Article Text

Abstract
Objectives: A gene–environment interaction between HLA-DR shared epitope genes and smoking in anti-cyclic citrullinated peptide antibody-positive rheumatoid arthritis (RA) has been reported. Identification of citrullinated proteins in bronchoalveolar lavage (BAL) cells from smokers has led to the suggestion that citrullination induced by smoking might be the first step in the pathogenic chain of RA.
Objective: To confirm and extend these findings.
Methods: Immunohistochemistry was performed on BAL cells and bronchial mucosal biopsy sections obtained through bronchoscopy from 14 healthy smokers and 16 healthy non-smokers. Two antibodies recognising citrullinated proteins, two antibodies recognising peptidylarginine deiminase (PAD)2 enzyme and one recognising PAD4 enzyme were used.
Results: Citrullinated proteins are upregulated in BAL cells of healthy smokers compared with healthy non-smokers. This was associated with higher expression of the PAD2 enzyme. The same level of citrullinated proteins was present in bronchial mucosal biopsy specimens of healthy smokers and non-smokers, despite higher expression of PAD2 in smokers.
Conclusion: This study provides evidence that smoking enhances PAD2 expression in the bronchial mucosal and alveolar compartment, with consequent generation of citrullinated proteins in the latter. Smoking is an environmental factor that may lead to citrulline autoimmunity in genetically susceptible subjects.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic autoimmune disease often characterised by the presence of antibodies against citrullinated peptides (CP). Epidemiological studies have proposed smoking as one of the main environmental factors associated with RA.1 We recently identified in a case–control study a gene–environment interaction between shared epitope and smoking in anti-cyclic-citrullinated-peptide (anti-CCP) antibody-positive RA.2 In an additional cohort of healthy subjects, we detected positive immunostaining for CP only in bronchoalveolar lavage (BAL) cells of smokers, suggesting that induction of citrullination in the respiratory tract might be the initial event in development of anti-CCP-positive RA.
Our aim was to extend our findings in a new prospective study including a larger number of healthy subjects. We studied citrullination not only in BAL cells but also in mucosal lung biopsy specimens using an additional antibody proposed to have higher specificity for those targets that are citrullinated in inflamed synovial tissue.3 We also studied expression of peptidylarginine deiminase (PAD) enzymes in lungs of healthy subjects.
METHODS
Samples
Fourteen healthy smokers (eight women, six men, median age 36 years) and 16 healthy non-smokers (11 women, five men, median age 34 years) were recruited. Smokers were all current smokers who had smoked for a median of 14 pack-years. All subjects had normal chest radiography findings and underwent bronchoscopy to obtain mucosal biopsy specimens from the central bronchi and BAL fluid. Cell viability was determined by trypan blue exclusion, and differential counts were evaluated by May–Grunwald and Giemsa staining. BAL cells were either cytocentrifuged on slides and 2% formaldehyde fixed or 4% formaldehyde fixed (non-centrifuged) and stored at −70°C. Bronchial mucosal biopsy specimens were snap-frozen in dry ice-cooled methanol; serial cryostat sections (7 μm) were 2% formaldehyde fixed and stored at −70°C. The Northern Stockholm Ethical Review Board approved all procedures and informed consent was obtained from all participants.
Immunohistochemistry and analysis
The presence of CP was detected using a rabbit polyclonal antibody against modified citrulline residues (AMC; Upstate, New York, USA)4 and a mouse IgM monoclonal antibody (F95).5 AMC was used for cytocentrifuged BAL cells and F95 for non-centrifuged BAL cells and bronchial mucosal biopsy specimens. For detection of PAD expression in non-centrifuged BAL cells and bronchial biopsy specimens we used two polyclonal antibodies: rabbit–anti-human PAD2 (SN665) and rabbit–anti-human PAD4 (SN823), provided by Walter van Venrooij, Nijmegen, Netherlands. Additionally, a rabbit polyclonal antibody (ROI002) (CosmoBio, Tokyo, Japan) was used to identify PAD2 expression. Appropriate controls were used for each antibody (supplementary figs 1 and2). Table 1 summarises the details of the antibodies used. The low amounts of BAL limited the availability of BAL specimens for different investigations. Only lung biopsy specimens of good histological quality (24/30) as evaluated by H&E staining were included. Staining results of BAL cells were assessed using double-blind, semiquantitative analysis followed by blinded single-observer quantitative analysis counting the percentage of positive cells per total tissue area. Bronchial biopsy specimens were analysed by double-blind, semiquantitative analysis followed by computer-assisted image analysis.
Statistical analysis
Differences between histological scores were analysed by Mann–Whitney test and differences between proportions by the Fisher exact test. A value of p<0.05 was considered significant.
RESULTS
BAL cells
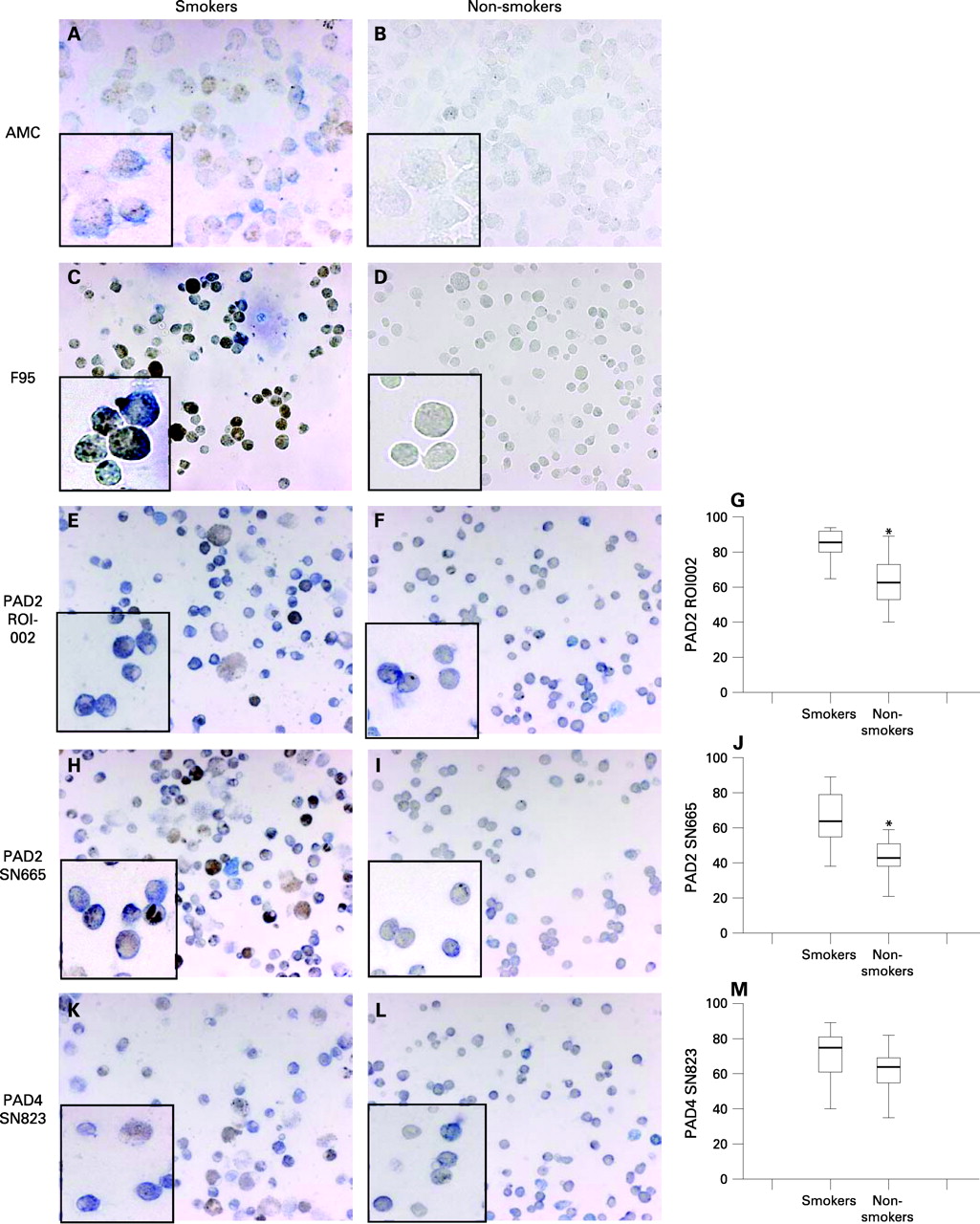
Most BAL cells were macrophages with a median of 94% in smokers and 86% in non-smokers. Fifty-six per cent of smokers (5/9) and 7% of non-smokers (1/15) were AMC positive (p<0.05) (figs 1A and B). Seventeen per cent of smokers (2/12), and none of seven non-smokers were F95 positive (figs 1C and D). The expression pattern for CP was predominantly cytoplasmic. All samples were positive for PAD2 and PAD4. We observed higher expression of PAD2 enzyme (figs 1E–J) in smokers than in non-smokers with both ROI002 antibody (median positive cells 86%, range 65–94% in 14 smokers and median 63%, range 40–89% in 14 non-smokers, p<0.001) and SN665 antibody (median positive cells 64%, range 38–89% in 14 smokers and 43%, range 21–59% in 15 non-smokers, p<0.001). No difference in PAD4 expression was observed between smokers (n = 14) and non-smokers (n = 15) (p = 0.08) (figs 1K–M). Similar to CP, PAD2 and PAD4 expression was predominantly cytoplasmic.
Bronchial mucosal biopsy specimens
Analysis of bronchial biopsy specimens showed that 100% of smokers (10/10) and 86% of non-smokers (12/14) were F95 positive, with no detectable difference in the amount and distribution of CP (p = 0.41) (figs 2A–C). The CP detected were mainly intracellular (cytoplasmic pattern) but also extracellular, in epithelial and lamina propria areas. AMC antibody was not suitable for staining the mucosal biopsy specimens owing to non-specific binding induced by the modification procedure. All biopsy specimens were positive for PAD2 and PAD4. We observed higher expression of PAD2 in smokers (median 6.2% positive stained area, range 1–17%) than in non-smokers (median 2.1% positive stained area, range 0.4–6.5%) for the SN665 (p<0.05) but not for the ROI002 antibody (p = 0.32) (figs 2D–I). No differences in PAD4 expression were detected (p = 0.22) (figs 2J–L). The expression of PAD enzymes was similar to that of CP with a mainly intracellular (cytoplasmic for PAD2, cytoplasmic and nuclear for PAD4) but also extracellular pattern, in epithelial and lamina propria areas (figs 2D, E, G, H, J, K).

{kind=link}
{kind=link}
DISCUSSION
This study confirms our previous findings that smoking is associated with generation of CP in the lung alveolar (BAL cells) compartment. Furthermore, we demonstrate for the first time that smoking is associated with higher expression of the PAD2 enzyme in two different lung compartments—the alveolar (distal airways) and bronchial mucosal (proximal airways) compartment—in smokers as compared with non-smokers.
To confirm our previous results we used the antibody from our first study2 and an additional antibody to detect CP. Both antibodies demonstrated almost exclusive expression of CP in smokers as compared with non-smokers. However, no perfect match was seen between the two stainings for sample identity, suggesting that the two antibodies might recognise different citrullinated epitopes. The AMC antibody has been developed to recognise all chemically modified citrulline residues independent of the backbone protein,6 suggesting that it recognises all the different CP.
However, there are reports suggesting that the AMC has a more restricted recognition pattern. For example, in normal adult rat brains deiminated myelin basic protein and glial fibrillary acidic protein are recognised by the F955 but not by the AMC.7 Also, in contrast to AMC, it has been suggested that the F95 has a more restrictive detection pattern with higher specificity for those targets that are citrullinated in inflamed synovial tissue.3 Additional studies to identify specific citrullinated targets recognised by each antibody in different tissues are needed to provide further insights into the potential pathogenic link between smoking, lung environment changes and synovial inflammation.
We detected CP in bronchial mucosal biopsy specimens of both healthy smokers and non-smokers that might be partly due to constitutional expression of CP in epithelial structures such as epidermis8 and oral mucosa.9 An alternative explanation may be that lung mucosa represents a natural barrier of the human body and as such, a constant continuing degree of subclinical inflammation, which could lead to citrullination,4 might be present both in smokers and non-smokers. A basal constitutional level of CP in both smokers and non-smokers might therefore preclude identification of an additive effect of smoking. However, our findings are in accordance with a recent study showing no detectable association between smoking and citrullination in lung tissues from RA-associated lung disease, idiopathic interstitial lung disease and healthy lung tissue from patients with lung cancer.10
Another potential explanation for the different smoking-related citrullination pattern in alveolar versus mucosal lung tissue might be the known anatomical differences and different cell populations between the two compartments. However, we identified higher expression of PAD2 in mucosal biopsy specimens of smokers than in non-smokers using two antibodies (the difference reached statistical significance for only one of the two antibodies used), which is consistent with the difference between PAD2 and PAD4 expression seen at the alveolar level. This finding might be related to the different maturation phase of mucosal and alveolar macrophages induced by smoking,11 as previous studies demonstrated the absence of PAD2 in monocytes as compared with mature macrophages.12 This observation is in agreement with the similar expression of PAD4 in smokers and non-smokers, as PAD4 is equally expressed in both monocytes and mature macrophages.12
Smoking increases PAD expression in BAL cells and lung mucosa but other events that influence citrullination reaction, such as an increase in intracellular calcium concentration, are also required.13 Smoking induces alveolar macrophage apoptosis,14 which in turn might result in high intracellular calcium, suggesting a potential mechanism to explain the link between smoking and citrullination induction. An alternative explanation might be that smoking induces inflammation that might lead to increased citrullination.4 No pathological changes were seen on chest radiography, but bronchiectasis might exist in smokers even in the absence of radiological signs.
Owing to the study design younger subjects than those usually developing RA are included in the current study. A longer smoking exposure would possibly increase the chance of detecting differences as it has been suggested that smoking might be associated with anti-CCP-positive RA in a dose-dependent manner.15
Our findings offer further support for our previous proposed aetiological hypothesis for RA that involves genes, environment and immunity to self molecules made immunogenic through post-translational modification. Further studies to elucidate the specific link between other environmental factors and citrullination as well as between citrullination and autoimmunity induction are needed for an understanding of RA pathogenesis.
Acknowledgments
We thank Marianne Engstrom for excellent technical assistance and help and Benita Dahlberg, Helene Blomquist, Margitha Dahl and Gunnel de Forest for assistance at bronchoscopies.
REFERENCES
Supplementary materials
web only figures 67/10/1488
Files in this Data Supplement:
{kind=link}
{kind=link}
Footnotes
▸ Additional figures are published online only at http://ard.bmj.com/content/vol67/issue10
Funding: This study was supported by grants from Ulla and Gustaf af Ugglas Foundation, Gustav den V:e Foundation, Swedish Medical Research Council, Swedish Heart Lung Foundation, Stockholm County Council, Torsten and Ragnar Soderberg Foundation, Clas Groschinskys Minnesfond.
Competing interests: None.
Ethics approval: Approved by the Northern Stockholm Ethical Review Board.
We declare that the study sponsors did not have any influence in the study design; in the collection, analysis, and interpretation of data; in the writing of the report or in the decision to submit the paper for publication.