





To the Editor:
We report a patient with a pulmonary squamous dysplastic lesion that appears as pure ground-glass opacity (GGO) on computed tomography (CT).
An ill-defined, 15-mm nodular lesion in the left lower lung was noted on a radiograph during an annual health check-up of a 61-year-old female who had never smoked. A physical examination and laboratory study results were unremarkable. Chest CT demonstrated a well-demarcated pure GGO nodule in the inferior lobe of the left lung. The nodule, measuring 15×13 mm, was located in the anteromedial basal segment (S8) (fig. 1a). A positron emission tomography scan showed no accumulation of radioactivity in the lesion. The patient underwent S8 segmentectomy of the left lung with lymph node sampling.

{kind=link}
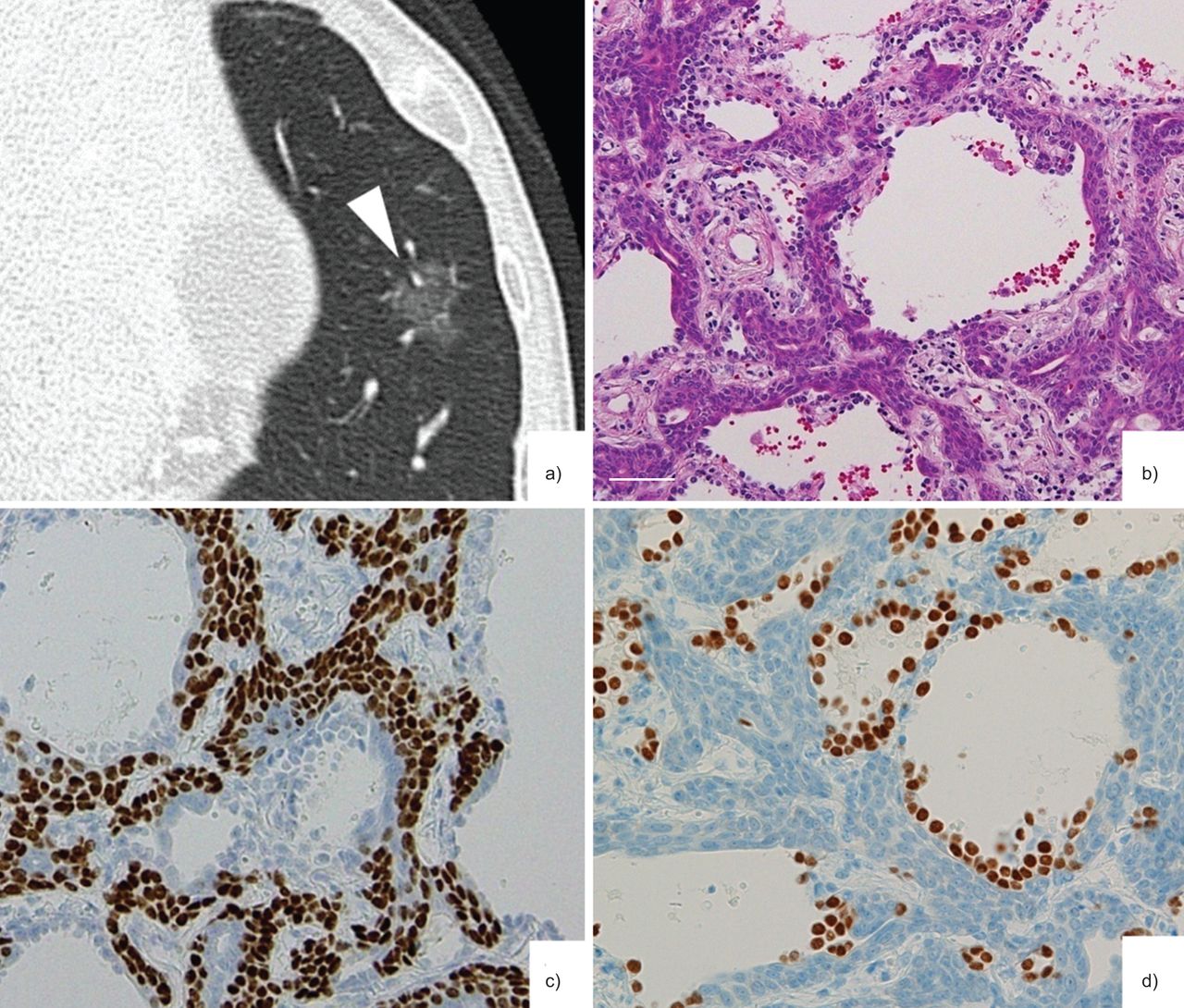
a) Chest computed tomography (CT) shows a well-demarcated pure ground-glass opacity nodule (arrowhead), measuring 15×13 mm, in the anteromedial basal segment of the left lung. b) Polygonal cells are present along the alveolar walls, but the alveolar structure is preserved (haematoxylin and eosin; scale bar=100 μm). c) Immunohistochemical staining for p63. The atypical cells were positive for p63. d) Immunohistochemical staining for TTF-1. The atypical cells were negative for TTF-1. Epithelial cells, positive for TTF-1, covered the atypical cells.
Histological examination demonstrated a well-demarcated lepidic growth pattern, similar to bronchioloalveolar carcinoma (BAC), in which the atypical cells grew along the alveolar walls, preserving the alveolar architecture. On examination of the entire specimen, the alveolar structure and air spaces were observed to be preserved in all areas of the nodule, and the histological appearance correlated with the pure GGO observed on CT. They involved the alveolar wall and developed continuously to the bronchiole. In a high-magnification view, polygonal cells with atypical nuclei proliferated between the layer of alveolar epithelial cells and the alveolar basement lamina (fig. 1b). Squamous differentiation was manifested by distinct intercellular bridges. By immunohistochemical staining, the atypical cells were positive for p63, CK5/6 and desmocollin-3, and were negative for TTF-1, indicating squamous differentiation (fig. 1c and d). The proliferation index, calculated as the percentage of Ki-67-positive cells in the carcinoma after counting at least 1000 cancer cell nuclei, was 7.9%. Based on these findings, we diagnosed this lesion as squamous dysplasia. EGFR and KRAS mutations were evaluated in DNA extracted from surgically resected tissues, using the previously described Smart Amp2 method [1]. EGFR and KRAS mutations were not detected.
This case showed a pure GGO on CT. Preoperatively, the GGO was considered to be BAC or atypical adenomatous hyperplasia (AAH). Pathologically, the polygonal cells spread along the alveolar walls, showing a lepidic growth pattern similar to that of BAC or AAH. However, squamous cell differentiation was evident due to the presence of intercellular bridges. The combination of negative staining for TTF-1 and positive staining for p63 and CK5/6 supports the diagnosis of squamous cell differentiation [2], [3]. Considering the morphology together with these immunoreactivities, the diagnosis of squamous dysplasia was confirmed.
GGO nodules most often represent BACs, and less frequently, other lesions such as AAH, lymphoproliferative disease, or organising pneumonia or fibrosis [4]. GGO nodules that represent squamous dysplasia have never been reported. Squamous dysplasia is usually found in the epithelium of the central airway, which is difficult to detect radiologically, and is considered a preneoplastic lesion leading to squamous cell carcinoma (SCC). By contrast, there are few reports of squamous dysplasia in the peripheral lung and its relevance to SCC is unknown.
Regarding SCC, development of a peripheral lesion has been discussed previously [5]–[7]. At the edge of the tumour, pulmonary SCCs have been recognised to develop along the alveolar walls. Dingermans and Mooi [5] demonstrated by electron microscopy that SCCs developed along the alveolar septa at the periphery of the tumour. Tokuda [6] confirmed similar findings by light microscopy observations and described a peripheral SCC subgroup in which cancer cells spread along the alveolar walls and proliferate between the basal membrane and epithelial cells. In a report by Kobayashi et al. [8], peripheral SCC development along the alveolar walls was observed in most parts of the tumour, showing a mixed GGO appearance on CT. Like these peripheral SCCs, the lesion in this case developed along the alveolar walls, and proliferated between the layer of alveolar epithelial cells and the alveolar basement lamina. However, the atypical cells were not invasive, resulting in the diagnosis of squamous dysplasia, not carcinoma. Consequently, the radiological finding of pure GGO represented a noninvasive lesion. These characteristics are suggestive of a precursor lesion of peripheral SCC of the lung.
In contrast to humans, squamous lung lesions often occur in rodents after toxin exposure [9], [10]. Pulmonary squamous metaplasia arising in the alveolar region caused by exposure to high burdens of particulate materials, such as talc, quartz or diesel, has been described [9]. Dioxin and dioxin-like compound intake also induces lesions, such as bronchiolar metaplasia and squamous metaplasia of the epithelium [10]. These squamous lesions are considered common reactions to the toxins; however, the incidence of SCC is low [10]. In the current case, no evidence exists regarding exposure to a toxin, such as professional exposure to particulate materials or dioxin-polluted food intake; thus, pathogenesis of the lesion remained unclear.
In conclusion, this extremely rare case is the first report of peripheral squamous dysplasia of the lung that presented as a pure GGO on CT and developed along the alveolar walls.
Footnotes
Statement of Interest
None declared.
- ©ERS 2013
REFERENCES










