





Abstract
Under optimal conditions we observed similar rates of relapse-free cure in patients with M/XDR-TB and non-M/XDR-TB http://ow.ly/SRvd30hPu73
To the Editor:
Multidrug-resistant (MDR) tuberculosis (TB), defined by bacillary resistance against rifampicin and isoniazid, has been identified as a global threat to mankind [1]. According to the latest report by the European Centres for Disease Prevention and Control, and World Health Organization (WHO) regional office for Europe, only approximately 50% of MDR-TB patients in Europe reach favourable treatment outcomes [2]. Successful treatment outcomes are achieved for less than 25% of patients with extensively drug-resistant (XDR)-TB (MDR plus resistance against a least one fluoroquinolone and one second-line injectable drug) in the European Union/European Economic Area Countries [2].
Recently, new diagnostic methods and novel drugs have been introduced that may improve treatment outcomes in countries where these innovations are available to provide personalised therapies [3–6]. In order to evaluate treatment outcomes in M/XDR-TB under unrestricted healthcare conditions, and to ascertain the difference in treatment outcome for patients with drug-susceptible TB, we performed a multicentre prospective observational cohort study in patients with M/XDR- and non-M/XDR-TB at clinical centres in Germany. We sought to compare existing WHO and newly described “simplified” treatment outcome definitions for both M/XDR- and non-M/XDR-TB patients [7, 8].
Patients with pulmonary TB confirmed by the GeneXpert MTB/RIF test (Cepheid, Sunnyvale, CA, USA) were enrolled at five hospitals in Germany (Medical Clinic, Research Center Borstel; Karl-Hansen-Klinik, Bad Lippspringe; Sankt Katharinen-Krankenhaus, Frankfurt; Thoraxklinik-Heidelberg, Heidelberg; Asklepios Fachkliniken München-Gauting, Munich) between March 2013 and March 2016. Patients less than 18 years of age, those HIV-positive, or individuals under legal supervision were excluded from the study. Written informed consent was obtained from all patients.
Samples with a positive GeneXpert result for rifampicin resistance were further analysed by using line-probe-assays (Hain Lifesciences, Nehren, Germany) for the detection of additional first- and second-line drug resistance. Findings were later confirmed by culture based drug susceptibility tests (DST) at the national reference centre for mycobacteria in Borstel, Germany. Individualised anti-TB drug regimens for patients with M/XDR-TB were designed using current therapy recommendations on the basis of molecular and phenotypic DST [9, 10]. The algorithms were mainly in consent with the current WHO guidelines [11]. However, the preferred usage of certain drugs changed over time (i.e. linezolid). Patients with non-M/XDR-TB were treated following national recommendations [12]. In addition to WHO-defined outcome definitions [8], we applied simplified outcome definitions that include a 1-year follow-up to both patient groups. According to the simplified outcome definitions [7]: 1) cure is defined as a negative culture status 6 months after treatment initiation, no positive culture thereafter, and no relapses within 1 year after treatment completion; 2) treatment failure is defined as a positive culture status 6 months after treatment initiation or thereafter, or a relapse within 1 year after treatment completion; 3) undeclared outcome is defined as an outcome that cannot be classified (owing to transferal out of the cohort, no culture status at 6 months while the patient was receiving care, or no post-treatment assessment); 4) death is defined as death during observation; 5) loss to follow-up is defined as non-receipt of care 6 months after treatment initiation.
For the follow-up 1-year after therapy end, patients were contacted by telephone interviews or/and during routine clinical follow-up visits. Study approval was granted by the Ethics Committee of the University of Lübeck (AZ 12–233), which subsequently was confirmed by the corresponding local ethic committees of all participating centres. Statistical analyses were performed using STATA (Version 14, StataCorp LLC, College Station, TX, USA).
75 patients were enrolled, of whom 46 were infected with non-M/XDR and 29 with MDR strains of M. tuberculosis. Of the 29 patients with M/XDR-TB, eight patients were infected with an XDR strain of M. tuberculosis. In the cohort of non-M/XDR-TB patients, two patients had isoniazid mono-resistant TB. Only three of 29 (10.4%) M/XDR-TB patients received an anti-TB regimen containing bedaquiline or delamanid, which became available during the study period. Of the 22 of 29 (75.9%) M/XDR-TB patients receiving fluoroquinolones, 18 of 22 (81.8%) were treated with moxifloxacin while four of 22 (18.2%) received levofloxacin. 21 of 29 (72.4%) M/XDR-TB patients were administered second-line injectable drugs, of whom 14/21 (66.7%) patients received capreomycin and 7/21 (33.3%) amikacin.
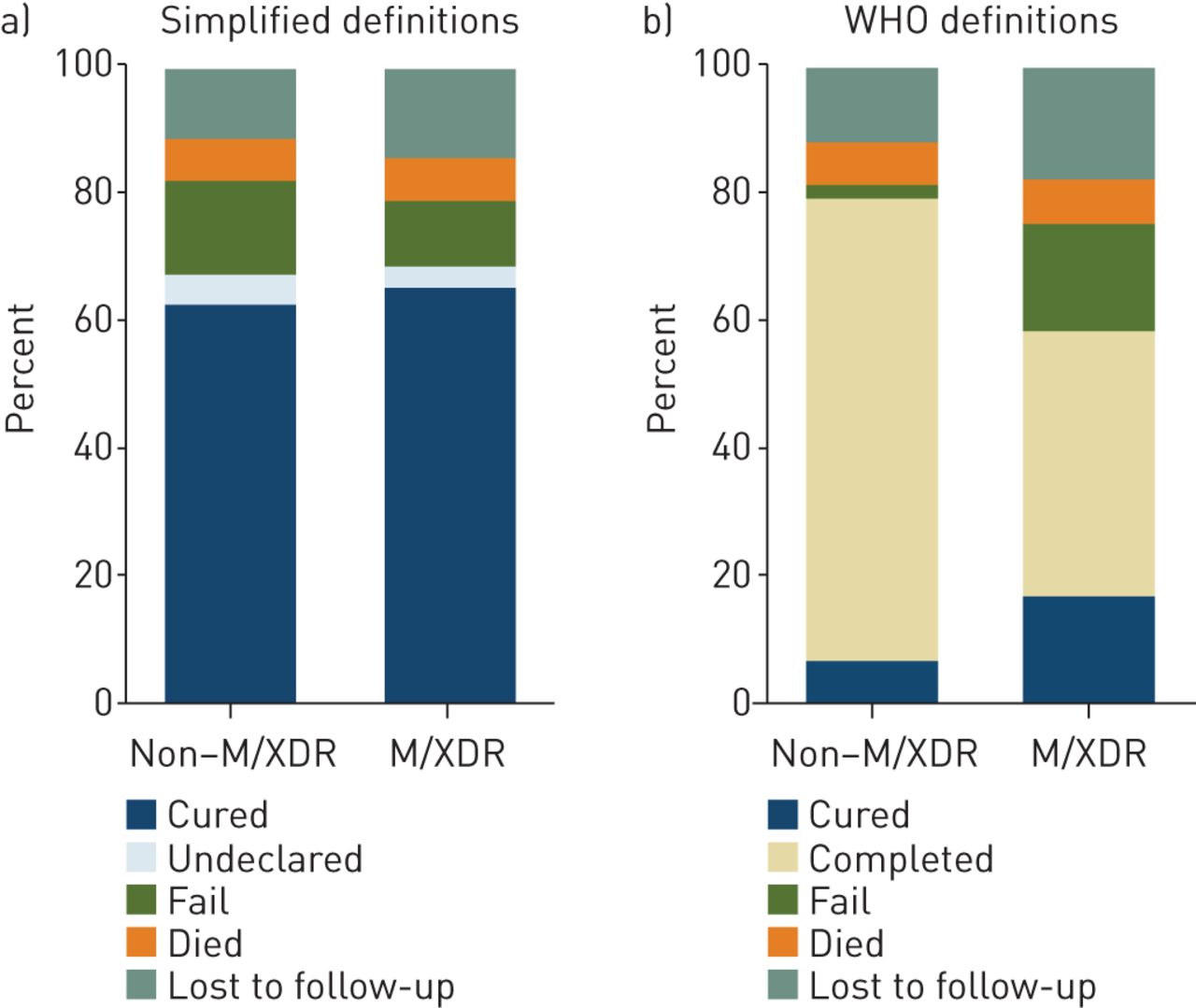
Patients with M/XDR- and non-M/XDR-TB showed similar frequencies of relapse-free cure (65.5% and 63.0%, respectively; p=0.828), as they did for death and failure (figure 1). Just eight patients (three M/XDR-TB, five non-M/XDR-TB) achieved cure by WHO definitions. Treatment success by WHO definition, driven by treatment completion, was markedly lower for M/XDR-TB patients (58.6%) compared to non-M/XDR-TB patients (76.1%; p=0.110). Given the relatively low number of patients, we could not identify any characteristics associated with treatment failure (Simplified outcomes: non-M/XDR-TB, n=7 versus M/XDR-TB, n=3).
{kind=link}
Treatment outcomes for patients with and without multidrug-resistant/extensively drug-resistant tuberculosis (M/XDR-TB) by a) simplified (TBNET) and b) World Health Organization (WHO) definitions. The simplified outcomes yielded the following results: death: non-M/XDR-TB, n=3 (6.5%) versus M/XDR-TB, n=2 (6.9%); lost to follow-up: non-M/XDR-TB, n=5 (10.9%) versus M/XDR-TB, n=4 (13.8%); failure: non-M/XDR-TB, n=7 (15.2%) versus M/XDR-TB, n=3 (10.3%); cure: non-M/XDR-TB, n=29 (63.0%) versus M/XDR-TB, n=19 (65.5%); undeclared: non-M/XDR-TB, n=2 (4.4%) versus M/XDR-TB, n=1 (3.5%). Outcomes following the WHO definitions were: death: non-M/XDR-TB, n=3 (6.5%) versus M/XDR-TB, n=2 (6.9%); lost to follow-up: non-M/XDR-TB, n=5 (10.9%) versus M/XDR-TB, n=5 (17.2%); failure: non-M/XDR-TB, n=1 (2.2%) versus M/XDR-TB, n=5 (17.2%); cure: non-M/XDR-TB, n=3 (6.5%) versus M/XDR-TB, n=5 (17.2%); completed: non-M/XDR-TB, n=32 (69.6%) versus M/XDR-TB, n=12 (41.4%); not evaluated: non-M/XDR-TB, n=2 (4.4%) versus M/XDR-TB, n=0 (0.0%). Total for both analyses: non-M/XDR-TB, n=46 (100%) versus M/XDR-TB, n=29 (100%).
Under optimal management conditions and resources we observed similar frequencies of relapse-free cure in patients with M/XDR-TB and non-M/XDR-TB when applying outcome definitions that include a 1-year follow-up period after the completion of treatment [7]. The lack of marked differences in treatment response between the two groups using new definitions is encouraging and stands in sharp contrast to the low frequency of WHO-defined cure for patients with TB ascertained on the last day of treatment. Frequency of treatment success by WHO definition (the sum of those who achieve cure or complete their treatment in the absence of failure) is nearly identical to the estimates reported by the European Centre for Disease Prevention and Control surveillance data [2]. A recent multi-national observational cohort study in Europe showed that WHO-defined treatment success is largely based on treatment completion rather than on cure [7, 8]. This was confirmed in the present study where only 6.5% of patients with non-M/XDR-TB were cured and 69.6% of patients had treatment completion. The main reason for the absence of cure is lack of the required number of sputum samples in the final stage of treatment.
Prevention of relapse is the main purpose for the long duration of therapy in TB. Thus, definition of “cure from TB” should include a relapse-free observation period after the end of therapy, which is already the case in anti-TB drug trials [13]. In the field of oncology, where there is also the risk of disease recurrence after the termination of therapy, determining cure (corresponding to end-points such as progression-free survival) at the last day of chemotherapy without the implementation of a follow-up period would be unacceptable [14]. The majority of the relapse cases occur within 12 months of treatment completion making an observation period of 1 year plausible to define relapse-free cure, as was recently demonstrated [7, 13]. A negative M. tuberculosis culture status after 6 months of treatment, as the critical assessment point for the simplified definitions, has been shown to be predictive for cure in MDR-TB [7, 15]. The current study shows that applying the same outcome definitions for patients with non-M/XDR-TB and M/XDR-TB gives plausible results in line with clinical experience. This opens the door to adopt a single set of outcome definitions for all pulmonary TB patients, regardless of resistance pattern or duration of therapy. Such a move will simplify and improve outcome reporting. Recently, two groups have demonstrated 6-month culture conversion rates of 96% [16] and 100% [17] in patients with M/XDR-TB treated with bedaquiline-based regimens providing hope that much higher cure-rates from M/XDR-TB can be achieved in the future.
One limitation of the study is a potential selection bias in non-M/XDR patients, since they were not strictly consecutively enrolled due to staff shortage at the participating centres. Enrolment was not related to patient characteristics, which makes the probability for bias small. Furthermore, non-M/XDR-TB patients have a similar sex and age distribution as notified TB patients in Germany in general.
In conclusion, in a country where sufficient resources for the management of patients with M/XDR-TB are available, we now observe substantial improvements in treatment outcomes resulting in a high frequency of relapse-free cure indistinguishable from cure in patients with non-M/XDR-TB. This “honeymoon” may last until strains of M. tuberculosis that have developed resistance against novel and refurbished second-line drugs start circulating in the community. WHO treatment outcome definitions for TB should be revised to describe cure only in the in the absence of disease recurrence 1 year after the end of treatment.
Acknowledgements
We thank Cordula Ehlers, Jessica Hofmeister, Franziska Daduna, Nelleke Smitsmann, and Dagmar Schaub for the study management and data entry.
Footnotes
Support statement: The study was funded by the German Center for Infection Research (DZIF). Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: J. Heyckendorf has received personal fees for lecturing at sponsored symposia from Chiesi, Gilead, Janssen and Lucane, outside the submitted work.
Conflict of interest: B. Kalsdorf has provided independebt lectures for Lucane Pharma and Oxford Immunotec, outside the submitted work.
Conflict of interest: H.J.F. Salzer has received honoraria for talks at scientific symposia organised by Chiesi and research grants from Gilead, outside the submitted work.
Conflict of interest: C. Lange has received personal fees for lecturing at sponsored symposia from Chiesi, Gilead, Abbvie, MSD, Becton Dickinson, Janssen, Lucane, Novartis and Thermofisher, outside the submitted work.
- Received September 15, 2017.
- Accepted December 20, 2017.
- Copyright ©ERS 2018
References










