


Abstract
Non-small cell lung cancer (NSCLC) is a major cause of cancer-related death and consumption of healthcare resources worldwide. Significant costs are generated shortly before death, partly because of continued oncological treatment during the terminal stage of disease. We analyzed factors predicting for the likelihood of active anticancer therapy during the final month of life. Patients who died from NSCLC (any stage and treatment) during the years 2006-2013 within a defined geographical region of northern Norway were included (n=266). Out of these, 28.6% received oncological treatment during the final month of life. Hospital death occurred in 70% of patients who received active treatment during their last month of life, compared to 41% of other patients (p=0.0001). Multivariate analysis showed that lack of documented resuscitation preference (p=0.001) and the presence of superior vena cava compression (p=0.039) were the most important predictors of active therapy during the last month of life. Trends were observed with regard to use of steroids for symptom palliation (p=0.067) and advanced T stage (p=0.071). Given that patients with documented resuscitation preference before their last month of life (typically a do not resuscitate order) were unlikely to receive active treatment during the final month (2% versus 35% in patients without documented preference), early discussion of prognosis, options for symptom control and resuscitation preference are crucial components in strategies for improving terminal care.
Survival of patients with lung cancer is limited. For 2005-2007, 1-year survival was 30% in the UK, 35% in Denmark, and 39-44% in Australia, Canada, Norway, and Sweden (1). Five-year survival was 9-11% in the UK and Denmark versus 15-20% in the other four countries. In the US, 5-year relative survival was 16% during the time period 1999-2005 (2). The number of estimated deaths from lung cancer in the US in 2010 was 157,300, with non-small cell lung cancer (NSCLC) being the largest contributor. As a consequence, a large number of patients with NSCLC worldwide receive palliative treatment, either at diagnosis or recurrence. These patients might experience a considerable symptom burden when their disease becomes refractory to a given line of treatment and in the terminal phase. Ideally, it would be desirable to obtain symptom control without aggressive end-of-life care, thus avoiding potentially toxic and distressing treatments (3, 4).
As described previously, significant costs are generated by oncological treatment during the final months of life, with hospitalization being a major cost driver (5, 6). In a recent study including 112 patients, we revealed that during the last three months of life, systemic treatment was given to 28% and thoracic radiotherapy to 23% of patients who died from NSCLC (7). During their last four weeks of life, 27% the patients received some type of active oncological therapy, i.e. radiotherapy with/without chemotherapy including tyrosine kinase inhibitors. Other studies suggest that standard oncological care often follows comparable traits (6, 8, 9) and indicate that more research on terminal care is needed. By expanding our previous database, we aimed to identify patients' characteristics associated with active anticancer treatment during the final month of life. Knowledge regarding predictive factors might improve decision making during the terminal phase of NSCLC.
Patients and Methods
This retrospective study included all patients who died from NSCLC in the uptake area of the Nordland Hospital Trust (NHT). Here all lung cancer care is prescribed and guided by the staff at NHT. NHT is owned by the Ministry of Health and Care services (www.hod.dep.no) and administered through a regional trust (North Norway Regional Health Authority trust, www.helse-nord.no). It provides specialist healthcare services to approximately 112,000 inhabitants in Nordland County, i.e. roughly 50% of the population of the county (a geographically widespread, largely rural area) including its main city Bodø. No private pulmonology or oncology services are available. This fact and the structure of the Norwegian healthcare system allows for evaluation of unselected patient groups almost comparable to large population-based registries, albeit with limited size. We used the electronic databases of the Departments of Oncology and Palliative Medicine, Pulmonology, Thoracic Surgery and the Division of Internal Medicine, NHT, to identify all patients treated for histologically-confirmed NSCLC and selected those who died during the time period from January 1st 2006 to September 30th 2013. Consequently, the initial diagnosis of NSCLC could have been made earlier. Out of 418 patients with NSCLC, 266 died from the disease and were included in this study. We excluded the remaining 152 patients because they were alive at the date of data extraction (October 1st 2013, n=119), had died from intercurrent disease with their NSCLC in remission (n=6), had died within 30 days after surgery (n=4) or were lost to follow-up (n=23). All medical records, including co-morbidity and medication use, death certificates and demographic data, were available in the hospital's electronic patient record (EPR) system (DIPS®) and were retrospectively reviewed starting from the first referral for suspected lung cancer until death. Our cohort was divided into two subgroups, i.e. patients who had received anticancer treatment during the final month of life and those who had not received such treatment. All patients were Caucasians, born in Norway and covered by the national public insurance system. Their treatment was based on national guidelines developed by the Norwegian Lung Cancer Group (www.nlcg.no) and discussed by a multi-disciplinary tumor board which meets on a weekly basis. TNM staging was applied as described in a prior publication (10).
Statistical analysis and ethics. Patients were selected from the hospitals EPR system and the IBM SPSS 21 software package (IBM SPSS Statistics, Somers, NY, USA) was employed for the database and statistical analyses. For comparison of dichotomous variables the Chi-square test and Fisher's exact test, where applicable, were employed, and for continuous variables the Mann Whitney U-test. For multivariate prediction of the primary study end-point (receipt of anticancer treatment during the final month of life), logistic regression analysis was used (backward stepwise approach). Only variables with p-value <0.1 in univariate test were included in the multivariate analysis. The following variables were analyzed: age, sex, weight loss, co-morbidity, prescription drug use, smoking status, immediate family network, T stage, N stage, TNM stage (seventh edition), initial pattern of metastatic disease (if any), presence of superior vena cava compression (SVCC), histology, initial management strategy, number of lines of systemic treatment, use of thoracic radiotherapy, use of steroids or opioid analgesics, patients' resuscitation preferences. The significance level was set to 5% and all tests were carried out two-sided. The study was performed as a retrospective analysis of end-of-life care for NSCLC. As a quality of care analysis, no approval from the Regional Committee for Medical and Health Research Ethics (REK) was necessary.
Results
The study population comprised of 266 patients, out of which 76 (28.6%) received active anticancer treatment during their last month of life. As shown in Table I thoracic radiotherapy was the most common type of treatment. The proportion of patients with active treatment during the last month of life remained constant during the time period of our study (2006-2013, p=0.44). The same holds true when performing a dichotomized analysis, i.e. comparing the years 2006-2009 to 2010-2013. Table II shows the baseline characteristics and univariate analyses of factors predicting active treatment during the last month of life. The only parameter approaching statistical significance was SVCC (at diagnosis or later, p=0.08). Tumor stage at diagnosis approached significance when dichotomized (stage I-IIIA compared to IIIB-IV, p=0.09). T Stage at diagnosis was significant when dichotomized (T1/2 compared to T3/4, p=0.025). Patterns of care are shown in Table III. It is interesting to note that even 16% of patients who initially were managed with best supportive care (BSC) later received active therapy during their last month of life. The rates of active therapy were numerically higher in the other groups [initial surgery 29%, radical (chemo)radiation 20%, systemic therapy alone 36%, palliative radiotherapy 30%; differences not significant]. Patients who needed steroids for symptom palliation, either initially or later during the course of disease, were significantly more likely to receive active therapy during their final month of life than patients who had never received steroids (35% versus 21%, p=0.045). Patients with documented resuscitation preference before their last month of life (typically a do not resuscitate order) were unlikely to receive active treatment during the final month (2% versus 35% in patients without documented preference and 40% in patients with preference documented during the final month of life, p<0.001). No other treatment-related factors were statistically significant.
Details regarding anticancer treatment during the final month of life (n=76; 13 patients received more than one therapy).
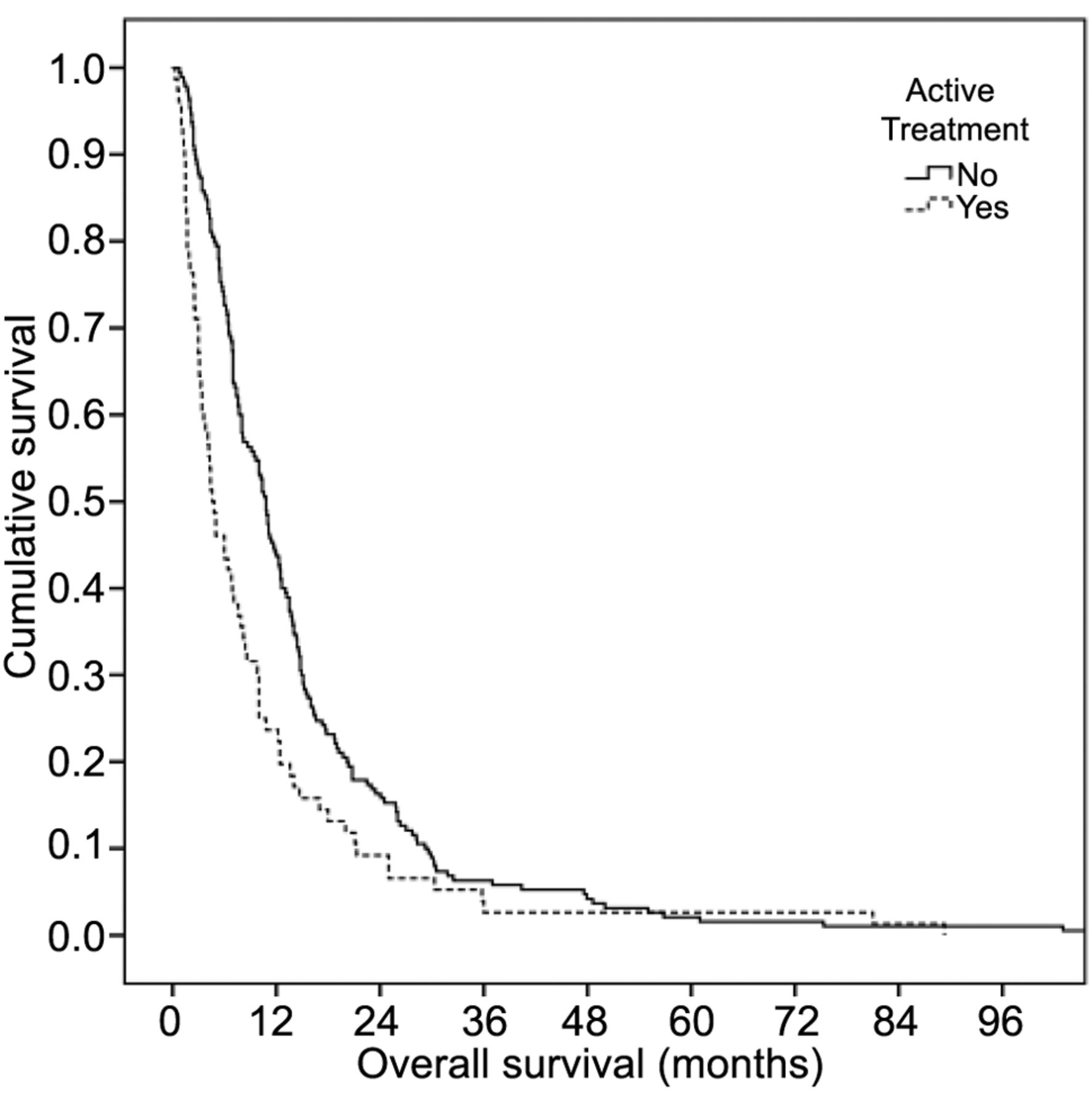
Multivariate logistic regression analysis (including SVCC, tumor stage, T stage, resuscitation preference and steroid use) revealed that documented resuscitation preference (p=0.001) and SVCC (p=0.039) were the most important predictors of active therapy during the last month of life, followed by steroids (p=0.067), advanced T stage (p=0.071) and tumor stage (p=0.58). Given that only two factors achieved statistical significance and SVCC was a rare event, no predictive score was developed. Pleurodesis was performed during the last month of life in 11% of patients who received active anticancer therapy compared to 4% of those who did not (p=0.034). Significantly more patients from the active-treatment group received continuous analgesics via pump during their last month of life (39% versus 22%, p=0.01). The rate of red blood cell transfusions administered during the last month of life was similar (13% versus 14%, p=1). The rate of intravenous antibiotics given during the last month of life was numerically higher in actively-treated patients (56% versus 48%, p=0.32). Median survival was significantly shorter among patients who received active therapy during the last month of life (4.7 versus 10.8 months, Figure 1). Place of death was also significantly different (p<0.001), with hospital death occurring for 70% of patients who received active treatment during their last month of life, compared to 41% for the other patients.
Baseline parameters at lung cancer diagnosis.
Patterns of care and general outcomes.

Actuarial Kaplan-Meier survival curves for patients with and without active treatment during the final month of life (median 4.7 versus 10.8 months), p=0.001, log-rank test.
Cause of death was documented reliably and in sufficient detail mostly for patients who died in hospitals. Details were unknown in a considerable proportion of patients, especially in the sub-group without active therapy during the last month of life, where hospital death was less common (Table IV). The prevailing cause of death in patients with known cause was NSCLC progression (72% in patients without and 68% in patients with active therapy during the last month of life).
Discussion
During the last days of life, sufficient time resources should be allocated to communication with patients and their relatives and to the preparation for the final steps of life. In a previous study with 112 patients, we found that during the last four weeks of life, 27% of patients received some type of active oncological therapy, i.e. radiotherapy with/without chemotherapy including tyrosine kinase inhibitors (7). This prompted us to embark on a larger study aiming at identifying of those patients at high risk of active anticancer treatment during their last month of life. We expected to be able to develop a predictive model based on patient characteristics at initial NSCLC diagnosis. The strengths of the present study are the completeness and comprehensiveness of data and the unselected real-life patient population. Even very elderly patients, those with adverse prognostic features, and those managed with BSC were included. The retrospective design is, however, a weakness. We were surprised to see the limited association between baseline parameters, including TNM stage, weight loss or age, and active therapy during the final month of life. Performance status (PS) was not included because changes may occur in both directions (improvement due to response to treatment, deterioration because of progression or toxicity) and the follow-up intervals will vary. In principle, disease characteristics might also change at any time after diagnosis. For example, initial T4 tumors might respond completely or near-completely to radical chemoradiation, brain metastases might develop and so on. We performed an exploratory analysis of such dynamic changes when looking at patients with initial brain metastases and those who were diagnosed with brain metastases at any time during follow-up as compared to those who remained free from this complication. Neither of these scenarios had any significant correlation with our primary study end-point.
Cause of death.
It is also important to emphasize that accurate survival prediction for an individual patient is elusive, despite several published scores that are able to discriminate between patient groups with different prognoses (11-16). In other words, whenever starting a new type or line of treatment, the subsequent clinical course might deviate from the prescribing physician's expectation (17). Whether or not treatment takes place during the final month of life is not firmly known at the time of treatment prescription. Our results indicate that active treatment during the final month of life typically took place in an attempt to palliate cancer-related symptoms, and that the number of patients in whom palliation was difficult without active anticancer treatment was constant over the time period 2006-2013. Patients who received active anticancer therapy during their final month of life were also significantly more likely to receive steroids, continuous analgesics via pump or pleurodesis, probably reflecting a higher symptom burden. The fact that patients with initial T3 or T4 tumors were more likely to receive active therapy during their final month of life and that thoracic radiotherapy was the most common type of treatment might indicate a high symptom burden from such primary tumors (airway obstruction, atelectasis, pneumonia, bleeding, chest pain). Given the higher symptom burden, higher T stage and presence of SVCC, the poorer overall survival of patients who received active therapy during their final month of life is not surprising (median 4.7 versus 10.8 months). In these cases, oncological treatment obviously was not able to prolong survival. The findings may also partly indicate that the medical doctors were not aware of the limited life expectancy, and continued anticancer therapy during the last days of life.
Was any positive outcome recorded? Our database did not include information about symptom palliation. From a methodological point of view, prospective quality of life data collection is needed to answer the question “Does palliative oncologic therapy in terminally-ill patients with NSCLC provide worthwhile clinical benefits even if survival remains unchanged or is such treatment always inappropriate irrespective of symptom burden?”
Notably, 50% of patients with SVCC received active treatment during the final month of life, indicating that attempts to treat this complication are successful in only half of the cases. On the other hand, median survival after SVCC was 7.2 months among patients who presented with this syndrome at initial NSCLC diagnosis, indicating that responding patients benefit from treatment and that nihilistic approaches are not warranted.
Patients with documented resuscitation preference before their last month of life (typically a do not resuscitate order) were unlikely to receive active treatment during the final month (2% versus 35% in patients without documented preference and 40% in patients with preference documented during the final month of life, p<0.001). This is probably one of the most important messages of the present study. If one attempts to reduce the rate of active treatment during the final month of life, one has to start communicating prognosis, resuscitation preferences, hospice care options, supportive measures and other patient or caregiver concerns and expectations early during the disease trajectory. Even if one acknowledges that i) prediction of treatment toxicities and prognosis in individual patients are still imperfect, ii) occasionally patients will die unexpectedly, and iii) one does not want to destroy patients' hope while providing active treatment, there is a potential for improved strategies of palliative care during the last months of life in these patients. Recently Yun et al. reported that patients informed of their terminal diagnosis had a significantly better quality of life, fewer symptoms, and had a lower rate of emotional distress than patients deducing it from their worsening condition (18). When patients' expectations are in harmony with their doctors' communication, positive effects on quality of life seem to occur.
Temel et al. published a randomized trial of early palliative care for patients with newly-diagnosed metastatic NSCLC, which recruited patients in the time period between 2006 and 2009 (19). This single-institution trial included 151 patients with defined performance status [(ECOG) 0-2] who were younger than the general NSCLC population (mean 65 years). Early palliative care integrated with standard oncology care was compared to standard oncology care alone. Patients assigned to the experimental-arm consulted with a member of the palliative care team within three weeks of enrollment and at least monthly thereafter. Those assigned to the standard-care arm only met with the palliative care team on request from the patient, family, or oncologist. Early palliative care integrated with standard oncological care led to significant improvements in quality of life and mood from baseline to 12 weeks. Moreover, more patients assigned to early palliative care had their resuscitation preferences documented. Fewer patients received aggressive end-of-life care, yet median survival was longer among patients receiving early palliative care (11.6 versus 8.9 months). No significant differences were observed with regard to the number of chemotherapy lines that the participants received (20). The groups were similar with respect to time between first- and second-line chemotherapy, as well as between second- and third-line chemotherapy. Adjusted for age, sex, and performance status, patients in the early-palliative-care group were half as likely to receive chemotherapy during their final two months of life (p=0.05). Within 30 days prior to death, chemotherapy was received by 43% of those under standard care and 30% of those in the experimental arm (p=0.14). Compared to our own study, which also assessed radiotherapy, a chemotherapy utilization rate of 30% is quite high.
Aggressive end-of-life care and delayed focus on symptom palliation are highly important issues in a world of limited healthcare budgets. The heightened focus on palliative interventions and terminal care, as well as improved communication and shared decision-making, is an important and timely development. Time spent on active therapy at the end of life may be allocated to communication with patients and their relatives, as well as preparation for the final steps of life. Both individual physicians and tumor boards were shown to overestimate the survival of patients with very limited prognosis, i.e. those who died in less than one month (21). It is crucial to examine key prognostic factors when trying to avoid inappropriate use of chemo- or radiotherapy during the final month of life. Combined analysis of individual data from nine randomized trials of second-line treatment in advanced NSCLC suggested that prognosis was significantly influenced by gender (worse in males), performance status, tumor histology (worse in squamous and other histology versus adenocarcinoma), stage (worse in IV versus IIIB), and response to first-line therapy (worse for patients not obtaining objective response) (15).
- Received November 29, 2013.
- Revision received December 16, 2013.
- Accepted December 17, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}