



Outdoor air pollution, exhaled 8-isoprostane and current asthma in adults: the EGEA study
- 1INSERM U1168, VIMA (Aging and Chronic Diseases: Epidemiological and Public Health Approaches), Villejuif, France
- 2Université Versailles St-Quentin-en-Yvelines, UMRS 1168, Montigny-le-Bretonneux, France
- 3Pôle de Biologie Pathologie Génétique, Laboratoire de Biochimie et Biologie Moléculaire, CHU de Lille, Lille, France
- 4ISGlobal, Centre for Research in Environmental Epidemiology, Universitat Pompeu Fabra, CIBER Epidemiología y Salud Pública, Barcelona, Spain
- 5Equipe d'Epidémiologie Environnementale, Institute for Advanced Biosciences, Centre de Recherche UGA, INSERM U1209, CNRS UMR 5309, Grenoble, France
- 6Institute for Risk Assessment Sciences, Utrecht University, Utrecht, The Netherlands
- 7Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, The Netherlands
- 8Santé Publique France, Saint-Maurice, France
- 9Swiss Tropical and Public Health Institute, Basel, Switzerland
- 10University of Basel, Basel, Switzerland
- 11Université Lille and CHU de Lille, Lille, France
- 12These authors are joint last authors
- B. Jacquemin, INSERM U1168, VIMA (Aging and Chronic Diseases: Epidemiological and Public Health Approaches), 16 avenue Paul Vaillant Couturier, 94807 Villejuif Cedex, France. E-mail: benedicte.jacquemin{at}inserm.fr
Abstract
Associations between outdoor air pollution and asthma in adults are still scarce, and the underlying biological mechanisms are poorly understood. Our aim was to study the associations between 1) long-term exposure to outdoor air pollution and current asthma, 2) exhaled 8-isoprostane (8-iso; a biomarker related to oxidative stress) and current asthma, and 3) outdoor air pollution and exhaled 8-iso.
Cross-sectional analyses were conducted in 608 adults (39% with current asthma) from the first follow-up of the French case–control and family study on asthma (EGEA; the Epidemiological study of the Genetic and Environmental factors of Asthma). Data on nitrogen dioxide, nitrogen oxides, particulate matter with a diameter ≤10 and ≤2.5 µm (PM10 and PM2.5), road traffic, and ozone (O3) were from ESCAPE (European Study of Cohorts for Air Pollution Effects) and IFEN (French Institute for the Environment) assessments. Models took account of city and familial dependence.
The risk of current asthma increased with traffic intensity (adjusted (a)OR 1.09 (95% CI 1.00–1.18) per 5000 vehicles per day), with O3 exposure (aOR 2.04 (95% CI 1.27–3.29) per 10 µg·m−3) and with exhaled 8-iso concentration (aOR 1.50 (95% CI 1.06–2.12) per 1 pg·mL−1). Among participants without asthma, exhaled 8-iso concentration increased with PM2.5 exposure (adjusted (a)β 0.23 (95% CI 0.005–0.46) per 5 µg·m−3), and decreased with O3 and O3-summer exposures (aβ −0.20 (95% CI −0.39– −0.01) and aβ −0.52 (95% CI −0.77– −0.26) per 10 µg·m−3, respectively).
Our results add new insights into a potential role of oxidative stress in the associations between outdoor air pollution and asthma in adults.
Abstract
Exhaled 8-isoprostane concentration is associated with both outdoor air pollution and current asthma in adults http://ow.ly/esqN30iGCH3
Introduction
According to the World Health Organization, outdoor air pollution caused 3.7 million deaths globally in 2012 and 9% of the total mortality in France was recently attributed to particulate matter with a diameter ≤2.5 µm (PM2.5) [1]. The most studied pollutants in relation to health effects are nitrogen dioxide (NO2), ozone (O3), and particulate matter with a diameter ≤10 µm (PM10) and PM2.5. Evidence of the impact of outdoor air pollution on respiratory health is increasing [2, 3], and the associations between exposure to outdoor air pollution and asthma have largely been studied in children [4]. However, studies on associations between long-term exposure to outdoor air pollution and asthma among adults are still carce [5].
One biological mechanism proposed to partly explain the association between outdoor air pollution and asthma is oxidative stress [6]. Oxidative stress is an imbalance between the increase in reactive oxygen species and antioxidant response [7]. Among the biological markers related to oxidative stress, 8-isoprostane (8-iso; a prostaglandin F2-like compound belonging to the F2-isoprostane class) is known as a stable and specific product of lipid peroxidation [8]. Interestingly, 8-iso can be measured noninvasively in exhaled breath condensate (EBC) [7]. An increase of 8-iso concentration along with a decline of antioxidant defence can induce tissue damage and can contribute to pathophysiological changes such as those seen in asthma [9, 10]. 8-iso is known to provoke airway hyperresponsiveness, to increase the production of mucus and to promote contraction of smooth muscles [10, 11]. In a recent systematic review, 8-iso concentration was found to be higher in adults with severe asthma than in those with mild-to-moderate asthma [12]. To date, epidemiological studies on the associations between long-term exposure to outdoor air pollution and asthma including the measurement of 8-iso in adults are lacking.
Here, among adults from the French EGEA (Epidemiological study of the Genetic and Environmental factors of Asthma) cohort, we first studied the associations between long-term exposure to outdoor air pollution (NO2, nitrogen oxides (NOx), PM10, PM2.5, traffic load, traffic intensity, O3 and O3-summer) and current asthma. Second, we studied the associations between 8-iso measured in EBC with both long-term exposure to outdoor air pollution and current asthma.
Methods
Study population
The EGEA is a cohort study based on an initial group of asthma cases recruited in chest clinics from five French cities (1991–1995) along with their first-degree relatives and a group of controls (https://egeanet.vjf.inserm.fr). Child controls were recruited from surgery hospitals, and adult controls from electoral rolls and from surgery hospitals or check-up centres [13]. The protocol and descriptive characteristics have been described previously [13, 14], and inclusion criteria used to define asthmatic cases and controls are described in the supplementary material. The EGEA collection is certified ISO 9001 [15]. Ethical approval was obtained from the relevant institutional review board committees (Cochin Port-Royal Hospital and Necker-Enfants Malades Hospital, Paris, France). All participants signed a written informed consent form.
The present analyses included 608 adults (≥16 years old) in the framework of the first follow-up (EGEA2, 2003–2007), with available data on current asthma, outdoor air pollution assessed by ESCAPE (European Study of Cohorts for Air Pollution Effects) and exhaled 8-iso concentration (figure 1). Among the 608 participants, five had no pollution data from the IFEN (French Institute for the Environment) assessment. No significant differences were found between the participants included and those not included (n=963) (supplementary table E1).
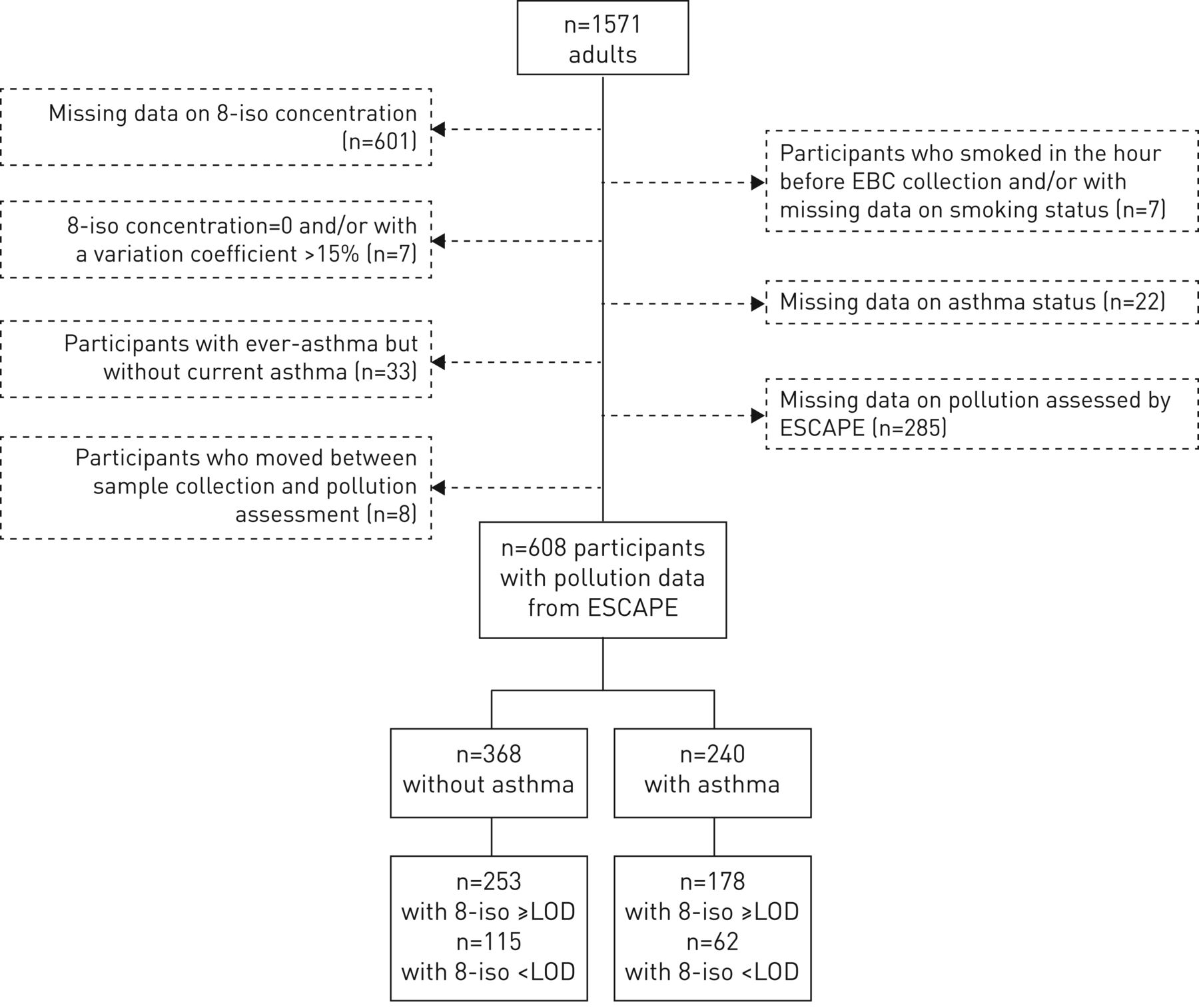
Flowchart of the studied population. 8-iso: 8-isoprostane; EBC: exhaled breath condensate; ESCAPE: European Study of Cohorts for Air Pollution Effects; LOD: limit of detection.
Respiratory phenotypes
At EGEA2, the participants with ever-asthma answered positively to at least one of the two questions “Have you ever had attacks of breathlessness at rest with wheezing?” or “Have you ever had asthma attacks?”, or were recruited as asthmatic cases at EGEA1.
Among participants with ever-asthma, “current asthma” was defined by a report of respiratory symptoms (wheeze, nocturnal chest tightness, attacks of breathlessness following strenuous activity, at rest or at night-time) or asthma attacks, or use of inhaled and/or oral medicines because of breathing problems in the past 12 months (see supplementary material for more details) [16]. Only participants with current asthma were included in the analyses because the phenotype “current asthma”, which reflects the recent activity of the disease, was more relevant than the phenotype “ever-asthma” to study the associations between long-term exposure to outdoor air pollution, biological markers and asthma.
Exposure assessment
Using ESCAPE and IFEN assessments, outdoor air pollution exposures (NO2, NOx, particulate matter, O3 and road traffic) were assigned to each participant's residential address.
Annual air pollution levels of NO2 and particulate matter were derived from ESCAPE standardised models (www.escapeproject.eu). Briefly, the ESCAPE monitoring campaigns took place between 2009 and 2010, including 40 measurement sites for NO2 and NOx in Paris, Lyon, Grenoble and Marseille, and 20 particulate matter measurement sites in Paris and Grenoble. Land-use regression (LUR) models were developed and two indicators of road traffic were also calculated. Traffic intensity on nearest road was defined as the number of motor vehicles circulating per day on the nearest road to the participant's home and was expressed in vehicles per day. Total traffic load was defined as the traffic load on all major roads based around a buffer of 100 m from the participant's home and was expressed by traffic intensity multiplied by road length. Back-extrapolation was used to transfer the recent or current LUR models to earlier years. In our study, the estimation of outdoor air pollution by ESCAPE took place after EGEA2, and accordingly we also analysed the back-extrapolated pollution estimates in order to obtain a better temporality between outdoor air pollution with current asthma and EBC collection. Back-extrapolated pollution data were available for NO2 and NOx in all cities, and for PM10 in Paris.
In order to supplement the ESCAPE data set, we used O3 and O3-summer exposures from the IFEN (see supplementary material for more details). The O3 estimate was the yearly mean ozone level in 2004 for each participant at the residential address and derived from a geo-statistical model as described previously [17]. The O3-summer exposure was assessed from the monthly means from April to September.
Measurement of exhaled 8-iso
EBC was collected at EGEA2 between 2003 and 2006 with an RTube (Respiratory Research, Charlottesville, VA, USA) according to a standardised method as described previously [18]. Samples were immediately stored at −80°C. Exhaled 8-iso concentration was measured 5.3–9.4 years after EBC collection, with a specific 8-iso enzyme immunoassay kit (Cayman Chemical, Ann Arbor, MI, USA) according to the manufacturer's protocol. Approximately 30% of the exhaled 8-iso concentration measurements were below the limit of detection (see supplementary material for more details).
Statistical analyses
The level of outdoor air pollution was described by city. Due to its skewed distribution, the exhaled 8-iso concentration was log10-transformed.
Associations between outdoor air pollution and current asthma, and associations between exhaled 8-iso concentration and current asthma, were studied with logistic models. In order to study the association between outdoor air pollution and exhaled 8-iso concentration independently of asthma, linear regression models were first performed among participants without asthma and sensitivity analyses were conducted by: 1) using back-extrapolated pollution estimates, 2) studying the associations by city and 3) using bipollutant models (PM2.5 and O3 or O3-summer). Analyses with back-extrapolated pollution estimates were performed to obtain a better temporality between pollution and EBC collection. We also studied the associations between outdoor air pollution and exhaled 8-iso concentration in all participants and among participants with current asthma.
All estimates were adjusted for age, sex and smoking status. Further adjustments were conducted for body mass index (BMI), socioprofessional category and use of cleaning products, which is an indicator of exposure to indoor pollution. In order to study only the road traffic effect, estimates of associations between road traffic and current asthma or exhaled 8-iso concentration were also adjusted for background NO2. As the aim was to study the effect of long-term exposure to outdoor air pollution, we performed sensitivity analyses by excluding participants who lived at the same address for <1 year (n=46).
In order to take into account the city effect on outdoor air pollution levels, we performed meta-analyses including city-specific analyses from the Harvard School of Public Health's macro program %metaanal (www.hsph.harvard.edu/donna-spiegelman/software/metaanal) and pooled analyses with random effect on city.
The above models took into account random effects on familial dependence. All the results are expressed for an increase of 1 pg·mL−1 of exhaled 8-iso concentration, 20 µg·m−3 of NOx, 10 µg·m−3 of NO2, PM10, O3 and O3-summer, and 5 µg·m−3 of PM2.5. For traffic measures, the results of traffic load are expressed for 4 million vehicles×m per day on major roads within a 100 m buffer and the results of traffic intensity are expressed for an increase of 5000 vehicles per day on major roads. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
The mean age of the 608 adults was 43 years, 47% were males, 39% had current asthma, 21% were current smokers and 37% were overweight (BMI ≥25 kg·m−2) (table 1). Participants with current asthma were younger, more often men, current smokers and unemployed (table 1). Participants with current asthma had also a lower forced expiratory volume in 1 s (FEV1), higher airway hyperresponsiveness, higher allergic sensitisation, higher IgE level and higher exhaled 8-iso concentration than those without asthma.
Characteristics of adult participants according to asthma status
The characteristics of participants were heterogeneous across cities (see supplementary material for more details).
The pollutant and traffic levels were the highest in Paris, except for the PM10 level (supplementary figures E1 and E2). The PM10 and PM2.5 levels were above the values recommended by the World Health Organization. The O3 and O3-summer levels were the highest in Marseille (supplementary figure E3). Positive and significant correlations were found between NO2, NOx, PM10 and PM2.5 (0.47≤r≤0.95; all p<0.002), whereas O3 and O3-summer levels were negatively correlated with all pollutants (−0.50≤r≤ −0.15; all p<0.002) (data not shown). The NO2 level was significantly higher in managers and technicians, and O3-summer level was significantly higher in manual workers (data not shown).
The geometric mean (interquartile range) exhaled 8-iso concentration was 3.16 (1.41–7.69) pg·mL−1 in all participants and 3.97 (1.85–9.10) pg·mL−1 among those with current asthma (table 1), and was seven times higher in Paris than in other cities, was higher in females and decreased with age (supplementary tables E2 and E3). No significant association was found between exhaled 8-iso concentration and smoking expressed as current smoker, quantity of tobacco or number of pack-years (all p>0.80; data not shown). No interplate variability was observed (data not shown), and no association was found between storage time and exhaled 8-iso concentration (regression coefficient 0.02; p=0.39).
Associations between outdoor air pollution and current asthma
Associations between outdoor air pollution and current asthma were not significantly heterogeneous between cities (Q-test; p>0.08). In pooled analyses, the risk of current asthma increased significantly with traffic intensity (adjusted (a)OR 1.09, 95% CI 1.00–1.18) and with O3 exposure (aOR 2.04, 95% CI 1.27–3.29) (table 2) whatever the adjustment. The results were similar after excluding participants who lived at the same address for <1 year. Back-extrapolated exposure estimates gave similar results (supplementary table E4).
Associations between outdoor air pollution and current asthma
Associations between exhaled 8-iso concentration and current asthma
A positive and significant association was found between exhaled 8-iso concentration expressed as a continuous variable and current asthma (aOR 1.50, 95% CI 1.06–2.12) (figure 2). No significant association was found when exhaled 8-iso concentration was expressed as below the limit of detection, or above or equal to the limit of detection. Overall, the risk of current asthma increased significantly with exhaled 8-iso concentration expressed as below the limit of detection, above or equal to the limit of detection and less than or equal to the median, or above or equal to the limit of detection and greater than the median (ptrend=0.05).

{kind=link}
{kind=link}
Associations between exhaled 8-isoprostane (8-iso) concentration and current asthma. LOD: limit of detection. The logistic models were conducted with random effects on familial dependence. Estimates were adjusted for age, sex, smoking status and body mass index. 8-iso concentration was log10-transformed. Data are presented as odds ratios and 95% confidence intervals with participants without asthma as reference. #: result is expressed of an increase for 1 unit of the concentration in 8-iso; ¶: 8-iso <LOD was used as reference category.
Exhaled 8-iso concentration was unrelated to duration of asthma (years) or age of asthma onset expressed continuously (years) or in classes (all p>0.40). Furthermore, no significant association was found between exhaled 8-iso concentration with FEV1 % predicted continuously or in classes (all p>0.60) or allergic sensitisation (p=0.12) (data not shown).
Associations between outdoor air pollution and exhaled 8-iso concentration among participants without asthma
Associations between outdoor air pollution and exhaled 8-iso concentration were not heterogeneous between cities (Q-test; p>0.20). In pooled analyses, exhaled 8-iso concentration increased significantly with PM2.5 exposure (adjusted (a)β 0.23, 95% CI 0.005–0.46), and decreased with O3 and O3-summer exposures (aβ −0.20, 95% CI −0.39– −0.01 and aβ −0.52, 95% CI −0.77– −0.26, respectively) whatever the adjustment (table 3). The results were similar after excluding participants who lived at the same address for <1 year. Analyses performed with back-extrapolated data also gave similar results (supplementary table E5). Furthermore, exhaled 8-iso concentration decreased significantly with O3 and O3-summer exposures in Paris (aβ −0.22, 95% CI −0.42– −0.02) and aβ −0.53, 95% CI −0.90– −0.16, respectively) (supplementary table E6). After excluding participants from Paris (n=111), no significant associations were observed between O3 and O3-summer and exhaled 8-iso concentration (supplementary table E7). In models adjusted for both PM2.5 and O3, a similar result was found only between O3-summer exposure and exhaled 8-iso concentration (aβ −0.59, 95% CI −0.71– −0.47) (supplementary table E8). In models adjusted for both NO2 and O3, the negative associations between O3 and O3-summer and exhaled 8-iso concentration remained statistically significant (data not shown). In all participants, only O3-summer exposure was negatively and significantly associated with exhaled 8-iso concentration (aβ −0.33, 95% CI −0.55– −0.11) (data not shown). No association was found between outdoor air pollution and exhaled 8-iso concentration in participants with current asthma (data not shown).
Associations between outdoor air pollution and exhaled 8-isoprostane (8-iso) concentration among participants without asthma
Discussion
For the first time in adults, we found associations between long-term exposures to outdoor air pollution estimated at the individual level, exhaled 8-iso concentration and current asthma. Traffic intensity and O3 exposure significantly increased the risk of current asthma. Exhaled 8-iso concentration was positively and significantly associated with current asthma. Among participants without asthma, exhaled 8-iso concentration significantly increased with PM2.5 exposure, and decreased with O3 and O3-summer exposures.
Participants with asthma included in the present analyses were mostly recruited in chest clinics as asthma cases, with a careful procedure set up to include true asthmatic subjects using standardised and validated questionnaires. Others were recruited as first-degree relatives of asthmatic cases based on answers to questions on asthma diagnosis. This led to a group of asthmatic subjects with a wide range of disease expression. In our cross-sectional analyses, cause and consequence cannot be disentangled. It was not possible to study the associations between outdoor air pollution and exhaled 8-iso concentration with the incidence of asthma because only 30 new cases of asthma were reported at EGEA2. However, there is clearly a need for further research to confirm the associations and to clarify its causal underpinnings. Regarding exposure assessment, LUR models are well adapted to take into account the spatial variation of NO2, PM2.5 [19] and NOx [20], and ESCAPE resolution is accurate to estimate the exposure to markers of road traffic, which have a spatial heterogeneity. In addition, IFEN resolution is larger than ESCAPE, but suitable for O3 and O3-summer, which are homogeneous over long distances [21]. We acknowledge that a weakness of our study is the noncompliance of the temporality because outdoor air pollution was estimated by ESCAPE between 2009 and 2010, whereas the collection of EBC and phenotype “current asthma” took place at EGEA2 between 2003 and 2007. To obtain a better temporality in our analyses, we used the back-extrapolated pollution estimates, which were back-extrapolated at the participant's residential address at EGEA2, and found similar results. Both back-extrapolated and non-back-extrapolated estimates were highly and significantly correlated in our study (correlation coefficients ≥0.98; p<0.001), as previously reported by Beelen et al. [22] in the same ESCAPE project and for a longer period. Previously in the ESCAPE study, associations between NO2 back-extrapolated estimates and asthma incidence were similar to those with non-back-extrapolated estimates [23]. We aimed to study the impact of long-term exposure to outdoor air pollution and therefore conducted sensitivity analyses by excluding participants who lived at the same residential address for <1 year, which did not change our conclusions. We cannot exclude that some nondifferential misclassification of pollution exposure may have occurred because the time–activity patterns of participants were not available in our analyses, but in this case it would lead to bias towards the null. Furthermore, IFEN resolution can better represent participant's daily exposures to O3 and O3-summer, at least for those who work close to home. We could not take into account all indoor environmental factors; however, we found similar results after further adjustment for domestic exposure to cleaning products. Furthermore, adjustment for socioeconomic position potentially associated with pollutant exposures [24] and asthma also gave similar results. The EGEA study is a case–control and family study. Participants from the same family share a genetic background, and also socioeconomic and lifestyle factors, that could be associated with exposure to outdoor air pollution or asthma risk. We therefore took into account familial dependence through random effects in mixed models. Subgroup analyses suffer from a lack of power but, as best as possible, we used the most suitable statistical models. Finally, the enzyme immunoassay method has been preferred for dosing exhaled 8-iso concentration rather the gas chromatography–mass spectrometry method because the former is better adapted to analyse a larger number of samples, as in our study.
We found that traffic intensity and O3 exposure increased the risk of current asthma. Our results add evidence of the impact of long-term exposure to outdoor air pollution on asthma in adults. Our results are partly in accordance with those of a recent study showing that traffic exposure but not NO2 exposure, assessed by satellite-based LUR model at residential addresses, was positively associated with current asthma in 1367 adults [25]. We also found a positive association between O3 exposure and current asthma. To the best of our knowledge, the literature assessing the effects of outdoor air pollution on asthma has been focused mainly on other asthma phenotypes such as asthma onset, asthma severity or asthma control. A study conducted in California in the USA reported that long-term exposure to O3 was associated with development of asthma in adult males [26]. Previously in the EGEA study, long-term exposure to O3 estimated by IFEN was associated with asthma severity [17] and with uncontrolled asthma [27]. Recently, a cohort showed that asthmatic adults exposed to O3 had a greater risk of developing asthma–chronic obstructive pulmonary disease overlap syndrome [28]. Interestingly, various asthma phenotypes were studied such as asthma onset, which reflects the initiation of the disease, and severity and control of asthma, which are linked to manifestations of the disease. Asthma reflects both ever-asthma and current asthma, and the participants with ever-asthma did not necessarily have current asthma. In the EGEA study, the phenotype “current asthma” was defined by the report of respiratory symptoms or asthma attacks, or use of inhaled and/or oral medicines because of breathing problems in the past 12 months. To study the associations between long-term exposure to outdoor air pollution, biological markers and asthma, the phenotype “current asthma” was more relevant than the phenotype “ever-asthma” because it reflects the recent activity of the disease. Overall, all these findings add evidence of associations between outdoor air pollution and asthma in adults, whatever the studied phenotypes.
This study adds new insights into a potential role of oxidative stress in the associations between long-term exposure to outdoor air pollution and asthma in adults. We reported a significant association between exhaled 8-iso concentration and current asthma after adjustment for age, sex, smoking status and BMI. We investigated whether other asthma characteristics could explain this association, but we did not find any significant association between exhaled 8-iso concentration and duration of asthma, age of asthma onset, lung function or allergic sensitisation. Our results add new evidence to the previous associations reported in the literature on asthma severity and asthma control [12]. We found for the first time that exhaled 8-iso concentration was positively associated with PM2.5 exposure in participants without asthma. Unfortunately, we did not have back-extrapolated data for PM2.5. In France, the PM2.5 level has shown an overall decrease between 2002 and 2012, and the association between PM2.5 exposure and exhaled 8-iso concentration may be underestimated [29]. The literature has been mainly focused on short-term exposure to outdoor air pollution and on other biological compartments. In fact, short-term exposure to PM2.5 was previously found to be positively associated with EBC 8-iso concentration among healthy adolescents [30] and with 8-iso concentration in urine among adults [31]. We also found counterintuitive negative associations between O3 and O3-summer exposures and exhaled 8-iso concentration. Our results are not in accordance with those of a previous study showing that O3 exposure assigned to residential location was associated with higher plasma 8-iso concentration in 120 healthy students [32]. The inconsistency with our findings may be partially attributed to differences in the study design, biological compartment and spatial resolution, which was less accurate than in our study. We showed that O3 exposure and exhaled 8-iso concentration increased the risk of current asthma, and we did not expect negative associations between O3 and O3-summer exposures and exhaled 8-iso concentration. We investigated more thoroughly why these associations were negative. The analyses conducted by city showed that Paris heavily weighted the negative associations between O3 and O3-summer exposures and exhaled 8-iso concentration. Previously, a study has also reported a negative association between short-term exposure to O3 and exhaled 8-iso in adolescents in New York in the USA [33]. Another explanation is that O3 is a secondary pollutant mainly produced through complex chemical reactions from NO2. In our study, O3 and NO2 levels were highly and negatively correlated, and NO2 exposure was also positively associated with exhaled 8-iso concentration, but not significantly. One likely hypothesis is that the positive association between NO2 and exhaled 8-iso partly explained the negative associations observed for O3 and O3-summer. Overall, the specific effects of pollutants are hard to disentangle even in bipollutant models given the strong correlations between pollutants. It is interesting to note that participants from Paris had an exhaled 8-iso concentration seven times higher, and were exposed to higher levels of road traffic, NO2 and particulate matter, and to lower levels of O3 and O3-summer than in other cities, suggesting that Parisians may have particular characteristics that could partly explain the negative associations between O3 and exhaled 8-iso concentration. O3 and O3-summer were negatively correlated with PM2.5, but the negative association between O3-summer exposure and exhaled 8-iso concentration remained significant in a bipollutant model. Previously in EGEA adults, O3 assessed by IFEN was also found to be negatively associated with the EBC total nitrites/nitrates level, a biological marker of nitrosative stress [21]. In the literature, complex interplays between nitrosative and oxidative stress pathways have been reported [34], including a reciprocal regulation. An alternative explanation is that our results were likely due to other factors that are not included in the present analyses. In all participants, only a negative and significant association between O3-summer exposure and exhaled 8-iso concentration was found, and no association was found in participants with current asthma. In a directed acyclic graph, the covariate “current asthma” may be a collider, which makes the interpretation of our results even more difficult in a context of cross-sectional analyses [35].
Several biological mechanisms by which outdoor air pollution may be associated with asthma have been suggested in previous reviews [36, 37]. Outdoor air pollution exposure may increase oxidative stress in airways through the production of reactive oxygen species and local inflammation [9]. The particulate matter can act as supports for allergens and their small size gives them a large surface related to oxidative potential [38]. To disentangle the complexity of the associations between asthma and oxidative stress, and 8-iso in particular, there is a need for longitudinal epidemiological studies. Overall, our results add new insights into a potential role of oxidative stress in the association between long-term exposure to outdoor air pollution and asthma in adults. To better understand the underlying biological pathways between outdoor air pollution and asthma, future epidemiological studies should use individual portable sensors in order to improve the pollution assessment, study the different windows of exposure and try to collect multiple exposures in order to identify exposure profiles through clustering methods.
In conclusion, we found that traffic intensity, O3 exposure and exhaled 8-iso concentration increased the risk of current asthma, and that among participants without asthma exhaled 8-iso concentration increased with PM2.5 exposure, and decreased with O3 and O3-summer exposures. Exhaled 8-iso seems to be an interesting oxidative stress-related biomarker adapted to epidemiological studies. Overall, our study adds new insights into the associations between long-term exposure to outdoor air pollution and asthma in adults, and suggests that oxidative stress may partly explain such associations. Longitudinal studies with larger samples are now needed to confirm such results.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-02036-2017_Supplementary_material
Figure E1 ERJ-02036-2017_Figure_E1
Figure E2 ERJ-02036-2017_Figure_E2
Figure E3 ERJ-02036-2017_Figure_E3
Acknowledgements
The authors thank all those who participated in the setting of the study and in the various aspects of the examinations involved: interviewers, technicians for lung function testing and skin prick tests, blood sampling, IgE determinations, coders, those involved in quality control, data and sample management, and all those who supervised the study in all centres. The authors are grateful to the three CIC-INSERM centres of Necker, Grenoble and Marseille who supported the study and in which participants were examined. They are also grateful to the biobanks in Lille (CIC-INSERM) and at Annemasse (Etablissement Français du Sang) where biological samples are stored. They are indebted to all the individuals who participated, without whom the study would not have been possible. The authors thank N. Jeannée (Géovariances, Avon, France) and all those from the French Institute for Environment (Orléans, France), particularly M. Ba, for their work on the geospatial models.
The EGEA cooperative groupis as follows. Coordination: V. Siroux (epidemiology; Principal Investigator since 2013), F. Demenais (genetics), I. Pin (clinical aspects), R. Nadif (biology), F. Kauffmann (Principal Investigator 1992–2012). Respiratory epidemiology: INSERM ex-U700, Paris: M. Korobaeff (EGEA1), F. Neukirch (EGEA1); INSERM ex-U707, Paris: I. Annesi-Maesano (EGEA1 and 2); INSERM ex-U1018, Villejuif: F. Kauffmann, M.P. Oryszczyn (EGEA1 and 2); INSERM U1168, Villejuif: N. Le Moual, R. Nadif, R. Varraso; INSERM U1209 Grenoble: V. Siroux. Genetics: INSERM ex-U393, Paris: J. Feingold; INSERM U946, Paris: E. Bouzigon, F. Demenais, M.H. Dizier; CNG, Evry: I. Gut (now CNAG, Barcelona, Spain), M. Lathrop (now McGill University, Montreal, QC, Canada). Clinical centres: Grenoble: I. Pin, C. Pison; Lyon: D. Ecochard (EGEA1), F. Gormand, Y. Pacheco; Marseille: D. Charpin (EGEA1), D. Vervloet (EGEA1 and 2); Montpellier: J. Bousquet; Paris Cochin: A. Lockhart (EGEA1), R. Matran (now Lille); Paris Necker: E. Paty (EGEA1 and 2), P. Scheinmann (EGEA1 and 2); Paris Trousseau: A. Grimfeld (EGEA1 and 2), J. Just. Data and quality management: INSERM ex-U155 (EGEA1): J. Hochez; INSERM U1168: N. Le Moual; INSERM ex-U780: C. Ravault (EGEA1 and 2); INSERM ex-U794: N. Chateigner (EGEA1 and 2); Grenoble: J. Quentin (EGEA1 and 2).
Footnotes
This article has supplementary material available from erj.ersjournals.com
Conflict of interest: V. Siroux reports personal fees (speaker honorarium) from Teva, AstraZeneca and Novartis, outside the submitted work.
Support statement: Research was funded in part by the National Hospital Program of Clinical Research (PHRC-national 2012, EvAdA), ANR-CES-2009, Region Nord Pas-de-Calais, Merck Sharp & Dohme, the GA2LEN (Global Allergy and Asthma European Network) project and the Fonds AGIR pour les Maladies Chroniques. ESCAPE (FP7/2007–2011, grant 211250). Anaïs Havet is financed by CHU de Lille.
- Received October 5, 2017.
- Accepted February 22, 2018.
- Copyright ©ERS 2018