





Abstract
There is a growing need to identify appropriate standardised treatment strategies that will adequately treat various forms of drug-resistant tuberculosis (TB) and prevent multidrug-resistant (MDR)-TB.
A Markov model estimated treatment-related acquired MDR-TB, mortality, disability-adjusted life years and costs in settings with different prevalence of isoniazid monoresistant TB and MDR-TB. We compared four treatment strategies: 1) the standard World Health Organization recommended treatment strategy; 2) adding ethambutol throughout the 6-month treatment of new cases; 3) using a strengthened standardised retreatment regimen; and 4) using standardised MDR treatment for failures of initial treatment. Treatment-related outcomes were derived from the published literature, and costs from direct surveys.
A strengthened retreatment regimen, which could achieve lower failure, relapse and acquired MDR rates in isoniazid monoresistant cases, was predicted to be the most cost-effective strategy in all modelled settings. Empirical MDR treatment of failures of initial treatment was the most costly strategy but resulted in the fewest deaths. Adding ethambutol throughout initial treatment would be most effective in preventing acquired MDR, but would lead to excess cases of blindness.
A high priority should be given to improving the standardised retreatment regimen, as this is predicted to produce greater benefits than other recently recommended strategies.
Abstract
Priority should be given to improving the standardised TB retreatment regimen http://ow.ly/r54us
Introduction
The World Health Organization (WHO) estimated that in 2011 there were 8.7 million new tuberculosis (TB) cases and 1.4 million TB deaths [1]. As a consequence of inadequate TB treatment and management, drug-resistant TB has emerged in all parts of the world and now accounts for ∼17% of all new cases [2]. The most common form of drug-resistant TB is isoniazid (INH) resistance, which is seen in 10% of new cases [2]. INH resistance is of concern as INH is one of the two most effective and potent first-line anti-TB drugs, and approximately one-third of new cases with INH resistance, or 3% of all new cases, has multidrug-resistant (MDR)-TB, which is a strain resistant to both INH and rifampicin (RMP) [2]. Patients with MDR-TB have substantially worse treatment outcomes [3, 4], despite a course of treatment that is much longer [5], and is more toxic and expensive [1], than for drug-sensitive TB. The proportions of MDR-TB have been increasing in many parts of the world; the highest proportions recorded in the history of the WHO Global Project on Anti-tuberculosis Drug Resistance Surveillance reached 35.3% among new and 76.5% of previously treated TB cases in 2012 in Minsk, Belarus [6].
Globally, <4% of all new cases of TB are estimated to receive drug susceptibility testing [1]. Thus, the vast majority of drug-resistant TB patients are unrecognised and do not receive adequate treatment [2]. In order to prevent MDR-TB where proper diagnostic testing is unavailable, the WHO recommends empirically adding ethambutol (EMB) throughout the initial treatment of new cases in settings with high levels of INH resistance [7]. However, the ability of EMB to protect against MDR-TB is uncertain [8, 9], and should be weighed against the risk of ocular toxicity [10–14]. The WHO also recommends using an 8-month regimen for previously treated patients who relapsed or defaulted [7]. This standardised retreatment regimen is comprised entirely of first-line drugs, was designed for populations with low levels of INH resistance and has never been tested in randomised clinical trials [4]. Published reports point towards unacceptably high rates of treatment failure, relapse and acquired drug resistance with this regimen in the presence of (non-MDR) INH resistance [3, 4]. Given that ∼28% of all retreatment TB cases are resistant to INH globally [2], this regimen will probably be frequently unsuccessful [3]. A third related WHO recommendation is to use an empirical MDR regimen for patients who have failed initial treatment [15].
The effectiveness of these three WHO treatment strategies is unclear in the context of emerging drug-resistant TB. In this study, we compared the treatment outcomes and costs of different strategies in four settings with different prevalence of INH monoresistance and/or MDR. The four strategies compared were: 1) the current WHO standard initial and retreatment guidelines; 2) adding EMB throughout initial treatment of new cases; 3) using a hypothetical retreatment regimen strengthened with second-line TB drugs; and 4) treating all failures of initial treatment with an empirical MDR regimen.
Methods
Overview
We estimated the treatment outcomes and costs of four different treatment strategies over a 10-year analytical horizon, using a Markov decision analysis model. We adhered to published recommendations for conducting and reporting a cost-effectiveness analysis [16, 17]. We assumed a societal perspective to evaluate costs and discounted both costs and health effects at a 3% annual rate. Our model assumed that drug susceptibility testing was not available and did not influence the treatment given, thus all treatment regimens modelled were standardised. There is insufficient published literature for estimating input parameters specific to HIV-TB co-infected patients; thus, we assumed that patients with HIV co-infection would have similar treatment outcomes [18].
Decision analytic model
We used TreeAge Pro 2008 Suite (release 1.0; TreeAge Software, Inc., Williamstown, MA, USA) to construct the Markov model. The model described the clinical progression of TB disease (fig. 1). A 10-year analytical horizon was used for comparability with previously published cost-effectiveness studies examining TB treatment strategies [19, 20].

Schematic representation of the decision analytic model. The ovals represent the seven different Markov health states. The solid square on the left represents the initial decision regarding which treatment strategy to apply. The solid circles are probability nodes, meaning a pre-defined probability at that node determined the outcome thereafter. These probability nodes make up the probability tree that patients go through to determine their next Markov state after every cycle spent in an “under treatment” Markov state. Throughout the 10-year time horizon, patients transitioned between the Markov states based on transition probabilities. The Markov state “dead” is an absorbing state, which means once patients entered the dead state, they could not transition to other states. Patients entered the “alive with untreated [tuberculosis] TB” state only if they failed, defaulted or relapsed after receiving the standardised multidrug-resistant (MDR) regimen. If a patient entered the “cured” Markov state, they could relapse within the next 1-year cycle. EMB: ethambutol; Str retreat: strengthened retreatment; INH: isoniazid.
The model simulated the treatment outcomes and costs accrued over 10 years for four hypothetical cohorts of 100 000 smear-positive, treatment-naïve TB patients. Each cohort went through the Markov model under four different treatment strategies (described later). When a cohort entered the model, its patient population was distributed across three initial health states, known as Markov states, which described patients with different primary drug resistance profiles (drug-susceptible TB, INH monoresistant TB and MDR-TB) undergoing initial treatment for TB. Only two forms of drug-resistant TB were modelled because there are insufficient published data regarding treatment outcomes of other forms of drug resistance. Patients with any resistance to RMP were considered to be in the same health state as MDR-TB patients because RMP resistance is considered a surrogate marker for MDR, and has significantly worse outcomes than other forms of drug resistance [21–26].
Each cohort represented a different setting with varying prevalence of primary INH monoresistance and MDR-TB in treatment-naïve patients, as follows: 1) low prevalence of both forms of drug resistance (5% INH monoresistant and 1% MDR-TB); 2) high prevalence of INH monoresistance (15%) and low prevalence of MDR-TB (1%); 3) low prevalence of INH monoresistance (5%) and high prevalence of MDR-TB (10%); and 4) high prevalence of both forms of drug resistance (15% INH monoresistant and 10% MDR-TB).
The cycle length of the model was 1 year, which was chosen in order to accommodate the following different treatment lengths: 6 months for initial treatment regimens; 8 months for retreatment regimens; and 24 months for the MDR regimen, which took two cycles. After the first year in the model, patients all moved through a probability tree that determined the Markov state they would be in during the following year. Depending on transition probabilities, patients could fail, default or successfully complete treatment and be cured; become blind due to the ocular toxicity of ethambutol; or die from TB or non-TB causes. Those who failed or defaulted treatment could undergo treatment the following year; however, their underlying drug resistance could have changed and the new regimen they received depended on the treatment strategy being modelled. Those who successfully completed treatment would be in the “cured” state but could relapse and return to treatment; for simplicity, we assumed that all relapses would occur only in the year immediately following treatment completion. Estimates of transition probabilities and treatment outcomes were derived from published literature whenever possible and expert clinical judgement when not (table 1).
After each yearly cycle, patients either transitioned to a different Markov state or remained in the same state. How a patient progressed through the model depended on a patient’s clinical history and underlying drug resistance profile.
Probability of EMB-induced blindness
If a patient became blind at any point during treatment, their treatment was discontinued in our model. This assumption was based on the understanding that blindness is detrimental to the livelihood of patients in resource-limited countries and, critically, curtails their ability to remain in treatment. The probability of becoming blind due to EMB was estimated at 0.23% (95% CI 0–0.61%) for a 6-month EMB treatment, based on results of a systematic review and meta-analysis [14].
Model outcomes
Each health state had corresponding health outcomes (table 1) and costs (online supplementary table S1). At the end of each year, the costs and health outcomes were accrued for the patients. Patients who completed treatment accrued the total cost of treatment. There were no costs assigned to the states “dead”, “blind”, “cured” and “alive with untreated TB”.
Our model results were expressed in terms of costs, INH monoresistant cases prevented, MDR-TB cases prevented, excess blindness, TB-related deaths averted and disability-adjusted life years (DALYs) gained. DALYs are an effectiveness measure introduced by the WHO to combine mortality and morbidity associated with diseases and injuries into one value. The DALY is calculated using disability weights estimated by the WHO, and for this study the weights used were 1 for cured TB (assumed perfect health), 0.729 for active TB (treated or untreated), 0.4 for blind and 0 for dead [36]. For example, if during the 10 years in the model, a patient lived with active TB for 2 years and then was cured and lived for another 8 years, then adjusting for disability, they would have lived for 2×0.729 (for active TB)+8×1 (for cured state)=9.46 DALYs. During each 1-year cycle, if a patient died, defaulted, relapsed or became blind, we assumed the transition between the two corresponding Markov states (e.g. from active TB undergoing treatment to blind) occurred halfway during the year.
TB treatment strategies
The four unique treatment strategies and different treatment regimens examined in the model are summarised as follows.
Reference treatment strategy (status quo): standard
This consisted of initial treatment of new cases with the WHO-recommended 6-months standardised initial regimen (known as 2HRZE/4H3R3) consisting of 2 months of INH, RMP, pyrazinamide (PZA) and EMB taken daily (initial phase), followed by 4 months of INH and RMP taken three times per week (continuation phase). Patients who failed, relapsed after cure or defaulted received the WHO-recommended standardised retreatment regimen with first-line drugs only (known as 2HRZES/1HRZE/5H3R3E3): streptomycin is given daily in the first 2 months; INH, RMP, PZA and EMB are taken daily for the first 3 months; and then INH, RMP and EMB are taken three times per week in the last 5 months.
Ethambutol added to initial treatment: EMB initial
All new patients received the WHO-recommended 6-month standardised initial regimen in settings with a high prevalence of INH resistance (2HRZE/4H3R3E3), consisting of 2 months of INH, RMP, PZA and EMB taken daily (initial phase), followed by 4 months of INH, RMP and EMB taken three times per week (continuation phase). Patients who failed, relapsed after cure or defaulted received the standardised retreatment regimen as in the standard strategy. Compared with the standard strategy, the addition of EMB throughout the initial regimen was assumed to reduce by 50% the probability of acquired INH monoresistance and acquired MDR-TB after initial treatment, and to increase the probability of EMB-induced blindness from 0% to 0.23%, but did not change any other probabilities.
Strengthened retreatment: Str retreat
New patients received the same initial treatment as in the standard strategy, but those who failed or relapsed after cure or default received a retreatment regimen that included second-line drugs (2 months of daily levofloxacin, rifampicin, pyrazinamide, ethambutol and streptomycin, followed by 1 month of daily levofloxacin, rifampicin, pyrazinamide and ethambutol, then by 6 months of thrice-weekly levofloxacin, rifampicin, and ethambutol; 2LfxRZES/1LfxRZE/5Lfx3R3E3): for costing purposes (but without data confirming the efficacy of this regimen), we assumed the regimen would be an 8-month standardised regimen in which INH was replaced with levofloxacin.
Compared with the standard strategy the strengthened retreatment strategy was assumed to reduce by 50% the probability of failure, or relapse and associated acquired MDR-TB in retreated patients with initial INH resistance, but did not change any other probabilities.
Standardised MDR treatment for failures of initial treatment: MDR failures
New patients received the same initial treatment as in the standard strategy. Patients who defaulted or relapsed after cure from initial treatment received the same retreatment regimen as described for the standard strategy. But those who failed initial treatment received a 24-month standardised MDR regimen. All patients were hospitalised for only 1 month at the start of MDR treatment, given published studies of the effectiveness of community-based treatment [37–39]. Amikacin (Am) is injected daily for the first 6 months. PZA, EMB, levofloxacin and ethionamide are taken daily for 24 months (6AmZELfxEth/18ZELfxEth) [5, 27, 29].
Compared with the standard strategy, the MDR failures strategy (MDR failures) was assumed to improve treatment outcomes in failure cases who had MDR in order to achieve cure rates equivalent to published estimates using this regimen [3]. All other probabilities remained unchanged.
For the first three strategies, patients who failed, relapsed or defaulted after retreatment received the WHO recommended standardised MDR regimen (6AmZELfxEth/18ZELfxEth) [5]. For all four strategies, patients who failed, relapsed or defaulted after receiving one course of the MDR regimen were assumed to receive no further treatment, and to enter a state of untreated TB from which they could continue to live, die or be spontaneously cured. The annual spontaneous cure rate was assumed at 25% [28, 33].
Treatment outcomes and probabilities
Estimates of transition probabilities and treatment outcomes, and published sources for these estimates are summarised in table 1.
There is no published information regarding the impact of adding EMB throughout initial treatment (EMB initial) on outcomes, and limited evidence on the treatment outcomes of a strengthened retreatment approach (Str retreat) where INH is replaced with a later generation fluoroquinolone regimens [40]. Hence, assumptions were made regarding their efficacy relative to the WHO standardised initial and retreatment regimens.
Costs
Costs were estimated from the societal perspective, and included health systems costs, patients' and families' out-of-pocket expenditure, and lost wages (online supplementary table S1). All costs were expressed in 2010 international US dollars, which were adjusted using 2007 power purchasing parity estimates for Ecuador [41], and inflated to 2010 currency using the average consumer price index in the US for 2007 and 2010 [42]. We used cost estimates from Ecuador because direct and indirect patient costs had been estimated there recently [43]. Indirect patient costs were based on patient and family time lost during TB diagnosis and treatment, which was converted into monetary costs using the hourly wage based on the power purchasing parity-adjusted average per capita gross national income [44].
Ecuador has one of the highest levels of MDR-TB in Latin America [2], which makes it an appropriate setting for estimating MDR-TB treatment costs. The country achieved national implementation of directly observed therapy, short course (DOTS) in 2006, and provides TB treatment and diagnosis free of charge for patients [45, 46]. Thus, estimated treatment costs should be comparable with other countries that have national coverage for DOTS.
Estimating health system costs
An interviewer-administered health facility cost survey was used to collect health system data in Ecuador. The interviews were conducted in 19 urban health facilities that treated TB patients in two provinces (Guayas and Tungurahua) between September and October 2009: 16 Ministry of Health clinics, two Ministry of Health hospitals and one nongovernment hospital (Erika Leung, McGill University, Montreal, Canada; personal communication). Salary levels of Ministry of Health employees were retrieved from the Ministerio de Inclusión Económica y Social [47]. We assumed that the personnel costs made up 80% of the total facility budget [48, 49]. The average health system cost per outpatient visit was the quotient of dividing the estimated total facility budget of each Ministry of Health clinic by the reported number of annual outpatient visits.
We assumed that the total inpatient budget of a hospital was the difference between the total health facility budget and the total outpatient budget. The per diem cost was the total inpatient budget divided by annual number of bed-days. Only data from one Ministry of Health hospital, Hospital Alfredo J. Valenzuela, was included because it was a respiratory/pulmonary-specific hospital and would be more applicable for estimating TB-related per diem costs. The cost of each directly observed therapy visit was estimated to be a third of the cost of an outpatient visit. This assumption was based on previously published surveys of health system costs [50, 51].
Cost-effectiveness analyses
We calculated three incremental cost-effectiveness ratios (ICERs): cost per MDR case averted, cost per death averted and cost per DALY gained.
Sensitivity analyses
We performed one-way sensitivity analyses to account for uncertainties in key model assumptions: prevalence of INH and MDR monoresistance; the probability of EMB-induced blindness; the efficacy of adding EMB throughout initial treatment and of strengthening the retreatment regimen with a second-line drug; the duration of hospitalisation during MDR treatment; and varying the discount rates used. The ranges chosen for each analysis were based on the published literature, WHO reports or expert opinion. We also performed probabilistic sensitivity analysis to incorporate statistical or sampling variability in input parameter estimates by performing 10 000 Monte Carlo simulation trials per analysis. We used 95% confidence intervals or ranges to estimate corresponding probability distributions with the method of moments approach [52]. γ distributions were assigned to cost parameters and β distributions to probability estimates [52]. Using the results from the probabilistic sensitivity analyses, cost-effectiveness acceptability curves were constructed to compare the different treatment strategies in the four hypothetical settings. These curves plot the probability that a given treatment strategy is cost-effective compared to the standard WHO strategy given a maximum acceptable ICER threshold. This threshold is also known as the willingness-to-pay threshold, indicating the maximum amount the group of interest (patient, government or society) is willing to pay per unit of benefit gained.
Results
Treatment-related outcomes
With the standard strategy, we predicted between 407 and 781 new MDR cases from acquired drug resistance, between 1.3% and 7.3% failures, and between 5.2% and 9.8% deaths, depending upon whether the prevalence of drug resistance was low or high (table 2). All three alternative treatment strategies resulted in fewer cases of MDR-TB and fewer TB deaths than standard (Tables 2 and 3).
Overall, EMB initial was predicted to avert the most cases of MDR-TB compared with standard. This strategy was predicted to prevent between 337 and 347 MDR cases per 100 000 patients when the prevalence of INH monoresistant TB was 15%, depending on whether the prevalence of MDR-TB was high (10%) or low (1%), respectively. When the prevalence of INH-resistant TB was 5%, this strategy was predicted to avert 177 and 186 MDR cases when the prevalence of MDR-TB was 10% and 1%, respectively. The other strategies were predicted to avert fewer MDR cases: between 30 and 61 MDR-TB cases for the strengthened retreatment strategy, and only five or six cases per 100 000 patients for the MDR failure strategy.
MDR failure strategy averted the most TB-related deaths compared with the standard strategy in all settings (between 75 to 664 deaths averted per 100 000 patients) except when the prevalence of INH monoresistant was 15% and the prevalence of MDR-TB was 1%, in which case the EMB initial strategy averted the most deaths at 128 per 100 000 patients.
The EMB initial strategy consistently resulted in a loss of DALYs compared with the standard strategy. Conversely, strengthened retreatment and MDR failure resulted in gains in DALYs compared with standard in all four settings. MDR failures resulted in the largest gains in DALYs in all settings, from 613 to 5454 total DALYs gained per 100 000 patients compared with standard regimen, and the gains were larger when the prevalence of MDR-TB was high at 10% and largest when both prevalence of MDR-TB and mono-INH resistant TB were high.
Treatment-related costs
Standardised MDR treatment of all failures of initial treatment (MDR failures) was the most costly treatment strategy in all four settings. The EMB initial and strengthened retreatment strategies were equal in cost or less costly than standard in all four settings (Tables 2 and 3). EMB initial was the least costly of all four strategies in all settings.
Incremental cost-effectiveness ratios
The strengthened retreatment strategy dominated the standard strategy, the more effective and less costly strategy, in terms of cost per MDR case averted, cost per TB death averted and cost per DALY gained compared with the standard treatment strategy in all four settings (table 2 and 3). EMB initial dominated standard as well as strengthened retreatment strategies, resulting in more cost savings and fewer MDR cases and TB deaths than both strategies. However, these advantages were offset by the predicted development of blindness in some patients, so that this strategy resulted in fewer total DALYs than the standard strategy (i.e. was less effective) in all four settings.
The MDR failures strategy cost between $2857 and $2860 per DALY gained compared with standard when the prevalence of MDR-TB was high at 10%. The cost per DALY gained increased when the prevalence of MDR-TB was low at 1%, between $4867 and $5745 per DALY gained compared with standard. A similar trend was observed for cost per TB death averted, and the opposite for cost per MDR case averted.
Sensitivity analyses
Prevalence of drug resistance was an important determinant of cost-effectiveness as shown in table 4. EMB initial was always dominant (less costly and more effective) compared with the standard strategy in terms of cost per MDR cases averted and cost per death averted regardless of the drug resistance prevalence. However, it was less effective in terms of cost per DALY gained compared to standard under most conditions, but dominated standard when the prevalence of INH monoresistant TB was >21%. Conversely, strengthened retreatment was always dominant over standard. The MDR failure strategy never dominated standard; however, it was always more effective. It became more cost-effective as the prevalence of MDR-TB increased, and bacame as low as $2665 per DALY gained when the prevalence of INH monoresistant TB was 5% and that of MDR-TB was 20%.
Strengthened retreatment was consistently dominant over standard treatment when other key assumptions were changed, except that it became more costly than standard when the efficacy of the strengthened retreatment regimen was less than approximately two times that of the standard retreatment, and when the hospitalisation period for MDR treatment was <1 month long, in settings with 5% INH monoresistant TB (online supplementary table S2). MDR failure was also more cost-effective when the duration of hospitalisation during MDR treatment was shorter, being as low as $664 per DALY gained when there was no hospitalisation, and was less cost-effective when it was long, being as high as $25 044 per DALY gained when there were 6 months of hospitalisation. Findings remained similar when we used the WHO-recommended discount rates of 6% for costs and 0% for health outcomes.
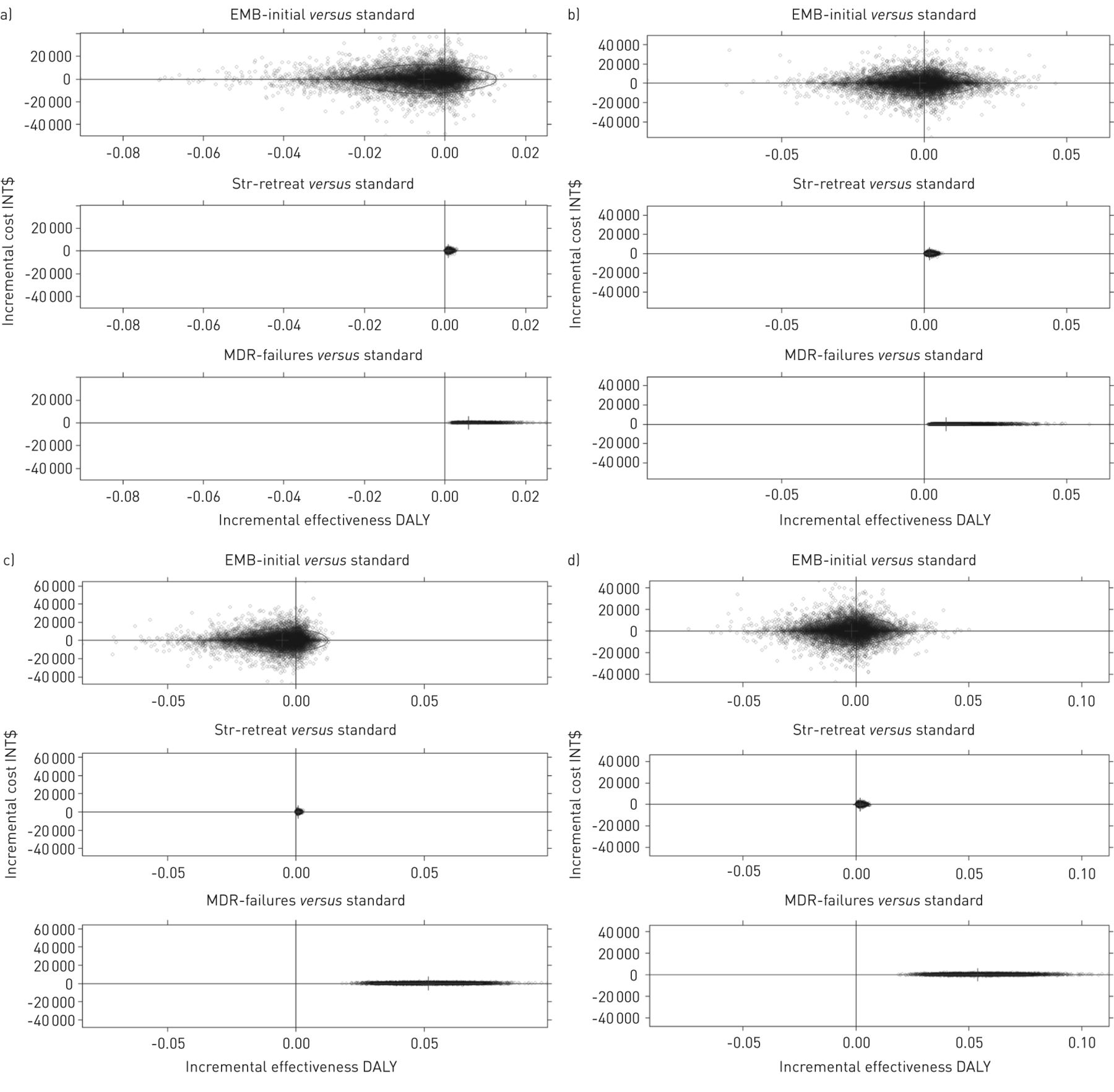
Results of probabilistic sensitivity analyses are shown in figure 2. The incremental costs of the EMB initial strategy varied widely, as did DALYs gained or lost, although in the majority of the simulations this strategy led to fewer DALYs than the standard strategy. Conversely, the strengthen retreatment and MDR failure strategies consistently led to more DALYs, with a much narrower range of incremental costs, centred around no difference, compared with the standard strategy.

{kind=link}
{kind=link}
Probability sensitivity analyses of incremental cost versus incremental change in average disability-adjusted life years (DALYs) per patient, comparing alternative treatment strategies to standard. The analyses were performed using 10 000 second-order Monte Carlo simulation trials in the four settings. a) 5% isoniazid (INH) monoresistant tuberculosis (TB) and 1% multidrug-resistant (MDR)-TB; b) 15% INH monoresistant TB and 1% MDR-TB; c) 5% INH monoresistant TB and 10% MDR-TB; and d) 15% INH monoresistant TB and 10% MDR-TB. Average DALYs gained or lost per patient comparing each strategy (ethambutol (EMB) initial, strengthened retreatment (Str retreat) and MDR failures) to standard is shown on the x-axis, and the change in average cost per patient is shown on the y-axis. Each black circle represents the result of one simulation trial. The ellipse depicts the 95% confidence interval of the incremental cost and incremental effectiveness estimates. INT$: international US dollars.
Based on these analyses, cost-effectiveness acceptability curves comparing the three individual strategies to the baseline strategy, standard, were created (online supplementary fig. S1). EMB initial was least likely to be cost-effective in terms of cost per DALY gained compared with standard among the three alternative strategies in all settings; its probability of cost-effectiveness ranged from 11.7% to 23.7%. After accounting for statistical uncertainty, MDR failures becomes more likely to be cost-effective compared with standard than both strengthened retreatment and EMB initial as the willingness-to-pay amount per DALY gained increases. However, strengthened retreatment is more likely to be cost-effective when the willingness-to-pay amount is as follows: below $4848 per DALY gained for low prevalence of INH monoresistance (5%) and MDR-TB (1%); below $4560 per DALY gained for high INH monoresistance (15%) and low MDR-TB prevalence; below $2448 per DALY gained for low INH monoresistance and high MDR-TB (10%) prevalence; and below $2648 per DALY gained for high INH monoresistance and high MDR-TB prevalence.
Discussion
This study provides evidence that a treatment strategy incorporating a strengthened retreatment regimen containing at least one second-line drug could lead to both cost savings and increased treatment effectiveness in terms of DALYs gained, MDR-TB cases averted and TB-related deaths averted compared with one using the standard WHO retreatment regimen. This finding was true in settings with varying prevalence of drug resistance, and in several one-way sensitivity analyses. However, despite the robustness of the finding, this treatment strategy would avert fewer MDR cases and lead to less cost saving than adding EMB to the initial treatment, and would avert fewer TB deaths than either adding EMB to initial treatment or giving a standardised MDR regimen to failures of initial treatment.
We estimated that adding EMB throughout the initial standardised treatment would lead to a loss of 237–660 DALYs per 100 000 patients compared with the standardised WHO initial treatment in four settings with widely different prevalence of drug resistance. This suggests that the benefits of averting MDR-TB cases and related deaths may be outweighed by the disability endured by a larger number of patients who develop blindness. However, we found that if the assumed risk of developing blindness from 6–8 months of EMB treatment was lower than ∼0.1%, then adding EMB to the initial standardised regimen would lead to gains in DALYs, with fewer MDR-TB and deaths, and net cost savings compared with the standard initial regimen. A recently published systematic review and meta-analysis estimated that the risk of EMB-induced blindness was 0.23% (95% CI 0.0–0.61%) [14]. Given these confidence intervals, it is possible that the health gains of adding EMB could outweigh the risk of blindness in settings with a higher prevalence of INH resistance.
To assess one of the new treatment recommendations of the WHO [15], we examined the costs and treatment outcomes of empirically treating all patients who failed initial treatment with an MDR regimen. Comparing this MDR failure strategy with the standard treatment strategy, the cost per DALY gained ranged from $2857 to $5745. This would be considered cost-effective in most middle-income countries that have a per capita gross national income above that range, a commonly used ICER threshold [53–56]. This strategy was also the most likely to be cost-effective compared with the other alternative strategies if the willingness to pay ICER threshold exceeded $4560 per DALY gained.
Limitations of the study
There are several limitations of this study. In our model, we analysed closed cohorts of TB patients and did not model disease transmission. However, this would probably result in an underestimate of the benefits of treatment strategies that averted MDR-TB cases, as this would also prevent transmission of drug-resistant strains of TB. A recently published systematic review of the impact of TB on health-related quality of life reported that longer duration of TB disease, or having MDR-TB, were associated with poorer health-related quality of life [57]. As we did not account for these differences in our model, it is possible that the average DALYs per patient were overestimated, particularly for patients who received more than one treatment, or had MDR-TB. Furthermore, there is likely to be more morbidity associated with the MDR regimen compared with other treatment regimens than accounted for by a uniform disability weight applied to all patients with active TB, regardless of treatment. Thus, the effectiveness of treating failures from initial treatment with an MDR regimen could have been overestimated.
Estimates of treatment outcomes were taken from systematic reviews and meta-analyses whenever possible in order to improve precision, and reduce potential biases from selecting a small sample of individual studies known to the investigators. However, there was little published evidence for the treatment outcomes of the alternative regimens we considered. We conservatively assumed that a retreatment regimen strengthened with a second-line drug would not improve treatment outcomes for patients with MDR-TB compared with the standard WHO retreatment regimen; however, this could have underestimated the effectiveness of using the strengthened retreatment regimen. Furthermore, our estimated treatment-related costs were based on studies conducted in Ecuador, which may not be generalised to other settings, particularly those with different TB treatment practices and from different income settings. Hence, we examined these uncertainties by performing extensive sensitivity analyses. In addition, we were not able to explicitly consider HIV in the model due to the paucity of published estimates of treatment outcomes in HIV co-infected patients with drug-resistant TB treated with various regimens. Some studies have previously shown that co-infected patients may experience greater risks of relapse and mortality, while others have not found any significant differences in treatment outcome [58–61].
Policy implications
This study has shown that the prevention and treatment of drug-resistant TB is complex, and requires careful consideration of health benefits, costs and treatment-related morbidities, such as EMB-induced blindness. This study also found that empirical treatment of all patients who fail initial treatment with an MDR regimen could avert a large number of TB-related deaths. However, this would be at the cost of treating many patients with lengthy and toxic MDR treatment who would not need this. Furthermore, this strategy would not avert MDR-TB and would have little additional societal impact. The analyses presented in this study provide supportive evidence for strengthening the standard retreatment regimen. This strategy could potentially lead to cost savings, and avert MDR-TB cases and TB-related deaths, even in settings with relatively low prevalence of INH monoresistant TB.
Acknowledgments
We would like to thank R. Steffen (Federal University of Rio de Janeiro, Rio de Janiero, Brazil), and V. Rouzier and E. Leung (both McGill University, Montreal, Canada) for collecting and providing data used in this study.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support statement: Funding for this study was provided by the Canadian Institutes of Health Research (CIHR Frederick Banting and Charles Best Canada Graduate Scholarships – Master's Award).
Conflict of interest: Disclosures can be found alongside the online version of this article at www.erj.ersjournals.com
- Received January 10, 2013.
- Accepted June 7, 2013.
- ©ERS 2014
References










