



Chronic breathlessness: re-thinking the symptom
- Olivia K. Faull,
- Lucy Marlow,
- Sarah L. Finnegan and
- Kyle T.S. Pattinson⇑
- Breathe Oxford Research Group, Nuffield Dept of Clinical Neurosciences, University of Oxford, Oxford, UK
- Kyle T.S. Pattinson, Breathe Oxford Research Group, Nuffield Dept of Clinical Neurosciences, University of Oxford, John Radcliffe Hospital, Oxford, OX3 9DU, UK. E-mail: kyle.pattinson{at}nda.ox.ac.uk
Abstract
Chronic breathlessness, symptom or syndrome: are we asking the right question? http://ow.ly/qJSX30hRpFq
To the Editor:
Is chronic breathlessness a symptom or a syndrome? Although hotly debated [1–5], we would like to suggest an alternative viewpoint. Here, we speculate that the argument over chronic breathlessness being considered as either a symptom or syndrome both holds us within a reductionist framework, and somewhat misses the point.
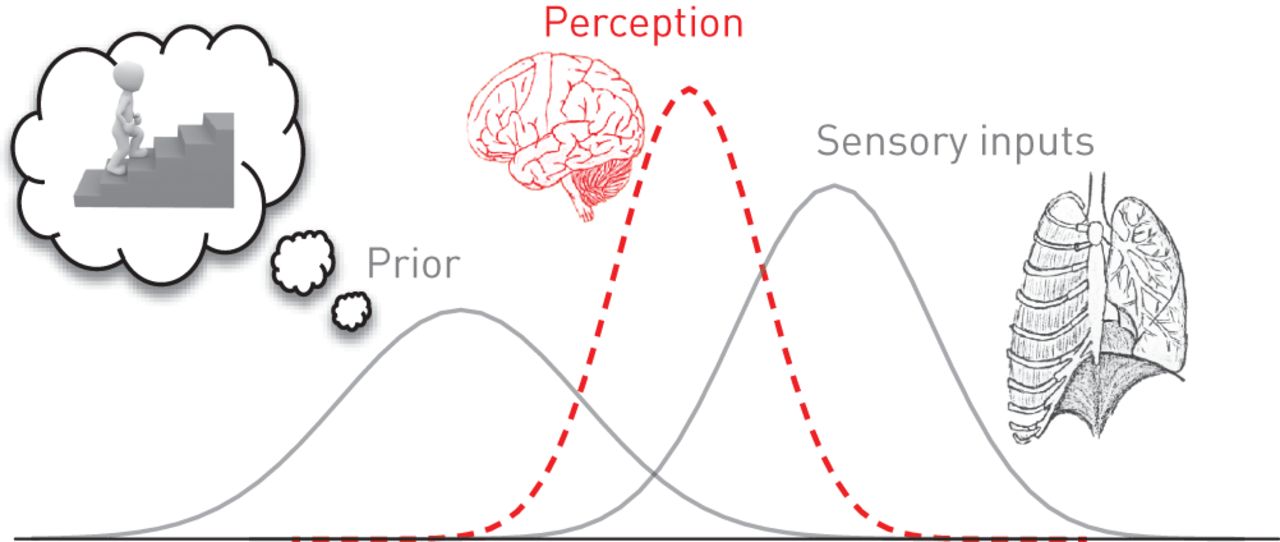
The approach of traditional medicine has been to identify and target the pathophysiology thought to underlie symptoms, and thus treat a disease. However, more modern neuroscientific approaches have taken a significant leap forward within our understanding of perceptual systems. First examined within the conventional, exteroceptive senses (vision, touch, etc.), the “Bayesian brain hypothesis” outlines how perception occurs as a result of a delicate balance between incoming sensory information and the brain's predictions about the world around us, based on learned experiences (priors) (figure 1). This hypothesis has recently been applied with vigour toward a more abstract set of perceptions, which consider the monitoring of our internal sensations (termed interoception [6–8]), such as breathing [9, 10].
{kind=link}
Schematic of the Bayesian brain hypothesis. Both prior expectations and incoming sensory information contribute to the resulting perception, where each is a distribution of possible values. Thus, both the precision and position of priors and sensory inputs can influence perception.
Thus, this framework emboldens us for a more comprehensive appreciation of the important point raised by Calverley [5]; namely, understanding what illness means to the patient and how it affects their lives. Each individual brings their own set of prior expectations, interoceptive abilities and bodily awareness [11, 12] and, thus, breathlessness will be both vastly quantitatively and qualitatively different between individuals. The breadth of these differences cannot hope to be enumerated into a narrow, homogenous set of symptoms that fall within a customary definition of a “syndrome”, but that does not need to be what Johnson et al. [1] were trying to achieve. The point, instead, is to view breathlessness as something that might not directly correspond to airway pathophysiology, and which may need to be treated both in parallel and independently of the lungs.
Furthermore, this theoretical view of breathlessness does not simply stop at lung disease. Whilst descriptive differences are often apparent between individuals who experience breathlessness in health, lung disease and other breathlessness-associated diseases, there is unlikely to be a hard qualitative boundary that exists between these (sometimes transient) health statuses. The wealth of experiences and prior expectations brought to the table by even healthy individuals will evoke a spectrum of breathlessness perceptions, and may even alter an individual's propensity towards symptom severity and debilitation, should they ever become associated with disease. Therefore, attempts to quantify even the intensity of breathlessness as a more purely physiological perception determined by neural respiratory drive, whilst appealing within a traditional reductionist framework, appears to be a significant oversimplification that moves us further from understanding breathlessness within an individual.
So where do we go from here? How do we tackle these seemingly infinite degrees of freedom and dimensions of breathlessness within an individual? Whilst phrenology was popular within the Victorian era, where different parts of the brain were assigned different functions, we must now update our methodology to equip us to test these current theories. Modern neuroimaging techniques allow us to envision cortical activity that may flow from areas such as primary motor/sensory cortices and posterior insula, relevant for primary signal transduction of afferent inputs, but we must tread carefully in labelling this “conscious perception”. Instead, perception (and indeed breathlessness) is likely to be an evolving function embedded within dynamic brain networks, where transduced sensory inputs are continuously compared to the brain's model of the world. Thus, linear increases in activity within one brain area is not likely to produce a corresponding linear change in breathlessness, and we need to equip ourselves with appropriate computational strategies [13, 14] to tackle these more difficult, more multi-dimensional brain network models.
Therefore, the suggestion from Campbell and Howell [15] that “a respiratory physiologist offering a unitary explanation for breathlessness should arouse the same suspicions as a tattooed archbishop offering a free ticket to heaven”, appears to have been a foreseen and apt word of caution to our modern neuroscientific selves. Indeed, to understand breathlessness we need to delve into the brain more deeply, requiring an understanding of the networks that generate perception, and not just correlated activity in single brain areas. In turn, this may lead us to identify important treatable traits relating to breathlessness, complementing periphery-based therapies across a host of diseases and disorders, and hopefully better address the holistic effect of an illness on the life of an individual.
Disclosures
Supplementary Material
K.T.S. Pattinson ERJ-02238-2017_Pattinson
Footnotes
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received October 31, 2017.
- Accepted November 2, 2017.
- Copyright ©ERS 2018