





Figures
- Figure 1–
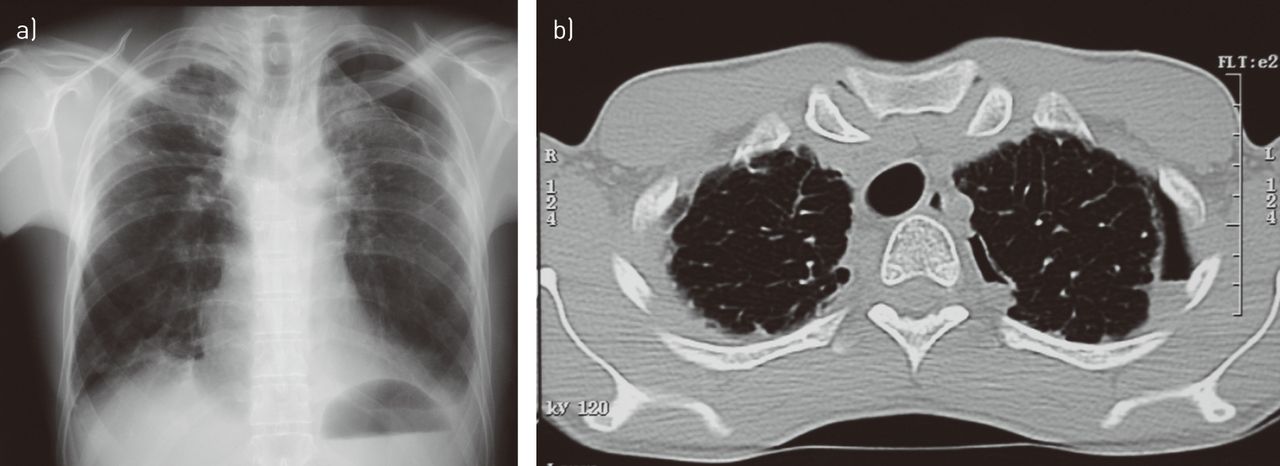
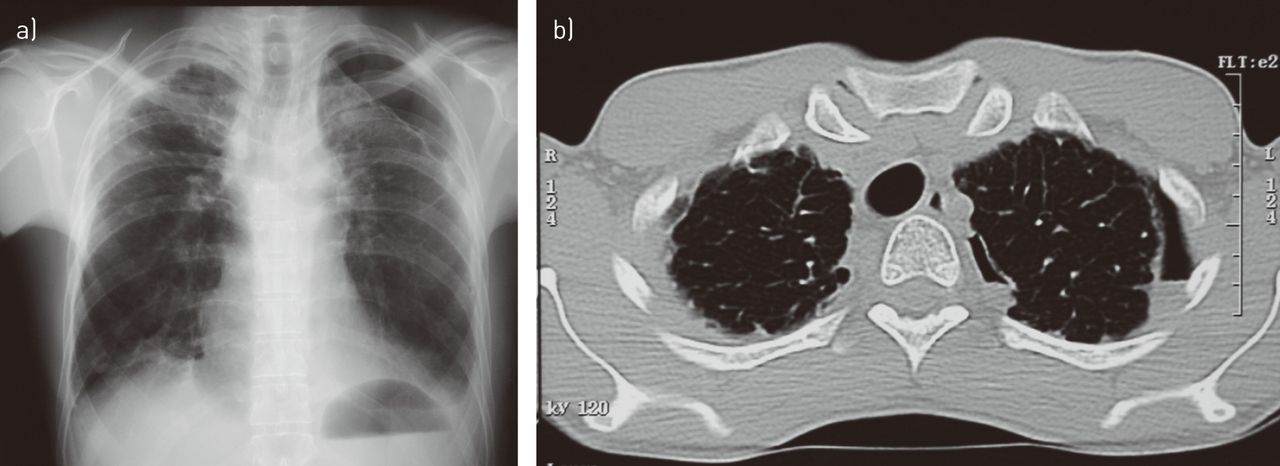
a) Frontal chest radiograph in a patient following chemotherapy for acute lymphoblastic leukaemia showing a typical appearance of pleuropulmonary fibroelastosis (corresponding to case 2 in [1]). Note the markedly thickened pleural dome on the right and partial spontaneous pneumothorax on the left. b) Computed tomography scan of the same patient taken several months later. A chest tube had been inserted and removed in the interim. A smaller, persistent pneumothorax is visible.
- Figure 2–
Advanced cases may show markedly restrictive physiology and reduced anterio-posterior diameter of the thorax; a trait known as platythorax.
- Figure 3–
Gross pathology of the lung showing grey elastotic fibrosis in the subpleural regions and around the bronchovascular bundles.
- Figure 4–
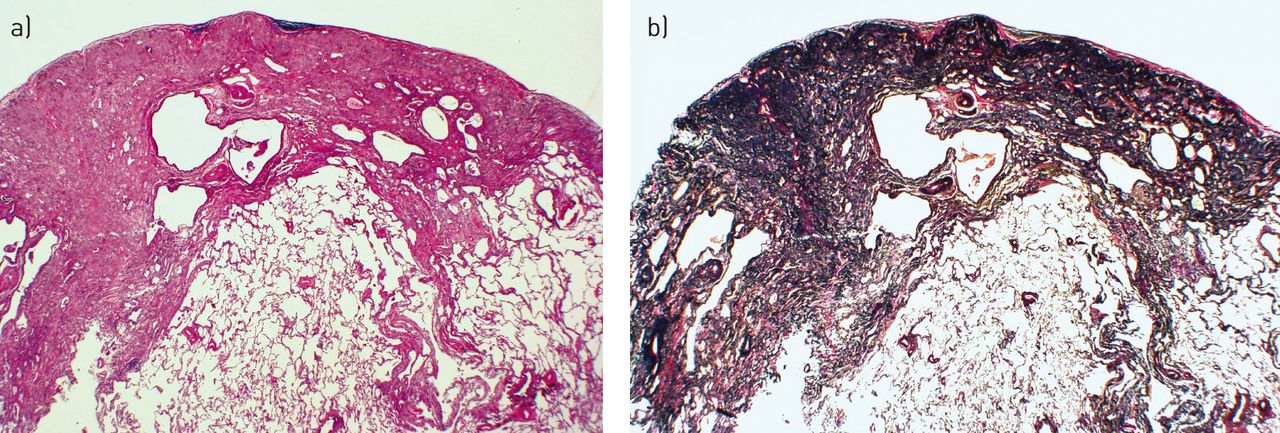
Histology staining showing a sharply demarcated zone of subpleural fibrosis with abundant elastic tissue on elastic tissue stain. a) Haematoxylin and Eosin stain and b) Verhoeff van Gieson elastic stain. Scanning power microscopy ∼40×.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1– Diagnostic features of pleuropulmonary fibrosis (PPFE)
Symptoms (not all of which may be present) Dyspnoea Dry cough Weight loss Dull chest pain Anteroposterior flattening of the chest wall (platythorax) mostly present in advanced cases ( fig. 3), may denote advanced disease Smoking status 85% never-smokers Significant history Lung transplant recipient: ∼50% Bone marrow transplant: 6% Prior exposure to chemotherapy or alkylating agents: 10% Family history of pulmonary fibrosis: 9% Idiopathic in an estimated 10–30% Imaging: chest radiograph and HRCT Bilateral apical (upper lobe + pleural dome) thickening invading the lung Generalised loss of volume The lower pleural-pulmonary zones are less involved or spared Interstitial markings may be increased Hila progressively retracted upwards Uni- or bilateral spontaneous partial pneumothoraces are common Chest ultrasound No data in humans at present Noninvasive imaging methods have been described in a donkey with PPFE [17] Pulmonary physiology Restrictive to markedly restrictive Obstruction present in some patients Over time, progressive hypoxaemia and hypercarbia may develop Bronchoalveolar lavage No consistent shifts in macrophages, lymphocytes, neutrophils or eosinophils PET scan No consistent data at present Pathology findings Upper zone collagenous fibrosis of the visceral pleura with haphazardly arranged elastic fibres Biopsy is NOT a prerequisite for PPFE diagnosis Subpleural intra-alveolar fibrosis with a sharp boundary with the underlying lung Alveolar septal elastosis Sparing of the parenchyma away from area of pleural thickening Mild, patchy lymphoplasmocytic infiltrates Fibroblastic foci are rare or absent HRCT: high-resolution computed tomography; PET: positron emission tomography. For more details see [2].










