Article Text

Abstract
Objective: To determine the effect of adenoidectomy and/or tonsillectomy (“adenotonsillectomy”) upon growth and growth biomarkers, in the context of sleep disordered breathing (SDB). SDB in children, primarily due to adenotonsillar hypertrophy, increases the risk of growth failure.
Design: Systematic review and meta-analysis. PubMed, ERIC and Cochrane Reviews databases from January 1980 to November 2007 were searched for studies reporting: pre/post-adenotonsillectomy height and weight changes as percentage increased or decreased, raw data, z scores or centiles, or: IGF-1 and/or IGFBP-3 serum-level changes as z scores or raw data. For anthropometrics, the meta-analysis included studies presenting z scores or centiles.
Setting: Observational studies.
Patients: Otherwise healthy children, not selected for obesity.
Main outcome measures: Pre/post-surgery changes in standardised height and weight, and IGF-1 and IGFBP-3.
Results: Of 211 citations identified, 20 met systematic review criteria. SDB was an enrolment criterion in 13 of the studies, and one of several enrolment criteria in three. Meta-analysis findings for pre/post-surgery changes were: standardised height: 10 studies, 363 total children, pooled standardised mean differences (SMD) = 0.34 (95% CI 0.20 to 0.47); standardised weight: 11 studies, 390 total children, pooled SMD = 0.57 (95% CI 0.44 to 0.70); IGF-1: 7 studies, 177 total children, pooled SMD = 0.53 (95% CI 0.33 to 0.73); IGFBP-3: 7 studies, 177 total children, pooled SMD = 0.59 (95% CI 0.34 to 0.83).
Conclusions: Standardised height and weight, and IGF-1 and IGFBP-3 increased significantly after adenotonsillectomy. Findings suggest that primary care providers and specialists consider SDB secondary to adenotonsillar hypertrophy when screening, treating and referring children with growth failure.
Statistics from Altmetric.com
Since the 1980s, case reports1–4 and case series5 suggest that sleep disordered breathing (SDB),6–8 which is characterised by snoring, mouth breathing and obstructive sleep apnoea,9–13 is a risk factor for growth failure. SDB affects an estimated 4%–20% of children,14–17 while 1%–3% experience obstructive sleep apnoea.15 16 Pre-school aged children experience even higher rates of SDB. Among 3–6-year-old children, 35% habitually snore, while 19% had reported obstructive sleep apnoea18; 25% of 5-year-old children in another sample had SDB.19
What is already known on this topic
Sleep disordered breathing in children, secondary to adenotonsillar hypertrophy, is often cited as a risk factor for growth failure.
Increases in weight, height, IGF-1 and/or IGFBP-3 are noted after adenotonsillecomy.
However, small sample sizes (all but one study have included <100 children) do not permit inferences about the magnitude of these changes.
What this study adds
This is the first systematic review and meta-analysis of the literature on growth or growth biomarker changes after adenotonsillectomy.
Most of the studies we reviewed had sleep disordered breathing as an inclusion criterion.
Our meta-analysis of these studies found significant increases in weight and height z scores, and IGF-1 and IGFBP-3 serum levels.
Our findings suggest that primary care providers and specialists should consider sleep disordered breathing when they screen, treat and refer children with growth failure.
Adenotonsillar hypertrophy is the primary factor associated with SDB in children. SDB peaks at 2–6 years of age, given the relative adenotonsillar hypertrophy during this period.20 Tonsillectomy and adenoidectomy (“adenotonsillectomy”) is curative in 80% of cases21 22 and resolves the common clinical symptoms of SDB.23 24 In case studies and case series of referred children, those who undergo adenotonsillectomy as an intervention for SDB show, as a corollary benefit, catch-up growth after the procedure.6 25–30
Several possible mechanisms might explain a relationship between SDB and growth failure. SDB interrupts slow-wave sleep, when growth hormone is preferentially secreted8 31; this is a prime posited pathway from SDB to growth failure. Even chronic snorers not meeting criteria for obstructive sleep apnoea have abnormal electro-encephalograms, with prominent abnormalities in slow-wave sleep.32 Growth failure is related to serum levels of insulin-like growth factor-1 (IGF-1) and IGF-binding protein 3 (IGFBP-3),33 34 both of which are highly correlated with diurnal growth hormone secretion and reflect mean daily growth hormone levels.35 36 SDB can lead to growth failure via increased energy expenditure during sleep,27 37 or pharyngeal dysphagia from adenotonsillar hypertrophy, which can elicit pain and obstruct food entry, thus reducing appetite.38 39 SDB is also associated with increased motor activity during the day,40 which may potentially increase energy expenditure and thus contribute to growth failure.
Apart from growth failure, SDB is associated with a range of neurobehavioral and cardiovascular complications.41–45 Despite the range of risks associated with SDB, few paediatric primary care providers screen for it,46 and just 50% are aware of any potential link to growth failure.47 As a result, children with SDB experience prolonged morbidity and delays in treatment,48 leaving untreated the sequelae of persistent SDB.41
We (a) systematically reviewed the literature on changes in height, weight, IGF-1 and/or IGFBP-3 before and after adenotonsillectomy surgery in otherwise healthy children, and (b) performed a meta-analysis of such standardised changes. We sought to expand upon prior (non-systematic) reviews of data related to growth failure and SDB.49–52 The sole report of sleep disorders in children selected for growth failure53 focused on non-SDB sleep disorders (eg, insomnia) in 158 non-growth hormone deficient endocrine clinic patients. Children referred for adenotonsillectomy surgery are a subpopulation of those with SDB, but the public health consequences of the effects of SDB upon growth are not limited to them.
There are complex interactions between obesity and SDB. Obesity is associated with an increased prevalence of SDB in children and adults,54 while SDB has been associated with alterations in serum concentrations of adipokines, including leptin,55 which in turn alters ventilatory responses in SDB.56 Obesity is associated with alterations in growth velocity. Obesity and SDB have co-morbidities, including insulin resistance and cardiovascular risk that may be mediated through common pathways, including systemic inflammation.57 Therefore, we reasoned that obesity may confound any relationships between SDB and growth failure and chose instead to focus this review on non-obese children.
METHODS
The population of interest was otherwise healthy children, from birth through 18 years of age, undergoing adenotonsillectomy surgery primarily for recurrent infection and/or SDB symptoms.
Search strategy and study selection
We searched Medline, ERIC and Cochrane Reviews for papers from 1 January 1980 to 15 November 2007 on changes in height, weight, IGF-1 and/or IGFBP-3 before and after tonsillectomy, adenoidectomy or both (“adenotonsillectomy”). Search terms included the following three domains of key words: (1) “failure to thrive”, “short stature”, “height”, “growth”, “growth failure”, “growth delay” or “growth impairment” paired with (2) either “adenotonsillectomy”, “tonsillectomy” or “adenoidectomy” and (3) either “sleep disordered breathing” or “obstructive sleep apnoea”.
For the systematic review, we included studies that provided an original, empirical summary or raw data on pre- and post-operative adenotonsillectomy changes (if any) in otherwise healthy children for one or more of the following outcomes: height, weight, IGF-1 or IGFBP-3. Papers were included if they reported (a) anthropometric changes as z scores, age- and sex-adjusted weight-for-height or height-for-age centiles, raw data, or as percentage increased or decreased or (b) raw or z score changes in serum levels of IGF-1 or IGFBP-3.
Excluded from the systematic review were: (a) case studies, (b) studies of children with conditions potentially affecting growth, dietary intake or respiration (eg, extremely low birth weight, craniofacial abnormalities), (c) studies specifically excluding children with suspected SDB, (d) studies specifying obesity as an inclusion criterion, or focus, given the potential for confounding, (e) articles that did not provide English language abstracts, and (f) foreign language (only) articles with incomplete outcomes data in their English language abstracts.
For the meta-analyses of height and weight, we restricted the sample to those studies meeting the above criteria that also provided either z scores or centiles (that could be translated to z scores under the assumption they were normally distributed) for anthropometrics before and after adenotonsillectomy, and standard deviations of differences or corresponding test statistics. Relevant descriptive and inferential statistics from these publications were compiled and then reviewed by an independent reviewer in preparation for analysis.
Data extraction
Two reviewers (KB and JH) independently completed a standardised data extraction form for studies that met initial systematic review criteria. Any differences were resolved by re-examination of the paper. A third reviewer (KF) adjudicated any remaining differences via independent review of findings with discrepant outcomes, and reviewed the appropriateness of all data prior to analysis.
The data extraction form included the following domains: (a) citation, (b) sample size, (c) measure of central tendency and dispersion for age, (d) duration of follow-up, (e) outcomes assessed, (f) indication of excess growth failure in sample, as evidenced by age- and sex-adjusted weight and/or height prior to adenotonsillectomy (ie, the proportion below the 5th centile), (g) whether SDB was the only criterion, one of several criteria or not mentioned with regard to sample selection, and (h) whether data were obtained from the English language abstract of a foreign language article.
Statistical analysis (meta-analysis)
For studies that provided growth parameters expressed as centiles, we translated centiles into z scores by assuming the centiles followed a t distribution. Using the corresponding degrees of freedom for this paired design, the z score was approximated by the t statistic that cut off the proportion of the area under the curve reflecting the centile. For studies in which only means, standard deviations at each time point, and p values were provided, the standard deviation of the difference was derived using the formula for the t test statistics for paired differences; the mean difference, sample size and critical t statistic for the appropriate number of degrees of freedom for the p value were substituted into the formula, and the standard deviation of the difference was derived.
Standardised mean differences (SMD) were computed as the difference in means post minus pre divided by the standard deviation of the difference. A fixed effects model was assumed, and the standard error of the mean difference of each study was computed along with corresponding 95% confidence intervals. For calculating the pooled SMD, the weight for each study was devised as the reciprocal of the variance of the SMD, and the pooled estimate of SMD was the average of the products of the SMD multiplied by the corresponding weight. The pooled SMD standard error of the mean difference was used to derive the 95% confidence interval for the pooled estimate of the SMD. Forest plots for height, weight, IGF-1 and IGFBP-3 differences from pre to post are presented.58 The significance of heterogeneity is derived by squaring the difference between the individual study effect and the pooled effect, weighting that by the reciprocal of the variance of the study effect, and summing these products; the sum has a χ2 distribution with k−1 df where k is the number of studies.
RESULTS
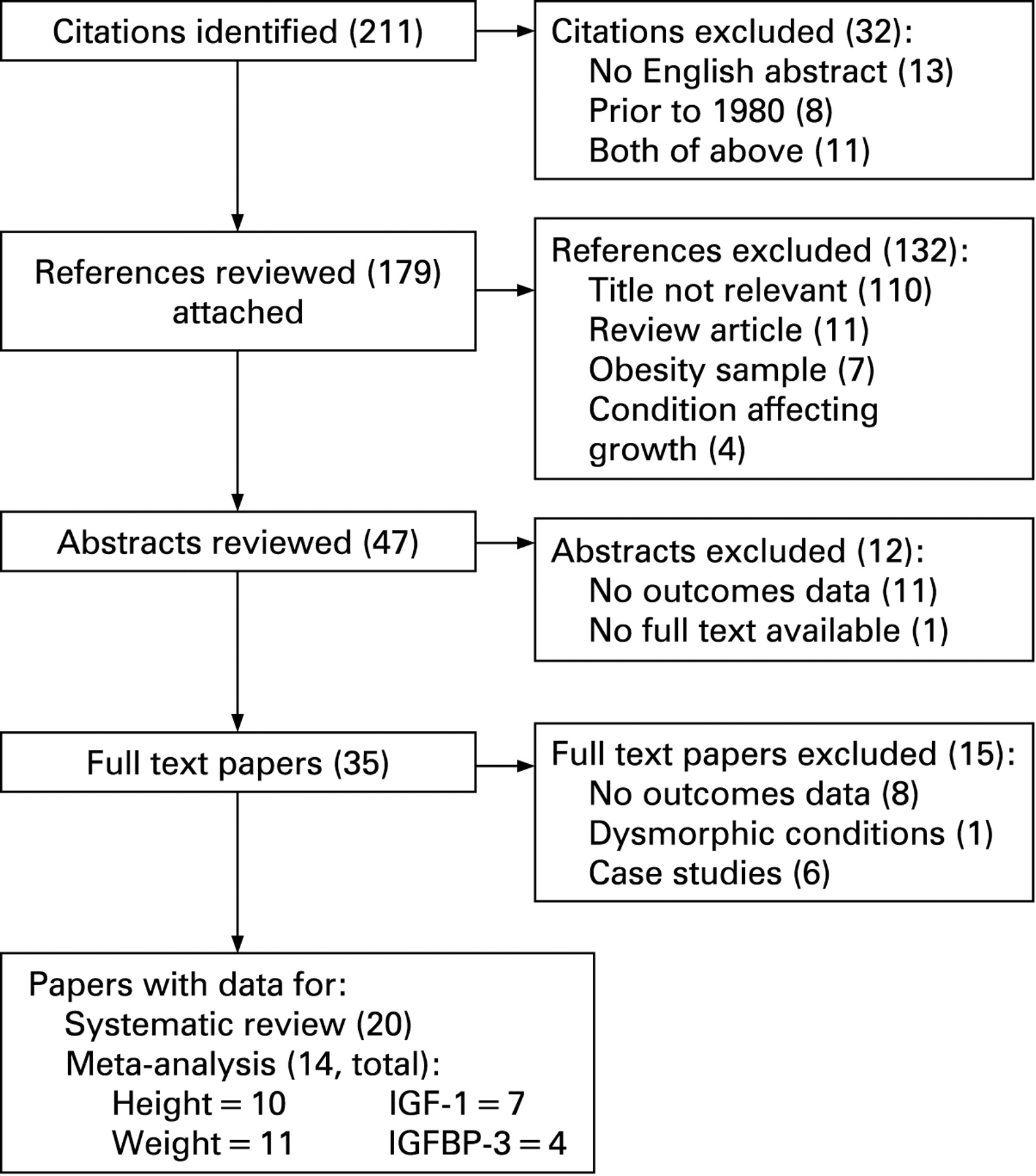
A total of 211 citations were initially identified. Figure 1 presents a flowchart of titles, abstracts and full text papers not meeting inclusion criteria for the systematic review and meta-analysis.

Systematic review
The 20 papers meeting systematic review criteria are described in table 1.59–62 These 2063–82 cohort studies ranged in size from 14 to 204 children with pre/post-data, spanned the ages of 5 months to 15.8 years, and had follow-up periods of 1 month to 3 years. Most children (n = 16) were selected from otorhinolaryngology (“ENT”) services, while three were from sleep centre patients. Excess growth failure at baseline was found in seven studies.
Underscoring the role of SDB, 16 studies included SDB as either a criterion for enrolment in the sample (n = 13) or one of several criteria (n = 3). Of note, seven studies employed objective assessments of SDB, such as polysomnography or capnography. The remaining studies identified SDB via clinical exam, parental report and/or questionnaire.
Regarding height, of the 10 studies included in the meta-analysis, seven presented z scores, while in three, height z scores were derived from centiles. Height was not assessed in five studies. The remaining five studies, which provided descriptive data insufficient for deriving a z score, reported excess height gain versus expected (p<0.05),63 increased height z score (no p value),65 increased height centile for 8/65 children,74 resolution of failure to thrive in 10/24 children (pre-surgery, 19/24 had height <3rd centile),77 and no increase in height centile (no p value).68
Regarding weight, of the 11 studies included in the meta-analysis, eight presented data as z scores, while in three, z scores were derived from centile data. Another eight studies, providing descriptive data which were insufficient for deriving a z score, reported weight gain versus expected (p<0.05),63 resolution of underweight in 6/22,66 20% with excess weight gain (no p value),67 increased weight gain velocity (no p value),68 12% with “greater than expected” weight gain (p<0.01),69 weight-for-height percentage increases,73 increased centiles for 25/65 children,74 and failure to thrive resolved in 10/24 children (pre-surgery, 19/24 had weight <3rd centile).77 Weight was not assessed in one study. Efforts to contact authors of studies with insufficient data for deriving z scores were unsuccessful.
Regarding IGF-1, seven studies provided primary pre/post-surgery data for IGF-1. Of these, one presented standard deviation score based upon national reference values.83 Of the seven, four also provided IGFBP-3 data, with the above-cited study providing this as a z score. Two additional studies of IGFBP-3 did not provide sufficient data for inclusion in the meta-analysis but indicated no significant differences in serum levels post-surgery.
Meta-analysis
Height
The meta-analysis for differences in pre to post height is based upon data from 10 studies, totalling 363 children (fig 2). The pooled SMD for height was statistically significant: pooled SMD = 0.34 (95% CI 0.20 to 0.47). In these 10 individual studies, the SMD favoured height increases in eight, although in six studies, the 95% CI for the SMD included 0 and thus was not significant. In eight of these 10 studies, SDB was a criterion for inclusion in sample selection (268/363 children), in one study SDB was one of several criteria, and in one study SDB status was unspecified.

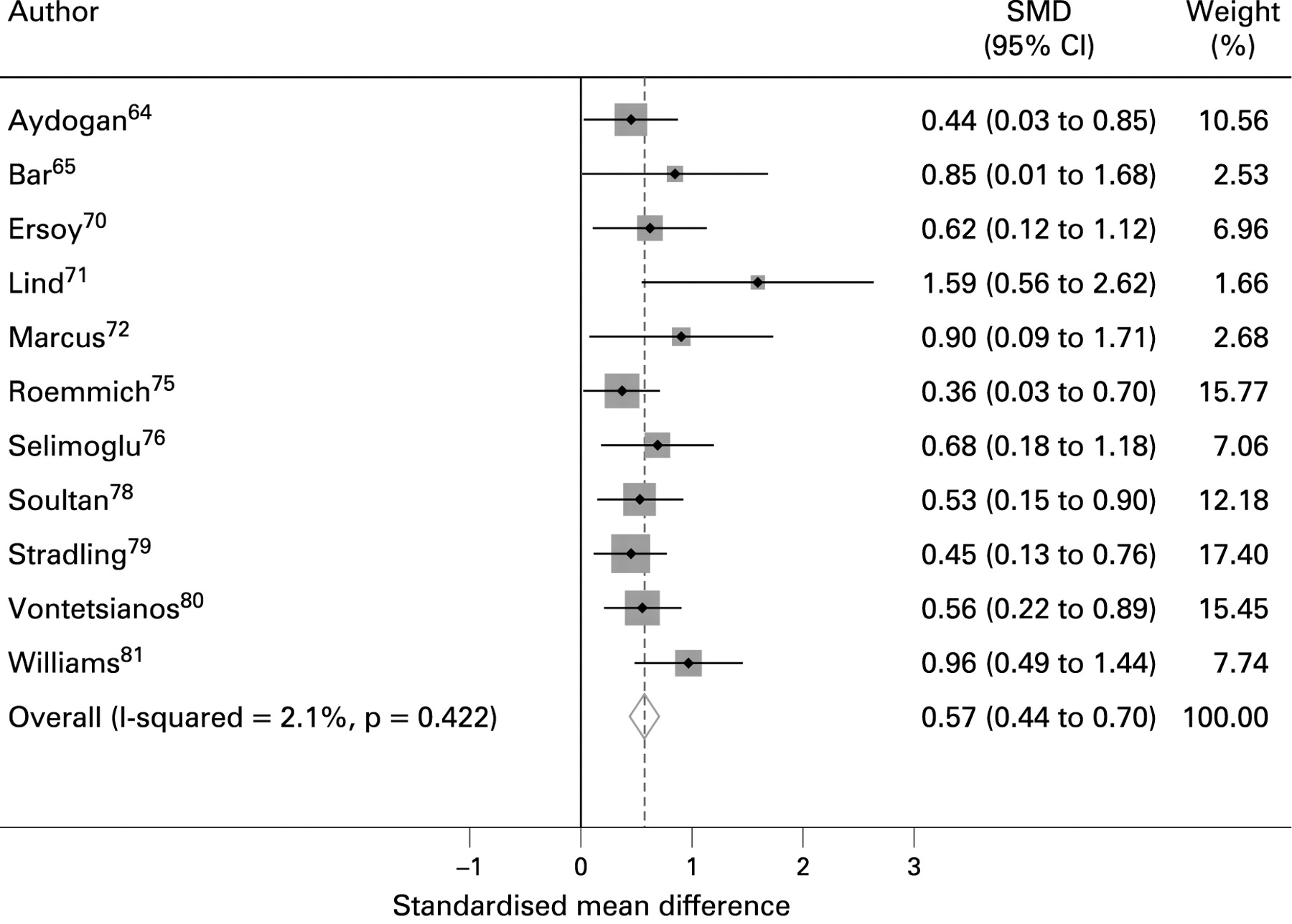
Weight
The meta-analysis for differences in pre to post weight is based upon data from 11 studies, totalling 390 children (fig 3). In all 11 of these individual studies, the SMD favoured weight increases. The pooled SMD for weight was statistically significant: SMD = 0.57 (95% CI 0.44 to 0.70). In nine of these 11 studies, SDB was a criterion for inclusion in sample selection (295/390 children), in one study SDB was one of several criteria, and in one study SDB status was unspecified.

IGF-1
The pooled SMD for IGF-1 was significant: SMD = 0.53 (95% CI 0.33 to 0.73). In five of these studies (82/177 children), SDB was a criterion for inclusion in the sample. In all seven individual studies, the SMD favoured IGF-1 increases, although in two studies this increase was not statistically significant as the 95% CI included 0 (fig 4).

IGFBP-3
The pooled SMD for IGFPB-3 was statistically significant: SMD = 0.59 (95% CI 0.34 to 0.83). In all four individual studies the SMD favoured IGFBP-3 increases. However, in two studies, the 95% CI encompassed 0 (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
This is the first systematic review and meta-analysis of data suggesting a relationship between SDB (secondary to adenotonsillar hypertrophy) and growth failure in children. Our meta-analysis found significant increases in both standardised height and weight following surgery. Pooled data from 10 studies on height yielded a significant z score increase of 0.34 (95% CI 0.20 to 0.47). For weight, pooled data from 11 studies yielded a significant z score increase of 0.57 (95% CI 0.44 to 0.70). These findings are supported by anthropometric outcomes from studies not meeting our criteria for inclusion in the meta-analysis; 4/5 reported height increases and 8/8 reported weight increases.
We also found significant increases in IGF-1 and IGFBP-3. However, the implications of these findings are less clear, given that their levels normally increase with age prior to puberty, vary by sex and BMI,84 and that few locally established reference ranges for healthy children exist.85 We note that in the one study with z score data, IGFBP-3 increases were significant but IGF-1 increases were not,64 while in the one study employing non-surgical controls, IGF-1 significantly increased only in the adenotonsillectomy group at follow-up.73 Future research on IGF changes prior to and after adenotonsillectomy, stratified by anthropometrics, growth hormone sufficiency, and other factors affecting growth are needed. Cost further motivates such research: growth hormone treatment averages $15 000–$20 000/year in young children and can exceed $50 000/year in adolescents.86
To place the anthropometric increases in context, the increased weight gain would likely shift a child into the normal range if their centile was less than 5%. Our pooled z score height increase was 0.34, which compares with 0.53 from a meta-analysis of growth hormone treatment for 1 year in children with idiopathic short stature.87 While the two meta-analyses’ samples are not comparable (person-level growth changes were not presented by papers used in our meta-analysis, SDB status was not assessed in growth hormone treatment meta-analysis, etc), our findings are nonetheless compelling. Longer term, adult height gains of 0.8 SD88 and 1.1 SD89 in initially growth hormone deficient children treated with growth hormone are reported; in an 8-year-old girl of average height, our 0.34 SD increase would equal 1.68 cm.90 In contrast to growth hormone treatment, adenotonsillectomy is a one-time intervention. Longer post adenotonsillectomy follow-up of children, stratified by initial growth status, might show greater or lesser effects.
Our findings support the hypothesis of an epidemiological association between SDB and growth failure; approximately 80% of SDB in young children is associated with adenotonsillar hypertrophy.21 22 Although it is possible that adenoidal hypertrophy without SDB could contribute to growth failure, through recurrent infection, inflammatory mechanisms and interference with nutritional intake, there is substantial evidence that SDB is a prime pathway for growth failure in children with adenotonsillar hypertrophy. SDB now surpasses recurrent throat infections as the primary indication for adenotonsillectomy in children.91 92 In 16 of 20 papers reviewed, SDB was either the primary criterion or one of several possible enrolment criteria. Otolaryngologists identify growth failure as an absolute indication for adenotonsillectomy.92 The American Academy of Pediatrics identifies growth failure as a serious complication of untreated obstructive sleep apnoea.93
Unfortunately, the existing literature is limited. No randomised controlled trials of surgery versus no surgery (eg, “watchful waiting”) met our inclusion criteria. Rather, the available observational studies were primarily small, single-site samples of referred children. Publication bias is generally more likely with observational studies versus clinical trials. Wide age ranges within and across samples further limit interpretation, especially given growth acceleration and deceleration shifts throughout childhood. The non-availability of patient level data precluded examining gender and other patient specific effects. Also, follow-up periods varied. It was also difficult to employ a singular definition of growth failure in the systematic review, reflecting a lack of consensus on what constitutes poor growth, particularly in infants and young children,94 95 and poor concurrence among criteria.96 Selection bias in who receives adenotonsillectomy is also a possibility, due to varying criteria used to define SDB.
Neither paediatric primary care providers97–102 nor specialists in genetics,103 gastro-intestinal104 105 or endocrine106 subspecialties routinely include upper airway obstruction, or adenotonsillar hypertrophy, in their differential diagnosis of growth failure in general, or short stature in particular. Our findings suggest that primary care providers and specialists consider SDB when they screen, treat and refer children with growth failure. Our current cohort studies (Sleep disordered breathing and growth in children: a longitudinal cohort study; National Heart, Lung, and Blood Institute grant 1R21HL091241-01A1) in the large, well-characterised Avon Longitudinal Study of Parents and Children are examining individual-level growth changes from birth throughout childhood in the context of SDB symptoms and related confounders.
Acknowledgments
The authors wish to acknowledge Professor Jonathan Sterne for graphic presentation of the forest plots, Ms Jennifer Lischewski for assistance in organising study data and Ms Klil Babin for research assistance.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- Atoms