





Abstract
Mannitol challenge is a promising diagnostic test for cough hypersensitivity syndrome http://ow.ly/gWf530j9O7H
To the Editor:
Cough is the most common reason why people seek medical attention [1]. Cough hypersensitivity syndrome (CHS) is a new concept to describe a condition with long-standing hypersensitivity of vagal afferent nerves or an alteration of the central processing of their input regardless of the underlying cause [2]. The current definition of CHS is purely clinical; however, a test capable of demonstrating this hypersensitivity both reliably and feasibly might be used as a diagnostic test for CHS.
The traditional cough provocation tests using capsaicin or citrate are limited by a wide normal range of the responses [3] and the measured cough sensitivity poorly correlates with the subjective symptoms [4]. Cough provocation testing using hypertonic saline can separate asthmatic from healthy subjects [5] and the level of cough responsiveness is correlated with the subjective symptoms [6]. However, this test requires complex technology and therefore may not be feasible to diagnose CHS.
The mannitol challenge is a regulatory approved bronchial provocation test. It is similar to hypertonic saline, providing an osmotic stimulus to airways and provoking cough, but can be administered using a simple powder inhaler [7, 8]. Thus, it might be a feasible diagnostic test for CHS. Cough sensitivity to mannitol separates asthmatic subjects from healthy subjects [7]. However, another study found a large overlap in the cough sensitivity to mannitol between healthy subjects and subjects with chronic cough [9]. The present study was performed to determine whether cough sensitivity to mannitol inhalation challenge can separate subjects with chronic cough from those without, and whether subjective cough severity is associated with the cough sensitivity to mannitol.
This was a prospective study including 15 healthy subjects and 69 consecutive symptomatic patients who were referred to a respiratory function laboratory for mannitol challenge as part of their clinical evaluation. Among the symptomatic patients, there were 17 subjects with chronic (over 8 weeks’ duration) cough as their primary symptom. This group was defined as the “cough” group and the remaining 52 as the “other symptoms” group (usually dyspnoea or wheezing).
All subjects completed the Leicester Cough Questionnaire (LCQ) [10]. Increasing doses of mannitol powder were administered starting with an empty capsule, followed by 5, 10, 20, 40, 80, 160, 160 and 160 mg doses [11]. 60 s after each dose, two forced expiratory volume in 1 s (FEV1) manoeuvres were obtained. The challenge was video recorded and two scorers counted the coughs afterwards. The mean value was used for analysis. The cough sensitivity to mannitol was expressed by coughs-to-dose ratio (CDR), the total number of provoked coughs divided by the cumulative amount of mannitol, expressed as coughs per 100 mg of mannitol [7], and by C5, the first noncumulative mannitol dose that provoked five or more coughs. Mann–Whitney and Kruskal–Wallis tests were used to analyse differences between groups, and Spearman correlation coefficient (rs) to analyse associations. The study protocol was approved by the Ethics Review Committee of the Sydney Local Health District (Royal Prince Alfred Hospital zone), number X11-0249.
The mean (95% CI) age of the subjects was 34.3 (31.2–37.5) years with 50% females. The mean FEV1 was 101% (98–104%) of predicted among the symptomatic subjects and 15 of them showed a >15% fall in FEV1 during the challenge.
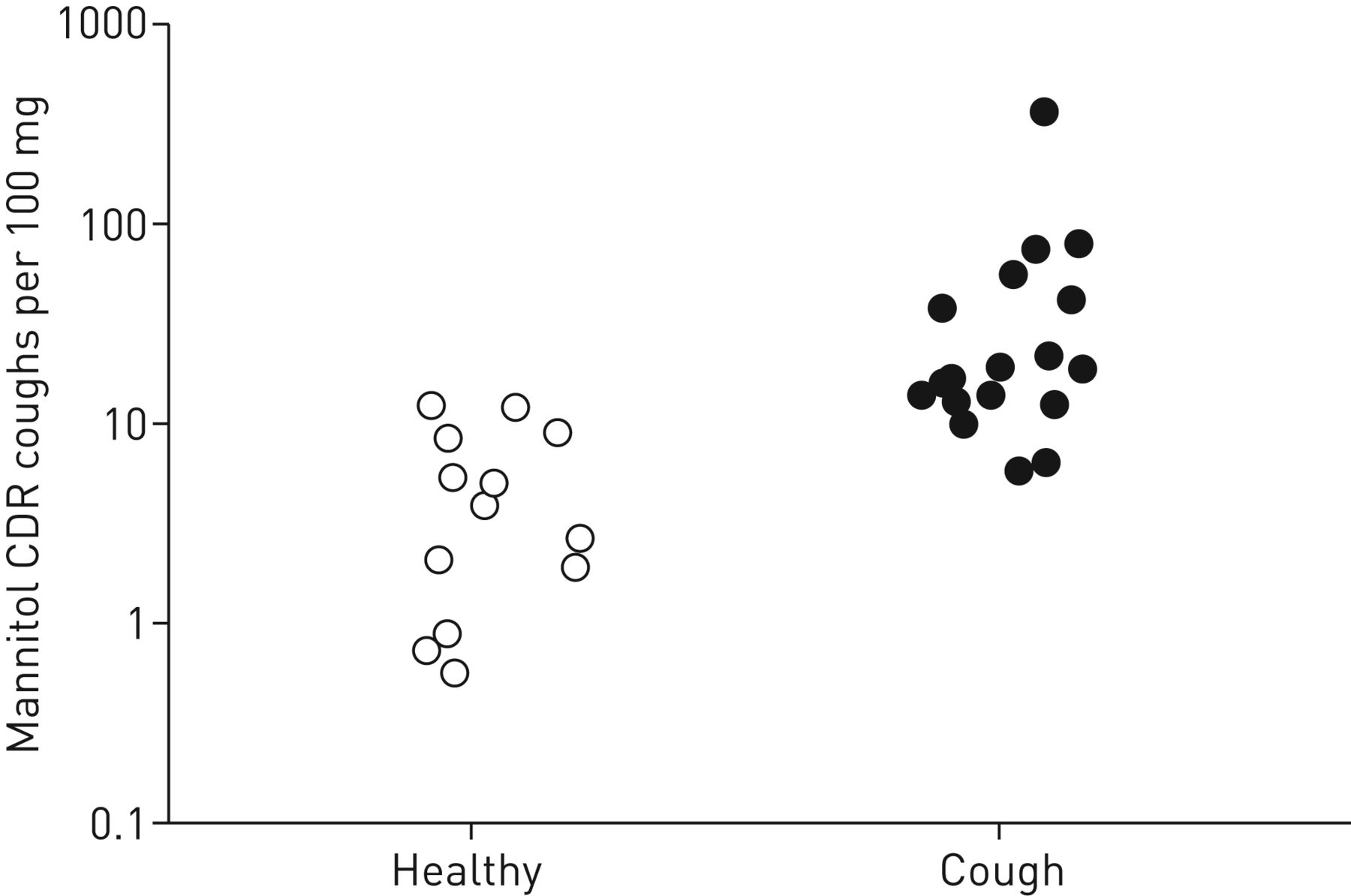
The cough group was significantly more sensitive to the cough-provoking effect of mannitol than the subjects with other symptoms and the healthy subjects (CDR 21.1 (12.6–35.4), 6.2 (4.2–9.4) and 2.8 (1.3–6.1) coughs per 100 mg, respectively; p<0.001 between cough and healthy subjects (figure 1), and p=0.002 between cough and other symptoms; C5 9.2 (5.8–14.7), 57.3 (38.9–84.6) and 116 (60.0–225) mg, respectively; p<0.001 between cough and healthy subjects, and p<0.001 between cough and other symptoms). There was a significant association between the LCQ total score and CDR both within the group “cough” (rs=0.50, p=0.04) and within all symptomatic subjects (rs=0.43, p<0.001). The cough sensitivity to mannitol was higher in women than in men among the symptomatic subjects (CDR 18.4 (12.9–26.2) versus 4.3 (2.6–7.0) coughs per 100 mg, respectively; p<0.001).
The present study demonstrates that the cough sensitivity to mannitol inhalation challenge clearly separates subjects with chronic cough both from healthy subjects and from subjects with other airway symptoms. Furthermore, mannitol cough sensitivity was correlated with the LCQ, a validated cough-related quality of life questionnaire.
Our study corroborates the previous studies with asthmatic patients in finding a large difference and small overlap in the cough sensitivity to hypertonicity between healthy subjects and the subjects with cough [5, 7, 12]. However, there is a previous mannitol study showing a relatively large overlap [9]. The main reason for this discrepancy is probably the very mild cough among the patients in the previous study. The mean LCQ total score was 17.3 among the chronic cough patients and 20.9 among the healthy subjects, with the difference just reaching statistical significance. By comparison, the mean LCQ total score among the subjects with chronic cough in the present study was 13.9, indicating much more severe cough. The present and the previous mannitol study differ also in many other aspects, including the ways in which the coughs were recorded and how the response was expressed.

{kind=link}
The coughs-to-dose ratios (CDRs) among 15 healthy subjects and 17 subjects with chronic cough (p<0.001 between the groups, Mann–Whitney test). The best cut-off value to separate the groups was 12.0 coughs per 100 mg. The vertical axis is logarithmic.
As mentioned, the traditional cough provocation tests using capsaicin or citrate usually show a wide normal range of the responses [3] and the measured cough sensitivity correlates poorly with the subjective symptoms [4]. Thus, there are important differences between traditional cough provocation tests and hypertonic aerosol cough provocation tests. The reasons for these are not clear. Capsaicin and, at least partly, citrate act via directly stimulating the transient receptor potential vanilloid 1 (TRPV1) receptor in the sensory nerves [13]. On the contrary, hypertonicity does not stimulate TRPV1 [14]. The most probable receptor to detect changes in osmotic homeostasis is TRPV4 [13]. Afferent Aδ and C fibres with cell bodies located in jugular ganglia are specifically sensitive to hypertonicity [15]. The repeatedly documented association between the cough sensitivity to hypertonicity and the subjective cough severity suggests that these fibres play a key role in CHS.
The fact that mannitol challenge not only measures the cough sensitivity but also the airway hyperresponsiveness is clinically useful, providing the possibility to simultaneously diagnose asthma, one of the most common causes of chronic cough.
There are several shortcomings in the present study. It would have been desirable for the group “cough” to be larger. More information about the cough background disorders would also have been useful. The strengths of the study include the representative sample of patients: they were referred to a respiratory function laboratory by independent physicians as part of real-life clinical evaluation. The accurate way of recording the coughs is also strength, as the challenges were video recorded and two scorers counted all coughs from the recordings afterwards.
In conclusion, the cough sensitivity to mannitol can identify subjects with chronic cough and this sensitivity is associated with the subjective cough severity. Since the mannitol challenge is regulator approved and can be performed without complex technology in a highly standardised fashion, it seems to be a promising diagnostic test for CHS. Studies with larger and better defined populations are now warranted.
Acknowledgements
The authors would like to acknowledge the assistance of Peter Briffa and Phillip Munoz (both Dept of Respiratory Sleep Medicine, Royal Prince Alfred Hospital, Camperdown, and Central Clinical School, Faculty of Medicine, The University of Sydney, Sydney, Australia) with their assistance in the cough counting.
Footnotes
Author contributions: All authors made substantial contributions to the conception and design of the work, and acquisition, analysis or interpretation of data for the work, drafted the article or revised it critically for important intellectual content, and gave final approval of the version to be published. All authors agreed to be accountable for all aspects of the work, in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of interest: H.O. Koskela reports receiving grants from Kuopion Hengityssäätiö, personal fees from Mundipharma Ltd, Orion Pharma Ltd, Oy, Eli Lilly Finland Ltd and Boehringer Ingelheim Finland Ltd as payments for giving scientific lectures at gatherings organised by medical companies, and personal fees from Takeda Leiras Ltd and Mundipharma Ltd to visit international scientific meetings, and owns shares in Orion Pharma Ltd.
Conflict of interest: C. Lake reports that the Royal Prince Alfred Hospital receives royalties for the sale of Aridol but no longer receives royalties for sales in Australia.
Conflict of interest: K. Wong reports that the Royal Prince Alfred Hospital receives royalties for the sale of Aridol but no longer receives royalties for sales in Australia.
Conflict of interest: J.D. Brannan reports receiving royalties for the sale of Aridol/Osmohale and owns shares in Pharmaxis.
- Received August 16, 2017.
- Accepted March 6, 2018.
- Copyright ©ERS 2018
References










