





Abstract
Asthma patients show evidence of a procoagulant state in their airways, accompanied by an impaired function of the anticoagulant protein C system. We aimed to study the effect of recombinant human activated protein C (rhAPC) in allergic asthma patients.
We conducted a randomised, double-blind, placebo-controlled, proof-of-concept study in house dust mite (HDM) allergic asthma patients. Patients were randomised to receive intravenous rhAPC (24 µg·kg−1·h−1; n=12) or placebo (n=12) for 11 h. 4 h after the start of infusion, a first bronchoscopy was performed to challenge one lung segment with saline (control) and a contralateral segment with a combination of HDM extract and lipopolysaccharide (HDM+LPS), thereby mimicking environmental house dust exposure. A second bronchoscopy was conducted 8 h after intrabronchial challenge to obtain bronchoalveolar lavage fluid (BALF).
rhAPC did not influence HDM+LPS induced procoagulant changes in the lung. In contrast, rhAPC reduced BALF leukocyte counts by 43% relative to placebo, caused by an inhibitory effect on neutrophil influx (64% reduction), while leaving eosinophil influx unaltered. rhAPC also reduced neutrophil degranulation products in the airways.
Intravenous rhAPC attenuates HDM+LPS-induced neutrophil migration and protein release in allergic asthma patients by an effect that does not rely on coagulation inhibition.
Abstract
Recombinant activated protein C attenuates allergen-induced migration of neutrophils to the bronchoalveolar space of asthma patients http://ow.ly/Rsevw
Introduction
Asthma is an obstructive respiratory disease accompanied by symptoms of recurrent dyspnoea, wheezing and chest tightness [1]. Severe allergic asthma is characterised by a mixed airway infiltration of eosinophils and neutrophils [2]. Chronic allergic lung inflammation may lead to irreversible lung damage, frequent asthma exacerbations and corticosteroid unresponsiveness in an important subgroup of asthma patients [1]. Therefore, there is a high urgency to develop new anti-inflammatory treatment strategies that improve allergic lung inflammation.
There is growing acceptance that allergic lung inflammation is accompanied by a pulmonary procoagulant and antifibrinolytic environment [3]. Regarding this interplay between allergic lung inflammation and coagulation in asthma, the anticoagulant protein C system has received particular attention, as it affects both inflammation and coagulation [4]. Activated protein C (APC), the end product of the protein C system, is primarily known for its anticoagulant effects through inactivation of clotting factors Va and VIIIa. In more recent years, APC has been shown to exert additional cytoprotective effects in different inflammatory settings that are independent of its anticoagulant properties [4, 5], including beneficial alterations in gene expression profiles, reduction of apoptosis and increasing endothelial barrier integrity. Recombinant human APC (rhAPC) (drotrecogin alfa) was registered for 10 years as an adjuvant treatment in adult multi-organ failure sepsis, until its retraction in 2011 for reasons of uncertainty of its effectiveness in this setting. Nonetheless, APC's anticoagulant and anti-inflammatory potential remains remarkable and the development of non-anticoagulant APC mutants with strong protective effects in a variety of inflammation models has fueled new interest in the protein C pathway as a therapeutic target [4, 5].
Asthma patients have decreased APC levels in bronchoalveolar lavage fluid (BALF) compared with healthy subjects both before and after allergen challenge [6]. Additionally, sputum of bronchial asthma patients showed reduced APC/thrombin ratios, suggesting insufficient upregulation of the protein C system in response to increased airway coagulation activation [7]. Data from a murine study showed a clear reduction in allergic lung inflammation by treatment with APC in an ovalbumin sensitisation and challenge model [8]. We hypothesised that restoration of the protein C pathway by administration of rhAPC would inhibit allergen-induced inflammation in patients with allergic asthma. In the current proof-of-concept trial we investigated the effects of rhAPC on allergic lung inflammation induced by intrabronchial allergen administration in patients with asthma.
Methods
Patients and design
We conducted a randomised, double-blind, placebo-controlled, proof-of-concept study in 24 house dust mite (HDM)-allergic asthma patients to study APC treatment in a setting of allergic lung inflammation (Netherlands Trial Register number 2943). The Medical Ethics Committee of the Academic Medical Center, Amsterdam (the Netherlands), approved the study and written informed consent was obtained from all patients. 4 h before allergen challenge, patients were randomly assigned to start on continuous intravenous infusion with rhAPC 24 μg·kg−1·h−1 (Eli Lilly, Indianapolis, IN, USA) or placebo (figure 1). rhAPC or placebo infusion was discontinued 1 h before the second bronchoscopy with BAL (see below) to minimalise bleeding risk during the BAL procedure. Segmental challenge was done via a bronchoscope as described with slight adjustments [6]. In short, a bronchoscopy was performed using a flexible fiberoptic videobronchoscope to instil one lung segment with saline (serving as a control) and a contralateral segment with a combination of HDM extract (50 biological units, Dermatophagoides pteronyssinus origin; ALK-Abello, Almere, the Netherlands) and lipopolysaccharide (LPS; from Escherichia coli, US standard reference endotoxin, 75 ng, kindly provided by Anthony Suffredini, National Institute of Health, Bethesda, MD, USA), seeking to mimic a clinically relevant and likely airway challenge [9, 10]. In total 28 patients were randomised. In four patients (one placebo, three rhAPC) the second bronchoscopy was not done by decision of the pulmonologist based on the presence of migraine in one patient and intolerance to introduction of the bronchoscope in three patients (none of these patients displayed asthma symptoms). All results relate to the 24 patients from whom BALF was obtained (12 rhAPC and 12 placebo treated patients), i.e., in whom effects could be determined. 8 h post-challenge, a bilateral BAL was performed for analyses [6]. Further details about patient screening, BAL handling procedures, measurements and assays are described in the online supplementary material.

Flow diagram of the study. APC: activated protein C.
Randomisation and masking
Randomisation was performed by using a closed envelope system supervised by the pharmacist. The patient and study team were blinded for treatment allocation. Measurements were performed blinded. After completion of the study the pharmacist provided the allocation key.
Statistical analysis
Comparison between two variables was performed using a T-test or Mann–Whitney U-test where appropriate. Serial data were analysed by two-way analysis of variance and Friedman's test for repeated measurements where appropriate. A p-value of <0.05 was considered statistically significant.
Results
Baseline characteristics
Table 1 shows baseline characteristics of both treatment groups. Groups were similar with respect to age, sex and type of asthma-related symptoms. All patients had intermittent-to-mild asthma severity (according to Global Initiative for Asthma criteria) and established HDM allergy, as reflected by similarly high D. pteronyssinus-specific IgE levels in both groups. There was a tendency to higher forced expiratory volume in 1 s (FEV1) (% of predicted) values in the rhAPC group compared with placebo (p=0.05). Otherwise, patient characteristics were similar.
Baseline patient characteristics
Clinical responses
Instillation of HDM+LPS did not induce clinical symptoms of asthma. There were no bleeding complications. One patient who had received rhAPC developed migraine; the infusion was stopped because of this and the headache disappeared spontaneously.
rhAPC has no impact on HDM+LPS induced pulmonary coagulation in allergic asthma
To monitor the anticoagulant effect of rhAPC in the circulation, we measured the activated partial thromboplastin time (APTT). Before start of therapy APTT was similar between groups (figure 2). As expected, patients infused with rhAPC had a prolonged APTT at t=0 (i.e., directly before allergen challenge; p<0.05 versus placebo) and t=8 h (p<0.01). HDM+LPS induced elevated thrombin–antithrombin complexes (TATc) and D-dimer BALF concentrations when compared with the saline side in both rhAPC (figure 3a and b; p<0.001 and p<0.05, respectively) and placebo-treated patients (p<0.01 and p<0.01, respectively). Remarkably, TATc and D-dimer levels measured in BALF from HDM+LPS challenged lung segments did not differ between rhAPC and placebo treated patients. In plasma, both TATc and D-dimer showed gradual increases during the study day (figure 3c and d), which were significant in both rhAPC (p<0.05 and p<0.01, respectively) and saline infused patients (p<0.05 and p<0.001, respectively). Although rhAPC tended to reduce plasma TATc (p=0.06) and D-dimer levels (p=0.08), differences with the placebo group were not significant. Considering that APC has been reported to exert an inhibitory effect on fibrinolysis by enhancing the release of plasminogen activator inhibitor type I (PAI-1) [5], we measured PAI-1 in BALF and plasma (figure S1). HDM+LPS challenge was associated with higher BALF PAI-1 levels in rhAPC (p<0.05 versus saline) and placebo-treated patients (p=0.05). BALF PAI-1 concentrations did not differ between treatment groups. In plasma, PAI-1 increased gradually during the study day in both patient groups (p<0.05). Although rhAPC tended to enhance this rise in plasma PAI-1, the difference with placebo-treated patients was not significant (p=0.06). Together, these data indicate that HDM+LPS elicits a procoagulant environment in the airways of patients with allergic asthma and that rhAPC infusion does not significantly alter this response.

Recombinant human activated protein C (rhAPC) prolongs activated partial thromboplastin time (APTT) in vivo. Horizontal arrows indicate differences within treatment groups during the day. Data are presented as mean±sem of 12 patients per group. *: p<0.05; ***: p<0.001.
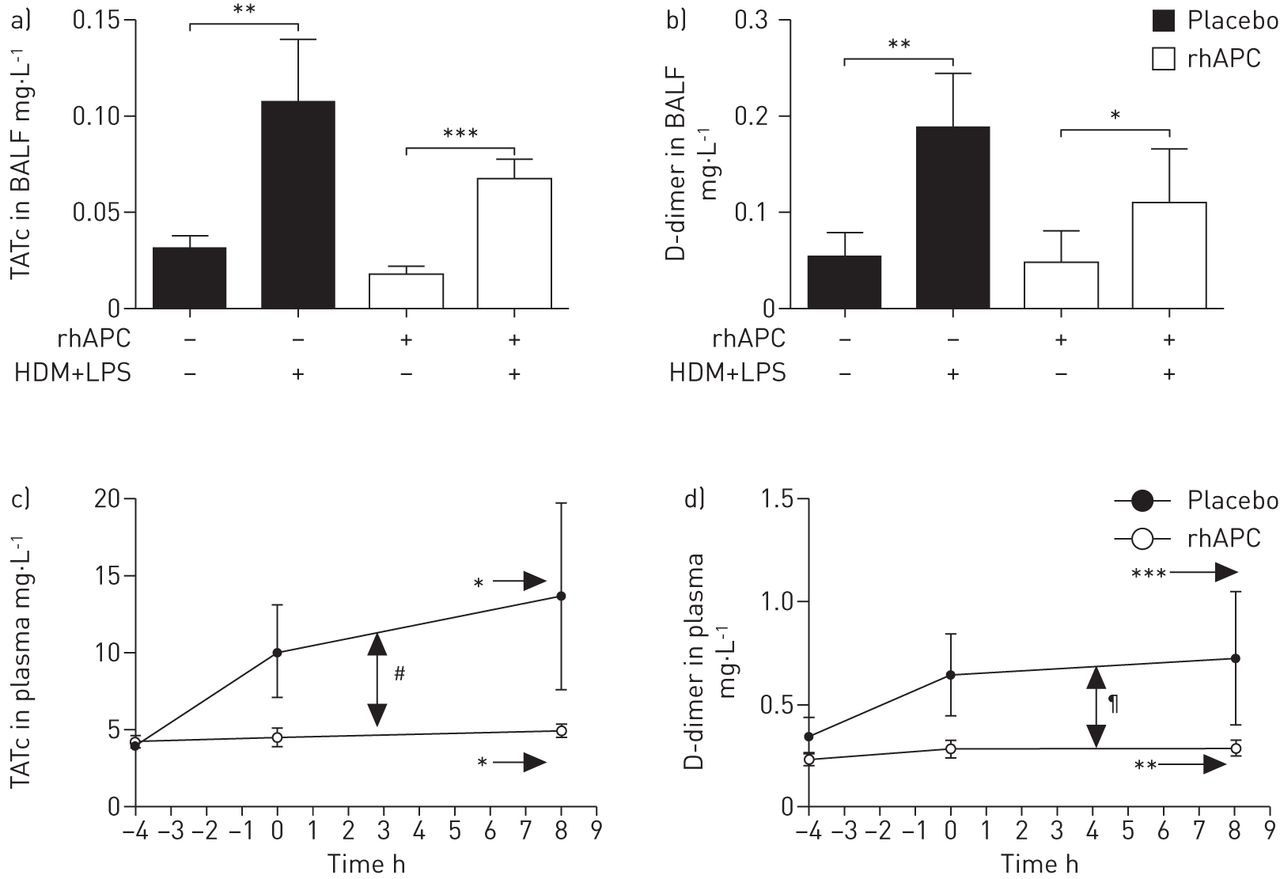
Recombinant human activated protein C (rhAPC) does not influence house dust mite extract and lipopolysaccharide (HDM+LPS)-induced coagulation activation and fibrinolysis inhibition. a) Thrombin–antithrombin complexes (TATc) in bronchoalveolar lavage fluid (BALF), b) D-dimer in BALF, c) TATc in plasma, and d) D-dimer in plasma. Horizontal arrows indicate differences within treatment groups during the day. Data are presented as mean±sem of 12 patients per group. *: p<0.05; **: p<0.01; ***: p<0.001; #: p=0.06; ¶: p=0.08.
rhAPC reduces HDM+LPS induced neutrophil influx in allergic asthma
Severe allergic asthma is characterised by a mixed cellular infiltration of the airways of eosinophils and neutrophils [2]. HDM+LPS instillation increased total leukocyte counts in BALF compared with saline (both p<0.001 for placebo and rhAPC groups), caused by an influx of eosinophils and neutrophils (figure 4a–c). rhAPC reduced mean leukocyte counts in HDM+LPS challenged lung segments by 43% relative to placebo (p<0.05). This inhibitory effect by rhAPC selectively involved neutrophils: whereas eosinophil numbers did not differ between treatment groups, rhAPC infused patients demonstrated a 64% reduction in mean neutrophil counts when compared to placebo-treated patients (p<0.05). Notably, rhAPC also reduced total leukocyte counts on the saline-challenged side compared with placebo (p<0.05); this effect was caused by a reduction in neutrophils counts; although, due to inter-individual variation, this difference did not reach statistical significance. Peripheral blood leukocyte (data not shown) and neutrophil counts (figure 4d) increased during the study day, whereas eosinophil numbers decreased ((data not shown, all p<0.001). These systemic responses were not influenced by rhAPC. Together, these results indicate that rhAPC selectively inhibits neutrophil recruitment into the airways upon local HDM+LPS challenge.

Recombinant human activated protein C (rhAPC) reduces house dust mite extract and lipopolysaccharide (HDM+LPS)-induced neutrophil influx. a) total leukocytes in bronchoalveolar lavage fluid (BALF), b) eosinophils in BALF, c) neutrophils in BALF, and d) blood neutrophils. Horizontal arrows indicate differences within treatment groups during the day. Data are presented as mean±sem of 12 patients per group. *: p<0.05; ***: p<0.001.
rhAPC does not influence the local release of neutrophil chemoattractants induced by HDM+LPS
Several chemokines and cytokines can attract neutrophils to the lungs, including interleukin (IL)-8, IL-1β, tumour necrosis factor α, macrophage inflammatory proteins 1α (CCL3) and 1β (CCL4). Levels of all of these mediators (table 2) were higher in HDM+LPS-challenged lung segments than in saline-instilled segments (non-significant for IL-8 in the placebo group). However, there were no differences between rhAPC and placebo-treated patients. Complement products too can attract neutrophils to sites of inflammation. C3a, C3bc and C4bc levels increased in BALF upon HDM+LPS challenge relative to saline administration. rhAPC did not alter this HDM+LPS-induced complement activation. C5a remained undetectable in BALF of all patients. CD11b is a β2-integrin implicated in neutrophil migration to the lungs. We therefore determined CD11b expression on blood and BALF neutrophils (figure S2). Pulmonary neutrophils showed increased CD11b expression compared with blood neutrophils, without differences between saline and HDM+LPS instilled lung segments. rhAPC did not affect neutrophil CD11b expression. Prostaglandin E2 can inhibit neutrophil migration. HDM+LPS induced an increase in BALF prostaglandin E2 concentrations relative to saline control in both groups, without effect of RhAPC (table 2). Together, these data suggest that rhAPC does not influence the local concentrations of neutrophil attractants. Similarly, rhAPC did not influence the HDM+LPS-induced release of eotaxin or soluble vascular cell adhesion protein-1, mediators implicated in eosinophil recruitment (figure S3).
Recombinant human activated protein C (rhAPC) does not influence the local release of neutrophil chemoattractants induced by house dust mite and lipopolysaccharide (HDM+LPS)
rhAPC attenuates HDM+LPS-evoked neutrophil degranulation in the airways of asthma patients
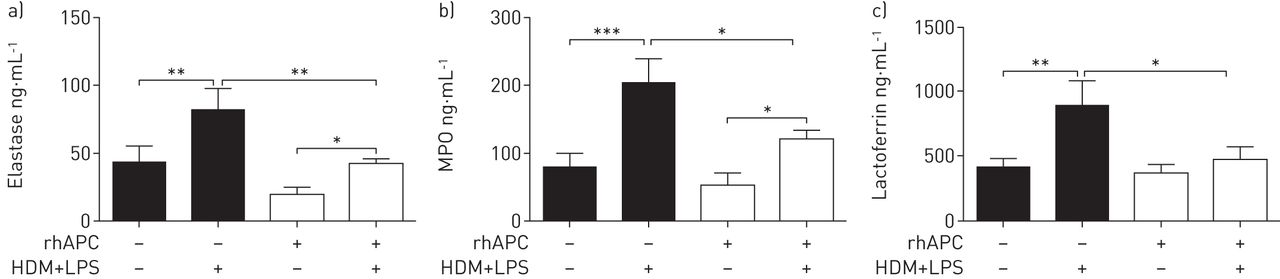
Enhanced release of neutrophil proteases within the respiratory tract has been implicated in airway inflammation in severe asthma [11]. Elastase is contained in azurophilic granules of neutrophils, together with myeloperoxidase (MPO). HDM+LPS challenge induced elevated BALF levels of elastase (figure 5a) and MPO (figure 5b) relative to saline administration (placebo: p<0.01 and p<0.001 for elastase and MPO, respectively; rhAPC: both p<0.05). Importantly, rhAPC infusion was associated with significantly lower concentrations of elastase (p<0.01) and MPO (p<0.05) in lung segments challenged with HDM+LPS. To test whether this anti-inflammatory effect of rhAPC was specific for azurophilic granules, we measured BALF levels of lactoferrin, which is a constituent of neutrophil-specific granules. HDM+LPS instillation induced an increase in BALF lactoferrin concentrations in placebo-treated patients (figure 5c, p<0.01 versus saline), but not in rhAPC-treated patients. In accordance, rhAPC infusion significantly reduced lactoferrin levels in HDM+LPS-challenged lung segments when compared with placebo treatment (p<0.05). These data show that levels of neutrophil degranulation products were lower in the airways of rhAPC treated asthma patients upon allergen challenge.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Recombinant human activated protein C (rhAPC) decreases the pulmonary house dust mite extract and lipopolysaccharide (HDM+LPS)-evoked increase of elastase, myeloperoxidase (MPO) and lactoferrin levels. Concentrations of bronchoalveolar lavage fluid (BALF) levels of a) elastase, b) MPO and c) lactoferrin. Data are presented as mean±sem of 12 patients per group. *: p<0.05; **: p<0.01; ***: p<0.001.
rhAPC does not influence T-helper cytokine release by HDM+LPS challenge
APC has been reported to inhibit the expression of T-helper type 2 cytokines in a mouse model of ovalbumin-induced allergic lung inflammation [8]. HDM+LPS instillation elicited rises in IL-5, IL-6 and IL-10 (figure S4) relative to saline administration; rhAPC did not impact hereon. IL-4 and IL-17 levels remained undetectable in all patients. Thymic stromal lymphopoietin, implicated in T-helper type 2 activation in allergic lung inflammation, was detectable at low levels in all samples, but no differences were detected between HDM+LPS and saline-challenged segments, or between rhAPC and placebo-treated patients (figure S5).
rhAPC does not modify vascular leak upon HDM+LPS challenge
APC can exert cyto- and barrier-protective effects on endothelial cells [5]. We determined the quotients of albumin and α2-macroglobulin levels in BALF and serum (QAlb and QA2M, respectively) and the relative coefficient of excretion (QA2M/QAlb) as measures of the permeability of the blood–airway barrier [12]. HDM+LPS instillation was associated with significant increases in QAlb (figure S6a; p<0.01 versus saline) and QA2M (figure S6b; p<0.001 versus saline) and relative coefficient of excretion (figure S6c; p<0.001 versus saline). These HDM+LPS effects were not altered by rhAPC (figure S6a–c). In accordance, HDM+LPS elicited rises in total protein levels (figure S6d) and in the number of vascular endothelial cadherin-positive microvesicles in BALF (figure S6e), which were not influenced by rhAPC infusion.
Discussion
In recent years, local activation of the coagulation system in the airways has been implicated as a pathophysiological mechanism contributing to allergic inflammation and asthma [3]. Here, we report a proof-of-concept trial that sought to determine the effect of rhAPC, a protein with distinct anticoagulant and cytoprotective properties, on allergen-induced lung inflammation in patients with asthma. The main finding of our study was that rhAPC reduces neutrophil recruitment and degranulation products in the bronchoalveolar space challenged with allergen. Considering the role of neutrophils in severe refractory asthma [13], these findings may have particular relevance for this patient category, in which conventional asthma therapies are less effective.
We used segmental challenges with HDM+LPS via a bronchoscope, a technique previously adopted by our and other groups to model allergic lung inflammation [6]. HDM was chosen as challenge since it is a frequent allergen source with high sensitisation rates in asthma populations [14]. We added low-dose LPS as a natural and relevant adjuvant [9]. LPS is a component of the gram-negative bacterial cell wall and an environmental pollutant that has been associated with the frequency of asthma symptoms [10]. Previously, we have shown that in mice HDM+LPS elicits a mixed eosinophil and neutrophil influx into the airways [15], and subsequently confirmed this observation in patients with mild asthma [16]. The dosages chosen for both HDM and LPS are within the range of levels detected in patient's homes. Co-exposure of HDM with LPS is not only a likely clinical event, but also may have relevance for asthma pathogenesis because the HDM allergen Der-p2 is structurally and functionally similar to the endogenous LPS-binding protein MD-2. By forming lipid-carrying sacks, HDM allergens act as carriers of LPS into the pulmonary compartment [17]. There is increased interest in studying asthma phenotypes characterised by mixed neutrophilic and eosinophilic infiltrates, since airway neutrophilia has been linked with severe asthma, refractory asthma and corticosteroid unresponsiveness [13].
Studies have revealed that both mouse and human neutrophils are important in the pathobiology of anaphylaxis and allergic inflammation via an IgG and FcγRIIA-dependent pathway [18]. rhAPC inhibited HDM+LPS-induced neutrophil influx into the airways without affecting eosinophil recruitment. In accordance, rhAPC reduced neutrophil influx upon segmental LPS challenge in healthy humans [19], and inhibited IL-8-directed [20] and integrin-mediated neutrophil migration [21]. Chronically elevated levels of elastase and MPO can lead to lung damage and thus could contribute to the association between neutrophils and asthma severity [13]. Asthma patients demonstrate increased elastase activity in sputum, correlating with worse clinical outcomes [22]. Neutrophil serine enzymes (most notably elastase) can enhance eosinophil effector functions, such as superoxide generation and cytokine/chemokine secretion [23]. In accordance, elastase inhibitors reduced allergen induced goblet cell degranulation in guinea pigs [24] and prevented eosinophilic inflammation, T-helper type 2 cytokine production and goblet cell metaplasia in an ovalbumin sensitisation and challenge model in mice [25]. Interestingly, APC reduced elastase induced lung injury in mice [26], suggesting that this drug influences neutrophil responses by multiple mechanisms. rhAPC also diminished the concentrations of lactoferrin, a constituent of neutrophil specific granules, of which the capability to activate eosinophils is of special interest in the context of asthma [27].
Intrapulmonary HDM+LPS exposure caused elevated levels of TATc, D-dimer and PAI-1 in BALF, indicating that allergic lung inflammation is associated with a pulmonary procoagulant and anti-fibrinolytic environment. Intriguingly, rhAPC did not prohibit HDM+LPS-induced pulmonary coagulation. In contrast, in a previous study, rhAPC treatment exerted anticoagulant effects after LPS exposure of the airways in healthy volunteers [28]. This discrepancy may be due to differences in the extent of coagulation activation, as indicated by the fact that BALF mean TATc levels were ∼50-fold higher in the present study. This difference in BALF TATc levels was not due to a higher LPS challenge dose, which was ∼25% of the LPS dose administered in the earlier study in healthy humans [28]. Apparently, the strong procoagulant response evoked by HDM+LPS in the pre-existing procoagulant environment in the airways of asthma patients cannot be inhibited by the usual intravenous dose of rhAPC. Together, these data suggest that the anticoagulant properties of rhAPC have little if any role in the inhibition of neutrophil influx and degranulation by this compound. This finding is important for the possible clinical implications and the current development of APC mutants that lack anticoagulant effects. These mutants display intact cytoprotective properties and are as effective as wild-type APC in reducing lethality in preclinical sepsis models. Moreover, a recent investigation showed that non-anticoagulant APC can inhibit acute lung inflammation elicited by Pseudomonas aeruginosa [29]. Non-anticoagulant APC mutants have the considerable advantage that they are not associated with increased bleeding risk, which has been a major concern for rhAPC in clinical practice in the past. Importantly, one of these selective APC mutants has reached the clinical testing phase. Considering the results of the current trial, it would be of interest to explore the efficacy of these APC mutants in patients with exacerbations of allergic asthma.
In a mouse model of lung inflammation induced by ovalbumin sensitisation and challenge inhalation of APC strongly attenuated allergic inflammation as reflected by a reduced influx of eosinophils and lower levels of the T-helper type 2 cytokines IL-4, IL-5 and IL-13 in BALF [8]. In our current study, intravenous infusion of rhAPC did not reproduce these effects, which at least in part can be explained by differences in species, allergen provocation and route of APC administration. Although intrapulmonary delivery of rhAPC may seem attractive, this approach is not feasible with the present product. Indeed, we recently reported unexpected exaggerated procoagulant and proinflammatory effects of intrabronchial rhAPC administration in healthy humans challenged with LPS via the airways [30]. In addition, APC has strong anti-inflammatory and barrier protective effects on endothelial cells [5], which are targeted better by intravenous infusion. Nonetheless, we were not able to detect barrier protective effects of rhAPC, as reflected by unaltered parameters of increased blood-airway permeability in HDM+LPS-challenged lung segments.
In conclusion, here we show that intravenous rhAPC infusion attenuates HDM+LPS-induced neutrophil migration and protease release in allergic asthma patients by an effect that did not rely on local inhibition of coagulation. This proof-of-concept study may have implications for the development of new anti-inflammatory treatment strategies in severe refractory asthma wherein neutrophils play an important role in chronic inflammation and acute exacerbations.
Acknowledgements
We want to thank E.M. Kemper and E.S. Brans from the hospital's pharmacy (Academic Medical Center, University of Amsterdam, Amsterdam, the Netherlands) for their help with study protocols.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Clinical trial: This study is registered at www.trialregister.nl with identifier number 2943
Support statement: J. Daan de Boer and Christof J. Majoor are supported by the Netherlands Asthma Foundation (projects 3.2.08.009 and 3.2.11.021 respectively).
Conflict of interest: None declared.
- Received March 21, 2015.
- Accepted June 28, 2015.
- Copyright ©ERS 2015
References










