





Abstract
Teenagers from a previously M. tuberculosis transmission-free settlement were at particular risk during a TB outbreak http://ow.ly/KALqZ
To the Editor:
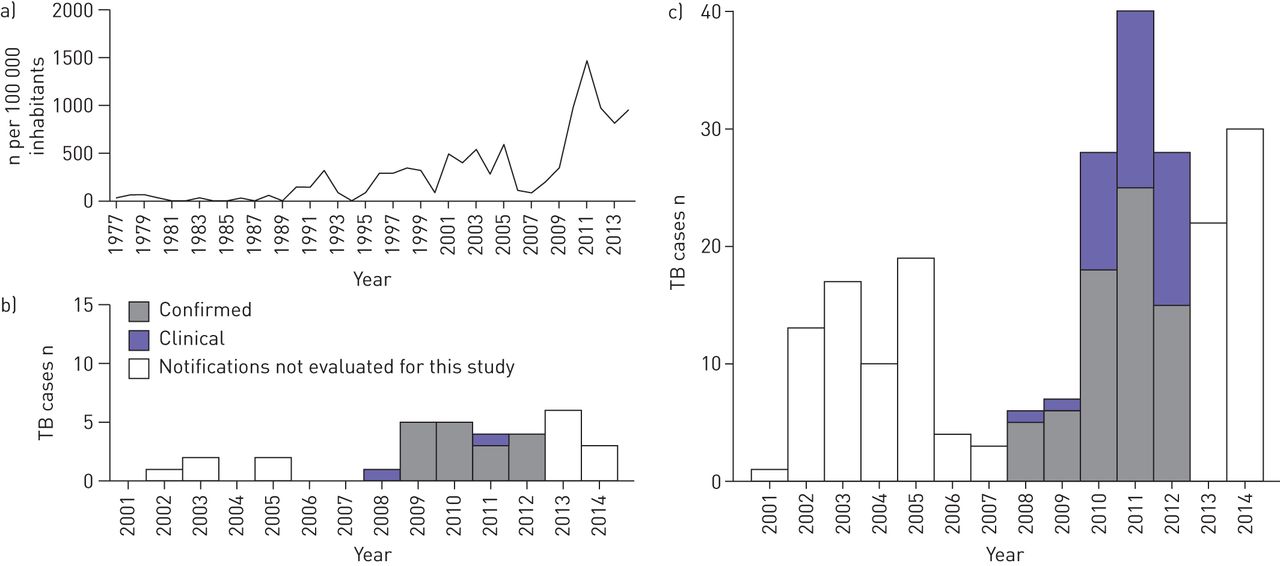
In 2009, an unusually high number of tuberculosis (TB) cases were reported from a settlement (Settlement X) in East Greenland. 4 years earlier, screening among schoolchildren had documented all children in this settlement to be free of Mycobacterium tuberculosis infection (MTI), whereas similar screenings had shown an MTI prevalence of 8% among schoolchildren in the rest of East Greenland [1]. The average TB incidence rate in East Greenland 5 years prior to the outbreak was ∼300 per 100 000 populations (fig. 1) [2, 3].
The documentation of areas with differences in M. tuberculosis transmission prior to a TB outbreak provided a special opportunity to study the risk of TB in these settings that have an otherwise comparable population. The objective of the study was to estimate the risk of TB and MTI during an outbreak, and to evaluate whether individuals from a previously M. tuberculosis transmission-free environment exhibited particular risk.
We conducted a cohort study including all inhabitants living in East Greenland on January 1, 2008 (n=3541). Participants were followed until TB notification, death, emigration or December 31, 2012. A personal Civil Registration System (CRS) identifier given to Greenlandic citizens at birth combined data across public registries. The cohort was stratified by residency (Settlement X or the rest of East Greenland) at study entry.
Notification of TB to the National Board of Health is mandatory and the Greenlandic TB case definition follows that of the World Health Organization (WHO) [4, 5]. A positive interferon-γ release assay (IGRA) (QuantiFERON-TB Gold; Cellestis, Venlo, the Netherlands) defined an MTI case. IGRA results among the cohort participants were obtained from routine diagnostics, contact tracing or previously conducted population screening and projects [1, 6]. Information on covariates was obtained from the CRS, TB notifications and medical records. A Greenlandic birthplace of both parents defined Greenlandic heritage.
Since 1955, all newborns have been offered bacille Calmette–Guérin (BCG) vaccination with national coverage rates of 90–99%. However, the BCG vaccination programme was temporarily discontinued between 1991 and 1996, and children born in these years were considered unvaccinated [2, 6, 7].
Crude TB incidence rates (IR) were estimated as TB cases per 100 000 person-years. Incidence rate ratios were estimated with Cox proportional hazard models with age as the underlying time axis and baseline hazard rate stratified by sex [8].
Age-specific MTI prevalences as of January 1, 2013, were estimated from all IGRA results since 2005 using an expectation-maximisation algorithm as a function of calendar time [9]. Time of birth or last negative test and time of first positive test defined the limits of the interval in which individuals were considered infected. Individuals with only negative results were considered right-censored at time of the last test. An MTI population prevalence was estimated by averaging the age-specific MTI prevalences with the percentages of the population in each age group. SAS statistical software, version 9.4 (SAS Institute, Cary, NC, USA) was used for analyses.
The Committee for Scientific Research in Greenland (Copenhagen, Denmark) approved the study (approval no. 2012-071304). All referred studies were individually approved by the Committee and fulfilled the Helsinki II declaration.
Table 1 presents demographic data, estimated MTI prevalence and TB IR for East Greenland. During the study period, 127 cohort participants were diagnosed with TB (fig. 1).
{kind=link}
Demographic characteristics of the study cohort, Mycobacterium tuberculosis infection prevalence as of January 1, 2013, and tuberculosis (TB) incidence rates (IRs) per 100 000 person-years, presented by residency
MTI prevalence was estimated on the basis of 4060 IGRAs (1157 positive) from 2238 cohort participants (844 positive individuals). For Settlement X, estimated MTI prevalence increased overall to 60.9%, and among teenagers born between 1991 and 1996, to 79.1%. For the rest of East Greenland, the numbers were 37.5% and 41.9%, respectively. 62 cohort participants from Settlement X participated in the 2005 school screening where all participants were MTI negative; 44 (75%) of these had become positive before the end of the study period. For the rest of East Greenland, the MTI prevalence among schoolchildren who participated in the 2005 screening changed from 8% to 32%.
Participants were followed for 17 028 person-years. The TB IR increased to 2695 per 100 000 person-years in Settlement X and to 1604 per 100 000 person-years for the rest of East Greenland. The TB IR was 2.48 (95% CI 1.6–3.85) times higher in Settlement X as compared with the rest of East Greenland. Overall, teenagers had the highest TB IR in both locations, but with a pronounced difference by place of residency: 4.08 (95% CI 2.28–7.31) times higher in Settlement X than in the rest of East Greenland.
TB IR more than doubled during the outbreak in East Greenland from 2009 to 2012. The risk of TB and MTI was especially pronounced in individuals from the previously M. tuberculosis transmission-free Settlement X. For these individuals, the TB IR increased more than five-fold. The highest TB IR was observed among teenagers, and teenagers from Settlement X experienced the highest rate. Likewise, the estimated MTI prevalence was high, especially among BCG-unvaccinated individuals born in 1991–1996, among whom 79% from Settlement X and 42% from the rest of East Greenland were estimated to have MTI.
Compared with TB IRs from other high TB burden countries [10], the TB IR in East Greenland was high and approaches rates observed in Greenland before the 1950s (2000 per 100 000) [11] despite a low HIV prevalence and almost no TB drug resistance [7, 12]. While crowding, poverty and smoking are highly prevalent in East Greenland, living standards are improving as in the rest of Greenland [13, 14]. The discontinuation of neonatal BCG vaccinations from 1991 to 1996 accounts for some of the increased rates in teenagers as compared with other age groups [6]. However, the difference in risk related to residency is not explained by a lack of vaccination and should be further studied. Teenagers from small settlements have to move to larger towns to finish secondary school and we speculate whether this physical relocation could increase the TB risk during an outbreak because of a possibly increased infection pressure in boarding homes combined with the stress of being relocated at a young age.
No schoolchildren in Settlement X had MTI in 2005, indicating that they had been raised in a low TB endemic period with presumably no M. tuberculosis transmission [1]. Of these previously IGRA-negative schoolchildren, 75% were IGRA-positive after 2010. Since the bulk of MTI occurs among the young, a further increase in IR can be expected in years to come.
Major strengths of this study are the unique CRS linkage of registers, and the availability of longitudinal data on both TB disease and MTI. A possible weakness in estimating MTI prevalence is the assumption that tests have been performed regardless of expected results, as in population-wide screenings. Including IGRA results from M. tuberculosis-exposed individuals from contact tracings could lead to overestimation. However, most individuals had more than one IGRA performed, which strengthens the estimates of interval censuring.
In conclusion, individuals from a previously M. tuberculosis transmission-free settlement carried an extra two-fold risk of MTI and TB disease during the outbreak. Teenagers had the highest TB risk, with unvaccinated teenagers from the previously M. tuberculosis transmission-free settlement being especially vulnerable. Greenland has a national TB programme evaluated by WHO, and treatment and access to care are free of charge [7], yet Greenland remains a high TB incidence country a long way from achieving TB elimination [15]. The study emphasises the need to rapidly confine any TB outbreak, especially in previously transmission-free environments, and underlines the importance of identifying groups at risk in order to aid future TB interventions.
Acknowledgements
The authors thank the East Greenlandic population for participation in the study, and H.C.F. Sørensen (Tasiilaq, Greenland), and former TB nurses J. Sommer and M. Weismann (Tasiilaq, Greenland) for identifying and treating TB patients, and collecting and providing data. The authors also thank the healthcare personnel in East Greenland, the Chief Medical Officer, Queen Ingrid's Health Center (Nuuk, Greenland), Queen Ingrid's Hospital and the Central Laboratory (Nuuk, Greenland) for support and access to data.
Footnotes
Support statement: The Commission for Scientific Research in Greenland, Forskningspuljen and Sundhedspuljen (Greenland Self-Government) funded the study.
Conflict of interest: None declared.
- Received December 15, 2014.
- Accepted February 21, 2015.
- Copyright ©ERS 2015










