
Abstract
Introduction
Pulmonary endarterectomy (PEA) is the most effective treatment for chronic thromboembolic pulmonary hypertension (CTEPH). The aim of this study is to evaluate long-term survival and freedom from clinical worsening after PEA.
Methods
All patients who underwent PEA in our hospital between May 2000 and August 2009 were included. Follow-up parameters were all-cause mortality and time to clinical worsening, defined as a combination of death, need for pulmonary hypertension-specific medication or 15% decrease in six-minute walk distance without improvement in functional class. The Cox proportional hazard regression was used to identify predictors.
Results
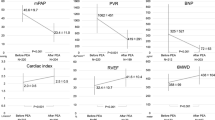
Seventy-four consecutive patients (mean age 55.9 ± 13.8 years, 51% female) underwent PEA. Prior to surgery, 55 patients were in NYHA functional class III or higher. The mean pulmonary artery pressure was 41.3 ± 11.9 mmHg with a mean pulmonary vascular resistance of 521 ± 264 dyn·s·cm−5 (range 279–1331 dyn·s·cm−5). Five patients (6.8%) died in-hospital. Out of hospital, 5 out of 69 patients (7.2%) died during a median follow-up of 3.7 ± 2.2 years [range 0.1–8.5 years]). The one- and five-year survival rates were 93% and 89%, respectively. During follow-up, clinical worsening occurred in 13 out of 69 patients (18.8%). The one- and five-year rates of freedom from clinical worsening were 94% and 72%, respectively. The baseline NT-pro BNP level tended to be a predictor for occurrence of clinical worsening.
Conclusion
Pulmonary endarterectomy is associated with good long-term survival in patients with CTEPH. However, clinical worsening occurred in a substantial number of patients at long-term follow-up.

Similar content being viewed by others


References
Becattini C, Agnelli G, Pesavento R, et al. Incidence of chronic thromboembolic pulmonary hypertension after a first episode of pulmonary embolism. Chest. 2006;130:172–5.
Pengo V, Lensing AW, Prins MH, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350:2257–64.
Klepetko W, Mayer E, Sandoval J, et al. Interventional and surgical modalities of treatment for pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43:73S–80.
Hoeper MM, Mayer E, Simonneau G, Rubin LJ. Chronic thromboembolic pulmonary hypertension. Circulation. 2006;113:2011–20.
Jamieson SW, Kapelanski DP, Sakakibara N, et al. Pulmonary endarterectomy: experience and lessons learned in 1500 cases. Ann Thorac Surg. 2003;76:1457–62.
Saouti N, Morshuis WJ, Heijmen RH, Snijder RJ. Long-term outcome after pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension: a single institution experience. Eur J Cardiothorac Surg. 2009;35:947–52.
Condliffe R, Kiely DG, Gibbs JS, et al. Improved outcomes in medically and surgically treated chronic thromboembolic pulmonary hypertension. Am J Respir Crit Care Med. 2008;177:1122–7.
Kim NH. Assessment of operability in chronic thromboembolic pulmonary hypertension. Proc Am Thorac Soc. 2006;3:584–8.
Masuda M, Nakajima N. Our experience of surgical treatment for chronic pulmonary thromboembolism. Ann Thorac Cardiovasc Surg. 2001;7:261–5.
Daily PO, Dembitsky WP, Iversen S. Technique of pulmonary thromboendarterectomy for chronic pulmonary embolism. J Card Surg. 1989;4:10–24.
Jamieson SW, Kapelanski DP. Pulmonary endarterectomy. Curr Probl Surg. 2000;37:165–252.
Matsuda H, Ogino H, Minatoya K, et al. Long-term recovery of exercise ability after pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension. Ann Thorac Surg. 2006;82:1338–43.
Freed DH, Thomson BM, Berman M, et al. Survival after pulmonary thromboendarterectomy: Effect of residual pulmonary hypertension. J Thorac Cardiovasc Surg. 2010 May 12. [Epub ahead of print].
Bonderman D, Skoro-Sajer N, Jakowitsch J, et al. Predictors of outcome in chronic thromboembolic pulmonary hypertension. Circulation. 2007;115:2153–8.
Auger WR, Kerr KM, Kim NH, Ben-Yehuda O, Knowlton KU, Fedullo PF. Chronic thromboembolic pulmonary hypertension. Cardiol Clin. 2004;22:453–66. vii.
Kim NH, Fesler P, Channick RN, et al. Preoperative partitioning of pulmonary vascular resistance correlates with early outcome after thromboendarterectomy for chronic thromboembolic pulmonary hypertension. Circulation. 2004;109:18–22.
Galiè N, Kim NH. Pulmonary microvascular disease in chronic thromboembolic pulmonary hypertension. Proc Am Thorac Soc. 2006;3:571–6.
Dartevelle P, Fadel E, Mussot S, et al. Chronic thromboembolic pulmonary hypertension. Eur Respir J. 2004;23:637–48.
Kim NH. Assessment of operability in chronic thromboembolic pulmonary hypertension. Proc Am Thorac Soc. 2006;3:584–8.
Freed DH, Thomson BM, Tsui SS, et al. Functional and haemodynamic outcome 1 year after pulmonary thromboendarterectomy. Eur J Cardiothorac Surg. 2008;34:525–9.
Reesink HJ, van der Plas MN, Verhey NE, van Steenwijk RP, Kloek JJ, Bresser P. Six-minute walk distance as parameter of functional outcome after pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension. J Thorac Cardiovasc Surg. 2007;133:510–6.
Corsico AG, D'Armini AM, Cerveri I, et al. Long-term outcome after pulmonary endarterectomy. Am J Respir Crit Care Med. 2008;178:419–24.
McLaughlin VV, Badesch DB, Delcroix M, et al. End points and clinical trial design in pulmonary arterial hypertension. J Am Coll Cardiol. 2009;54:S97–107.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schölzel, B., Snijder, R., Morshuis, W. et al. Clinical worsening after pulmonary endarterectomy in chronic thromboembolic pulmonary hypertension. Neth Heart J 19, 498–503 (2011). https://doi.org/10.1007/s12471-011-0203-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12471-011-0203-4