NICE within their guidelines, prospective studies have yet to be published to determine what proportion of IFNγ-test-negative children go on to develop clinical disease.
However IFNγ results do correlate better with risk factors and degree of exposure in contacts of MTB than the TST does.6 7 12 This suggests a better positive predictive value for IFNγ tests than TSTs in low-prevalence populations. This explains the high false-positive TST rate in these populations and a low positive agreement between tests, as seen in our population. Conversely a recent study in a high TB prevalence area suggested that the TST correlated better than an IFNγ test with recent exposure.13
The Mantoux test remains an effective screening tool with proven benefits; treating LTBI on the basis of TST results decreases the risk of active TB by 60%.14 The potential decrease in false-positive Mantoux results with the introduction of IFNγ tests will significantly decrease the amount of LTBI treatment given to children in contact with TB.
Within NICE guidelines there is a reliance on the superiority of QFG over Mantoux; however, without a gold standard to determine the absolute sensitivity and specificity of QFG in LTBI, it is difficult to tell with how much confidence we can discharge children without treatment on the basis of QFG results. Clinical judgement should be used in interpreting results to ensure the best management outcome for the child.
What is already known on this topic
UK guidelines for testing people in contact with infectious tuberculosis are well established.
NICE guidelines, introduced in 2006, recommend the inclusion of an IFNγ blood test in the assessment of contacts of tuberculosis. Treatment is considered on the basis of a positive IFNγ test rather than a positive Mantoux test.
What this study adds
Specific guidelines used for screening for TB are extremely well adhered too, and any new guidelines would expect to be equally well followed.
Nearly half of children screened for tuberculosis would have an IFNγ test recommended when using NICE guidelines.
Following NICE guidelines would result in 85% fewer children being given treatment for LTBI after contact with TB.
Acknowledgments
We appreciate the assistance of Elspeth Gould and Anne Black CDCN (TB), HPA, in the children’s contact tracing clinic. Thanks for providing a QFG clinical service to Anne Barrett and Julie Dunn, Regional TB reference Laboratory, HPA North East, Newcastle Laboratory, Newcastle General Hospital, Westgate Road, Newcastle-upon-Tyne, NE4 6BE. Thank you to Dr S Hackett and Dr A Fall for reviewing with helpful comments and suggestions.
REFERENCES
Footnotes
Competing interests: None.
Funding: None.
Linked Articles
- Atoms
- Perspectives