





Figures
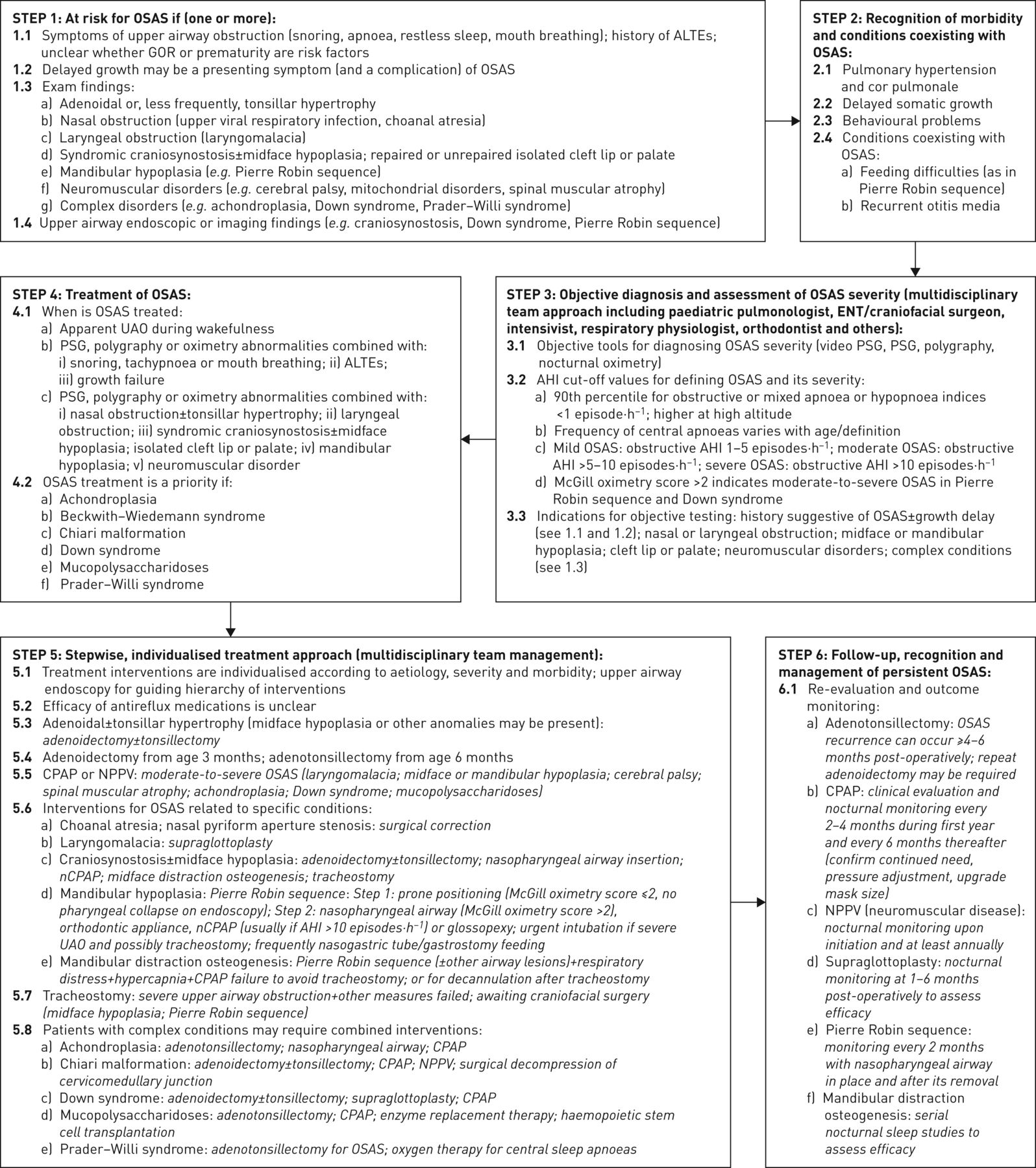
- FIGURE 1
A stepwise approach to the management of obstructive sleep disordered breathing in 1- to 23-month-old children reflecting the Task Force members’ current practice. This scheme is not intended as a recommendation for clinicians. OSAS: obstructive sleep apnoea syndrome; ALTE: apparent life-threatening event; GOR: gastro-oesophageal reflux; ENT: ear, nose and throat; PSG: polysomnography; AHI: apnoea–hypopnoea index; UAO: upper airway obstruction; CPAP: continuous positive airway pressure; NPPV: non-invasive positive pressure ventilation; nCPAP: nasal CPAP.
{kind=link}
Tables
- TABLE 1
Definitions of obstructive sleep disordered breathing (SDB) and its clinical entities
Definition Obstructive SDB A syndrome of upper airway dysfunction during sleep characterised by snoring and/or increased respiratory effort that result from increased upper airway resistance and pharyngeal collapsibility Clinical entities Primary snoring Habitual snoring (>3 nights per week) without apnoeas, hypopnoeas, frequent arousals from sleep or gas exchange abnormalities Upper airway resistance syndrome Snoring, increased work of breathing, frequent arousals, but no recognisable obstructive events or gas exchange abnormalities Obstructive hypoventilation Snoring and abnormally elevated partial pressure of carbon dioxide in the absence of recognisable obstructive events Obstructive sleep apnoea syndrome Recurrent events of partial or complete upper airway obstruction (hypopnoeas, obstructive or mixed apnoeas) with disruption of normal oxygenation, ventilation and sleep pattern Information from [4, 5].
- TABLE 2
Similarities and differences in the diagnosis and management of obstructive sleep disordered breathing (SDB) in younger and older children (1–23 months versus 2–18 years)
Younger children (1– 23 months) Older children (2–18 years) Diagnosis Symptoms reflecting upper airway obstruction are frequently present both during wakefulness and sleep Yes No Adenotonsillar hypertrophy and obesity predominantly cause SDB No Yes Various congenital, syndromic and/or genetic entities predominantly cause SDB Yes No Feeding difficulties and growth failure may coexist with OSAS Yes No Pulmonary hypertension may complicate OSAS, especially in patients with complex conditions Yes Yes Polysomnography is the gold standard for diagnosis of OSAS Yes Yes Endoscopy is especially useful to determine the level of upper airway collapse Yes No Management Adenotonsillectomy is the most commonly used treatment No Yes NPPV is frequently used as first-line treatment due to a high incidence of multilevel, dynamic airway collapse Yes No Orthodontic appliances are effective in cases of OSAS with retrognathia or malocclusion No Yes Patients with complex conditions are prioritised for treatment Yes Yes Follow-up after each treatment intervention may identify persistent OSAS Yes Yes Patients on NPPV undergo nocturnal cardiorespiratory monitoring annually Yes Yes OSAS: obstructive sleep apnoea syndrome; NPPV: non-invasive positive pressure ventilation.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-00985-2017_Supplement











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Unique characteristics of this ERS statement
- Methods
- Results of the literature search
- Topic 1: recognition of the young child at risk for OSAS
- Topic 2: recognition of morbidity and conditions frequently coexisting with OSAS in young children
- Topic 3: objective diagnosis and assessment of OSAS severity
- Topic 4: treatment of OSAS in young children
- Topic 5: stepwise individualised treatment approach for OSAS in young children
- Topic 6: follow-up, recognition and management of persistent OSAS
- Conclusions
- Supplementary material
- Acknowledgements
- Footnotes
- References
- Figures & Data
- Info & Metrics