Article Text

Abstract
BACKGROUND Acute asthma is associated with elevated serum concentrations of products of activated T cells and eosinophils.
AIMS To compare the changes in concentrations of these products with disease severity and changes in lung function following oral prednisolone treatment.
METHODS Twenty patients (mean age 8.7 years) were recruited on admission with acute asthma to a district general hospital. Disease severity was recorded before and after treatment with oral prednisolone using a validated pulmonary index score. Serum concentrations of interleukin (IL)-4, IL-5, soluble (s)CD25 (soluble IL-2 receptor), using a specific enzyme linked immunosorbent assay, and eosinophil cationic protein (ECP), using radioimmunoassay, were measured concomitantly. Non-asthmatic children (n = 6, mean age 9.2 years) undergoing elective surgery were recruited as controls, and serum samples were obtained on one occasion without treatment. Main outcome measures were changes in serum concentrations of cytokines and ECP, clinical asthma severity score, and peak expiratory flow rate.
RESULTS As expected, oral glucocorticoid treatment in the children with asthma was associated with clinical improvement and also with significant reductions in serum concentrations of IL-5 (mean 5.59 to 2.19 pg/ml, p = 0.0001), sCD25 (mean 2236 to 1772 pg/ml, p = 0.002), and ECP (mean 54.3 to 33.1 pg/ml, p = 0.0001). Serum IL-4 concentrations, in most patients and all the controls, remained below the sensitivity of the assay. However, serum concentrations of IL-5, sCD25, and ECP remained significantly higher than in controls, even after treatment with oral glucocorticoids (p = 0.03).
CONCLUSIONS These data suggest that T cell mediated inflammation may persist in childhood asthma despite apparent clinical remission associated with conventional doses of prednisolone. The long term consequences of persistent inflammation after an apparently treated acute attack of asthma require clarification. Clinical assessment and pulmonary function are inadequate surrogates for airway inflammation.
- asthma
- cytokines
- eosinophil cationic protein
- prednisolone
- lung
- airway inflammation
Statistics from Altmetric.com
In the past decade, bronchial biopsy and bronchoalveolar lavage in adult asthma have led to the concept that bronchial mucosal inflammation plays a fundamental role in the pathogenesis of asthma. This inflammation is characterised by T cell activation and airway eosinophilia.1 Local release of eosinophil granule proteins, of which eosinophil cation protein (ECP) is prototypical, is thought to cause bronchial mucosal damage and, ultimately, reversible airway obstruction and bronchial hyper-responsiveness.2The influx of eosinophils is thought to be mediated by local release of eosinophil active cytokines by activated T cells, of which interleukin (IL)-5 is the most important.3 ,4 IL-5 acts specifically on eosinophils, bringing about their recruitment and activation, and promoting their enhanced survival. IL-4, another product of activated T cells, may also play a role in eosinophil recruitment, as well as being one of only two cytokines known to initiate IgE synthesis in B cells, suggesting a further fundamental role for this cytokine in the pathogenesis of asthma.5 Glucocorticoids powerfully inhibit T cell activation and cytokine secretion, and this is probably one of the principal mechanisms by which they ameliorate asthma.6
We have previously shown elevated percentages of T cells expressing activation markers and mRNA encoding IL-4 and IL-5 in the peripheral blood of both adults and children with asthma as compared with controls.7-10 Other groups have shown elevated concentrations of the soluble form of CD25 (sCD25), released by activated T cells,11 ,12 and ECP13 in the serum of asthmatic adults and children compared with controls. Some of these studies have suggested a correlation between the concentrations of these products and disease severity, highlighting the possible role of these markers as simple objective measures to monitor disease activity and response to treatment.
In this study we wished to extend our previous observations on the properties of T cells and eosinophils in the peripheral blood of children with asthma, by measuring serum concentrations of their products during acute exacerbations, and changes in serum concentrations following oral gluccorticoid treatment. We hypothesised that serum concentrations of sCD25, IL-5, IL-4, and ECP would be elevated, compared with controls, during acute exacerbations in children with asthma, and that these concentrations would normalise concomitantly with systemic glucocorticoid treatment and clinical improvement. We measured the concentrations of these proteins in the serum of a group of children with moderate to severe asthma, before and after five days of oral prednisolone treatment, while monitoring lung function and clinical severity score. We also measured serum concentrations in controls matched, as far as possible, for age and atopic status.
Methods
SUBJECTS
Twenty children (14 boys, six girls; mean age 8.7 years, range 5–14 years) known to have asthma and admitted to a district general hospital with an acute exacerbation formed the study group. We were not able to perform viral or other studies to determine the cause of the acute exacerbation. Sixteen of these children were atopic (see definition below). Exclusion criteria included a history of chronic lung disease such as bronchopulmonary dysplasia, cystic fibrosis, or other definite systemic disease, presence of stridor, suspicion of foreign body inhalation, or use of systemic steroids within the previous 24 hours. After clinical examination the children were assigned a pulmonary index disease severity score based on pulse rate, respiratory rate, usage of accessory muscles of respiration, presence or absence of audible wheeze, oxygen saturation in room air, and peak expiratory flow rate. For each of these six measurements or observations, a score of 1–3 was assigned (table 1), resulting in a possible minimum score of 6 (normal) and maximum score of 18. Scores were assigned on admission, and seven days later, by a single observer (A S E-R) before any laboratory measurements were made. All children were treated with oral prednisolone 2 mg/kg/day (maximum 40 mg/day) for five days and with oxygen and inhaled β2-agonist as required. None required intravenous treatment or antibiotics.
Derivation of pulmonary index score for asthma severity
CONTROLS
Six healthy children (two boys, four girls; mean age 11 years, range 7–16 years), who required a blood test in the course of minor elective surgical procedures, were recruited as controls. Two of these children were atopic. No child had any previous symptoms of asthma.
ETHICS
This study was approved by the research ethics committee at Queen Mary's Hospital, Sidcup. Informed written consent was obtained from parents or guardians for their children to participate in the study.
DEFINITION OF ATOPY
For the purposes of this study, atopy was defined as a positive skin prick test (wheal diameter > 4mm at 15 minutes) to extracts of three common aeroallergens (mixed grass pollen, cat dander, house dust mite: Soluprick; ALK, Horsholm, Denmark) and/or a serum IgE concentration > 150 IU/ml (PRIST; Pharmacia, Uppsala, Sweden).
BLOOD SAMPLING AND MEASUREMENT OF SERUM ANALYTES
Peripheral venous blood (3–5 ml) was drawn from the children with asthma at admission before glucocorticoid treatment, and again after five days of treatment at about the same time of day. A single sample was drawn from the control subjects. Blood was allowed to clot on plain glass for one hour at 20°C, after which serum was recovered by centrifugation and stored at −80°C pending analysis. Serum concentrations of IL-5, IL-4, and sCD25 (soluble IL-2 receptor) were measured by commercial sandwich enzyme linked immunosorbent assay (ELISA) calibrated with recombinant human standards (R&D Systems, Abbingdon, Oxon, UK). The assays were sensitive above 1.8 pg/ml (IL-5), 0.012 pg/ml (IL-4, high sensitivity assay), and 56 pg/ml (sCD25). Serum ECP concentrations were measured with a commercial radioimmunoassay kit (Pharmacia) sensitive above 2 pg/ml. Samples were diluted, where necessary, so that all measurements fell within the ranges of the standard curves. For each analyte, duplicate measurements were made contemporaneously in the same assay.
STATISTICAL METHODS
Statistical comparisons were made between serum concentrations of cytokines before and after prednisolone treatment using Student's paired t test. This test was also used to compare changes in peak expiratory flow rates and asthma severity scores. The non-parametric Wilcoxon signed ranks test was used to compare serum ECP, sCD25, and IL-5 concentrations between patients and controls. The p values shown in fig 3 are derived from Pearson's linear regression analysis.

Relation between serum concentrations of interleukin-5 (IL-5), soluble CD25 (sCD25), and eosinophil cationic protein (ECP) and severity scores in the children with asthma on admission. All measurements are in pg/ml. p values by Pearson's linear regression.
Results
CLINICAL RESPONSE OF PATIENTS WITH ASTHMA TO TREATMENT
In the children with asthma, the mean (SEM) severity score was 11.2 (2.3) on admission. After one week, most patients were essentially asymptomatic (mean score 6.1 (0.4)). The mean (SEM) peak expiratory flow rate in the children with asthma was 41 (6)% of the predicted value on admission and 88 (3)% after one week. Both of these changes were significant (fig 1).
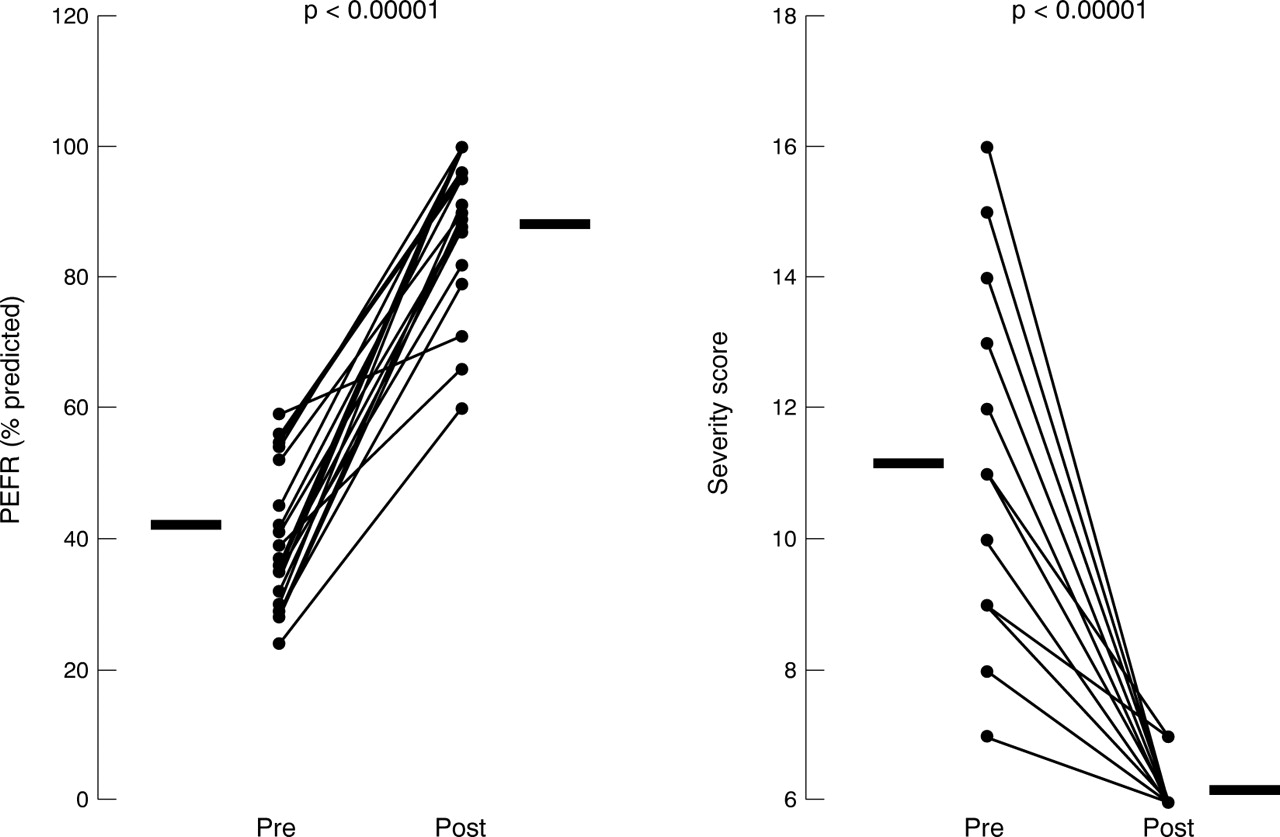
Changes in peak expiratory flow rate (PEFR, % predicted) and asthma severity scores in the 20 children with acute severe asthma before (Pre) and after (Post) oral prednisolone treatment. Bars represent mean values. Statistical comparisons by paired t test.
SERUM ANALYTE CONCENTRATIONS
IL-5
IL-5 was detectable in the serum of all 20 children with asthma on admission, but undetectable using the same assay in all six controls. Prednisolone treatment was associated with a significant reduction in serum IL-5 concentration (5.59 (0.71) to 2.19 (0.18) pg/ml, p = 0.0001; fig 2, table 2), which nevertheless remained significantly elevated at the end of the study compared with that of the controls (2.19 (0.18) pg/ml vundetectable, p = 0.03; table2).

{kind=link}
{kind=link}
{kind=link}
Serum concentrations of interleukin (IL)-5, IL-4, soluble CD25 (sCD25), and eosinophil cationic protein (ECP) in 20 children with acute severe asthma before (Pre) and after (Post) a course of oral prednisolone (2 mg/kg/day; five days) and six non-asthmatic controls. Bars represent mean values. Statistical comparisons by paired t test.
Serum analyte concentrations in children with asthma before and after oral prednisolone treatment, and the normal controls
IL-4
Even with the use of a high sensitivity ELISA, IL-4 was detectable in the serum of only a minority of the patients with asthma on admission, and was undetectable in all of the controls. In three patients, prednisolone treatment was associated with a measurable increase in serum IL-4 concentrations, but in the majority IL-4 remained low, and the changes in the group as a whole were not statistically significant (fig 2, table 2).
sCD25 (sIL-2 receptor)
sCD25 was detectable in the serum of all 20 children with asthma on admission and also in all six controls (fig 2, table 2). Prednisolone treatment was associated with a significant reduction in serum sCD25 concentrations (2236 (192) to 1772 (175) pg/ml, p = 0.002), which nevertheless remained elevated compared with the controls even after treatment (1172 (175) pg/mlv 506 (34) pg/ml, p = 0.03; table 2).
ECP
ECP was detectable in the serum of all 20 children with asthma on admission and also in all six controls (fig 2, table 2). Prednisolone treatment was associated with a significant reduction in serum ECP concentrations (54.3 (4.7) to 33.1 (3.7) pg/ml, p = 0.0001), which nevertheless remained elevated compared with the controls even after treatment (33.1 (3.7) pg/ml v 15.5 (1.9) pg/ml, p = 0.03; table 2).
CORRELATION OF CLINICAL SEVERITY SCORE WITH ANALYTE CONCENTRATIONS
In the patients with asthma on admission, clinical severity score correlated with serum concentrations of IL-5 (r 2 = 0.73, p = 0.017), sCD25 (r 2 = 0.84, p = 0.007), and ECP (r 2 = 0.85, p = 0.005) (fig 3). There was no significant correlation between IL-4 and clinical severity score.
Discussion
We show in this study that the concentrations of the asthma relevant cytokine IL-5, the T cell activation marker sCD25, and the prototypical eosinophil degranulation product ECP are elevated in the serum of children with acute severe asthma compared with controls. Furthermore, we show that the concentrations of these mediators are reduced in association with glucocorticoid treatment and clinical improvement. These data cannot prove a causal relation between the release of T cell and eosinophil mediators and the regulation of asthma severity. They are consistent with the hypothesis that acute severe asthma in children is associated with increased IL-5 release by activated T cells, which in turn results in enhanced eosinophil degranulation. Our observed correlations between disease severity on admission and serum concentrations of these mediators further support this concept.
It may be thought surprising that we were unable to detect IL-4 in the serum of most of our asthmatic patients despite using a high sensitivity assay. Increases in serum IL-4 concentrations were seen in three of these patients following glucocorticoid treatment, but the changes in the group as a whole were not significant. In a large study14 comparing atopic and non-atopic children of different ages, IL-4 was only increased in the serum of the atopic children, as compared with the controls, when a high sensitivity ELISA was used, but there was no correlation with the presence and severity of asthma. Two further studies on adults15 and children16 have shown essentially similar results. Overall, these data suggest that serum IL-4 concentrations may be slightly elevated in atopic patients compared with non-atopic controls, irrespective of whether or not they have asthma. Even so, direct correlations between serum IL-4 and total IgE concentrations in these patients, where sought,14 ,15 have not been found. It is possible that inappropriate IgE synthesis may not require continuous elevated IL-4 synthesis, at least as reflected by serum concentrations.
The main point of interest in this study is that the serum concentrations of these asthma relevant analytes were still clearly elevated in the children with asthma compared with normal controls even after treatment resulting in resolution of all signs and symptoms as judged by clinical and spirometric criteria. The clinical significance of this finding is unclear. It may be that these serum inflammatory changes resolved spontaneously within a few days. This could be investigated by a further study taking serial blood samples, although this may not be considered ethical. These data suggest that more prolonged intensive anti-inflammatory treatment may be warranted in acute exacerbations of childhood asthma. Further clinical and immunological studies are required to investigate the long term consequences of apparently untreated inflammation. However, this study does highlight the deficiencies of relying on clinical assessment and pulmonary function to monitor an inflammatory airway disease such as asthma, and the response to treatment with anti-inflammatory medication.
Cysteinyl leukotrienes are mediators that are also believed to be important in the pathogenesis of asthma. Of interest and in accord with the findings of our study was a report that plasma leukotriene B4 and urinary leukotriene E4 were increased in acute asthma,17 and fell in association with oral corticosteroids, but remained significantly above normal one month later, again implying continuing inflammation despite an apparently adequate clinical response.
More importantly, this study has shown that, despite the usual course of prednisolone for acute asthma, there is evidence of continuing airway inflammation despite resolution of symptoms and normalisation of pulmonary function.
Acknowledgments
This study was funded partly by the National Asthma Campaign and the Medical Research Council (UK).