



Efficacy and safety of etanercept in moderate-to-severe asthma: a randomised, controlled trial
- S.T. Holgate*⇓,
- M. Noonan#,
- P. Chanez¶,
- W. Busse+,
- L. Dupont§,
- I. Pavordf,
- A. Hakulinen**,
- L. Paolozzi##,
- J. Wajdula¶¶,
- C. Zang¶¶,
- H. Nelson++ and
- D. Raible¶¶
- *School of Medicine, University of Southampton, Southampton
- fDept of Respiratory Medicine, Thoracic Surgery and Allergy, University Hospitals of Leicester NHS Trust, Glenfield Hospital, Leicester, UK
- #Allergy Associates Research Center, Portland, OR
- +Dept of Medicine, University of Wisconsin, Madison, WI
- ¶¶Pfizer Inc., Collegeville, PA
- ++National Jewish Health, Denver, CO, USA
- ¶Département des Maladies Respiratoires, Université de la Méditerranée, Marseille
- ##Pfizer Inc., Paris, France
- §Dept of Respiratory Medicine, University Hospital Gasthuisberg, KU Leuven, Leuven, Belgium
- **Clinical Research Institute HUCH (Helsinki University Central Hospital), Skin and Allergy Hospital, Helsinki, Finland
- S.T. Holgate, III Division, Mail Point 810, Level F, South Block, Southampton General Hospital, Southampton, Hampshire, SO16 6YD, UK. E-mail: sth{at}soton.ac.uk
Abstract
Increased tumour necrosis factor-α levels have been observed in bronchial biopsies and induced sputum from subjects with severe asthma. We investigated etanercept (ETN) as a therapeutic option for treating moderate-to-severe persistent asthma.
In this 12-week, randomised, double-blind, placebo-controlled, phase 2 trial, subjects (n = 132) with moderate-to-severe persistent asthma received subcutaneous injections of 25 mg ETN or placebo twice weekly, and were evaluated at baseline, and at weeks 2, 4, 8 and 12. The primary end-point was the change from baseline to week 12 in pre-bronchodilator forced expiratory volume in 1 s (FEV1) % predicted. Secondary end-points included morning peak expiratory flow, FEV1 % pred, Asthma Control Questionnaire (5-item version), asthma exacerbations, provocative concentration of methacholine causing a 20% decrease in FEV1, and the Asthma Quality of Life Questionnaire.
No significant differences were observed between ETN and placebo for any of the efficacy end-points. ETN treatment was well tolerated, with no unexpected safety findings observed during the study.
Clinical efficacy of ETN was not shown in subjects with moderate-to-severe persistent asthma over 12 weeks. However, ETN treatment was a well-tolerated therapy. Studies in specific subsets of patients with asthma with longer-term follow-up may be needed to fully evaluate the clinical efficacy of ETN in this population.
- Asthma
- etanercept
- forced expiratory volume
Asthma is a chronic inflammatory disorder of the airways characterised by airflow obstruction, hyperresponsiveness and remodelling, leading to variable airflow obstruction [1, 2]. This inflammatory disorder involves the recruitment of eosinophils, mast cells, T-helper type 2 lymphocytes, neutrophils and macrophages, which is regulated by local release of autacoid mediators, cytokines and chemokines [3, 4].
The first line of therapy for asthma includes leukotriene modifiers and inhaled corticosteroids used alone or in combination with long-acting β2-adrenoceptor agonists (LABAs); however, ∼5–15% of subjects with severe disease either do not respond or respond incompletely to this therapy [5–7]. For subjects with severe asthma, treatment with drugs that modify the immune response, or therapies with monoclonal antibodies directed to immunoglobulin (Ig)E or interleukin-5 are effective, although efficacy appears to be restricted to specific patient subtypes [8, 9].
Tumour necrosis factor (TNF)-α is an effective therapeutic target in chronic inflammatory disorders [10]. This cytokine is predominantly produced by lymphocytes, macrophages and mast cells. TNF-α produces its pleotropic effects by interacting with two receptor subtypes, p55 and p75, and it augments inflammatory responses through multiple mechanisms, including the promotion of leukocyte adhesion and enhanced mediator release [11].
Increased levels of TNF-α have been observed in bronchial biopsies and induced sputum from subjects with severe asthma [12–15]. Monocytes and macrophages of subjects with asthma have also been shown to have higher TNF-α production compared with these cells from subjects without asthma [16]. Additionally, inhalation of TNF-α in normal individuals and those with asthma has been shown to increase airway hyperresponsiveness and cause an influx of neutrophils into the airways [17, 18]. Thus, TNF-α may play a sentinel role in maintaining the inflammatory state in subjects with asthma, especially those whose asthma is refractory to treatment with inhaled corticosteroids [19, 20].
Several clinical studies have examined the efficacy and safety of recombinant antibodies that bind and neutralise the soluble TNF-α homotrimer and its membrane-bound precursor [21]. Etanercept (ETN) is a genetically engineered recombinant protein consisting of two molecules of the extracellular portion of p75 TNF receptor, fused to the Fc portion of a human IgG1 [22]. ETN binds both TNF-á and lymphotoxin-á with high affinity.
In an open-label, pilot study, Howarth et al. [14] found that in subjects (n = 17) with severe asthma who received 25 mg ETN twice weekly as an add-on therapy for 12 weeks, ETN was associated with improvements in lung function, asthma symptoms and bronchial hyperresponsiveness. In a subsequent 10-week, double-blind, placebo-controlled trial of ETN in subjects (n = 30) with refractory asthma, similar clinical improvements occurred, including improved asthma-related quality of life [23]. However, in a small (n = 39) randomised, placebo-controlled trial, ETN did not have significant effects in patients with moderate-to-severe asthma [24].
The efficacy of other anti-TNF therapies in subjects with moderate-to-severe asthma has also not been convincing. A recent study evaluating infliximab failed to demonstrate clinical efficacy for the primary end-point in subjects with moderate asthma [3]. Similarly, no significant differences between placebo and anti-TNF-α biologic golimumab were observed in subjects with uncontrolled, severe, persistent asthma after 24 weeks of treatment, although a subgroup with more reversible airflow obstruction and upper airway disease did appear to respond in a dose-dependent manner [25].
These data suggest that severe asthma is a heterogeneous disease consisting of several subphenotypes [25, 26]. As in other complex diseases, substratification of patients with asthma according to disease phenotype and comorbidities may lead to more individualised therapies [26].
Because outcomes in previous trials of ETN in subjects with moderate-to-severe asthma have been so variable [14, 23, 24], this study was designed to provide additional data from a larger number of subjects on the effect of ETN in this population.
METHODS AND MATERIALS
Study design
This was a 12-week, randomised, parallel, double-blind, placebo-controlled, worldwide phase 2 trial evaluating the efficacy and safety of ETN in subjects with moderate-to-severe persistent asthma conducted at 36 sites (ClinicalTrials.gov identifier NCT00141791). Clinical evaluations were performed at screening and baseline, at weeks 2, 4, 8 and 12, and during a follow-up period of 2−4 weeks. Eligible subjects were randomised to subcutaneous injection of either 25 mg ETN or placebo twice weekly.
This study was undertaken in accordance with the ethical principles of the Declaration of Helsinki. The protocol and its amendments received independent ethics committee or institutional review-board approval before site initiation and recruitment of subjects. All elements of informed consent were explained to eligible subjects, and adequate time was allowed for questions and for subjects to make voluntary decisions. No subject underwent procedures specific to the protocol until he or she had signed and dated an approved informed consent form.
Subjects
Subjects (aged 18–70 yrs) were included in the study if they had been diagnosed with moderate-to-severe persistent asthma as defined by the National Heart, Lung and Blood Institute (NHLBI) [27] ≥1 yr before randomisation. All subjects demonstrated ≥9% actual reversibility from the pre-bronchodilator baseline forced expiratory volume in 1 s (FEV1) with inhaled albuterol during screening or at baseline, and had an FEV1 of 50–80% predicted ≥6 h after a short-acting β2-agonist or 12 h after a LABA at screening or baseline. Subjects were also required to: have a mean score of ≥2 on the Asthma Control Questionnaire (5-item version; ACQ-5) [28], be taking a high-dose inhaled corticosteroid (≥1,000 μg·day−1 beclomethasone–chlorofluorocarbons, 500 μg·day−1 beclomethasone–hydrofluoroalkane, 500 μg·day−1 fluticasone or 1,000 μg·day−1 budesonide, or equivalent); and be receiving stable doses of their current medications for asthma ≥4 weeks prior to randomisation. Females needed to have a negative pregnancy test at screening, and all sexually active females and males were to use a medically acceptable contraceptive during the study.
Subjects were excluded from the study if they had: previous treatment with ETN, antibody to TNF-α or other TNF-α inhibitors; investigational biologic agents ≤3 months prior to randomisation; any live (attenuated) vaccines ≤4 weeks prior to randomisation; or were currently using cigarettes or cigars, or had a smoking history >10 pack-yrs. Also excluded from the study were subjects with: abnormal blood chemistry or haematology profiles; respiratory tract infection ≤4 weeks before baseline; significant concurrent medical conditions at the time of screening, including chronic obstructive pulmonary disease, active infections or underlying disease, tuberculosis, uncontrolled hypertension, class III–IV or uncompensated congestive heart failure, multiple sclerosis, uncontrolled insulin-dependent diabetes mellitus, any rheumatologic disease, cancer or history of cancer, known HIV, presence of hepatitis B or C antigens; psychiatric illnesses; or history of drug or alcohol abuse.
The subjects were permitted to continue inhaled and oral corticosteroids (≤12.5 mg prednisone or equivalent), inhaled LABAs, leukotriene antagonists, cromones, antihistamines, and allergen immunotherapy if the maintenance dose was stable for 3 months. Prohibited treatments included oral corticosteroids (>12.5 mg prednisone or equivalent), inhaled anticholinergics, theophylline, oral β2-agonists, systemic immunosuppressive agents (methotrexate and cyclophosphamide), β-blockers, any live (attenuated) vaccine, and other TNF-α antagonists or biologics.
Efficacy end-points
The primary efficacy end-point was the change in pre-bronchodilator FEV1 % pred from baseline to week 12. Secondary end-points included: morning pre-bronchodilator peak expiratory flow (PEF); FEV1 % pred at weeks 2, 4 and 8; ACQ-5 score; provocative concentration of methacholine causing a 20% decrease in FEV1 (PC20), measured by either the tidal breathing method or the dosimeter method (site preference); Asthma Quality of Life Questionnaire (AQLQ) score [29]; and asthma exacerbations, which were defined as unscheduled visits requiring de novo systemic corticosteroids or an increase in the dose of oral corticosteroids, an emergency room visit, or hospitalisation.
Statistical analysis
60 patients per treatment group yielded ∼90% power to detect a 10% point difference in the change of FEV1 % pred from baseline between the ETN and placebo groups, assuming the standard deviation of the change of FEV1 from baseline to week 12 was 16%, and a two-sided t-test was used to compare at a significance level of p<0.05.
Efficacy analysis was performed on the intent-to-treat (ITT) population, which included all randomised subjects and was the primary population for efficacy analysis. Safety was analysed for all subjects who received at least one dose of study medication.
Change from baseline in FEV1 % pred was calculated at each time-point and analysed using an ANCOVA, with baseline FEV1 measurement used as a covariate and treatment group as a factor. Paired t-tests were used for the comparisons of changes from baseline within treatment groups for the ITT population at each time-point.
Secondary efficacy end-points were analysed using ANCOVA, with the corresponding baseline measurement for the variable used as the covariate. A “last observation carried forward” approach was used for missing values for analysis of the ITT population.
RESULTS
Subject disposition
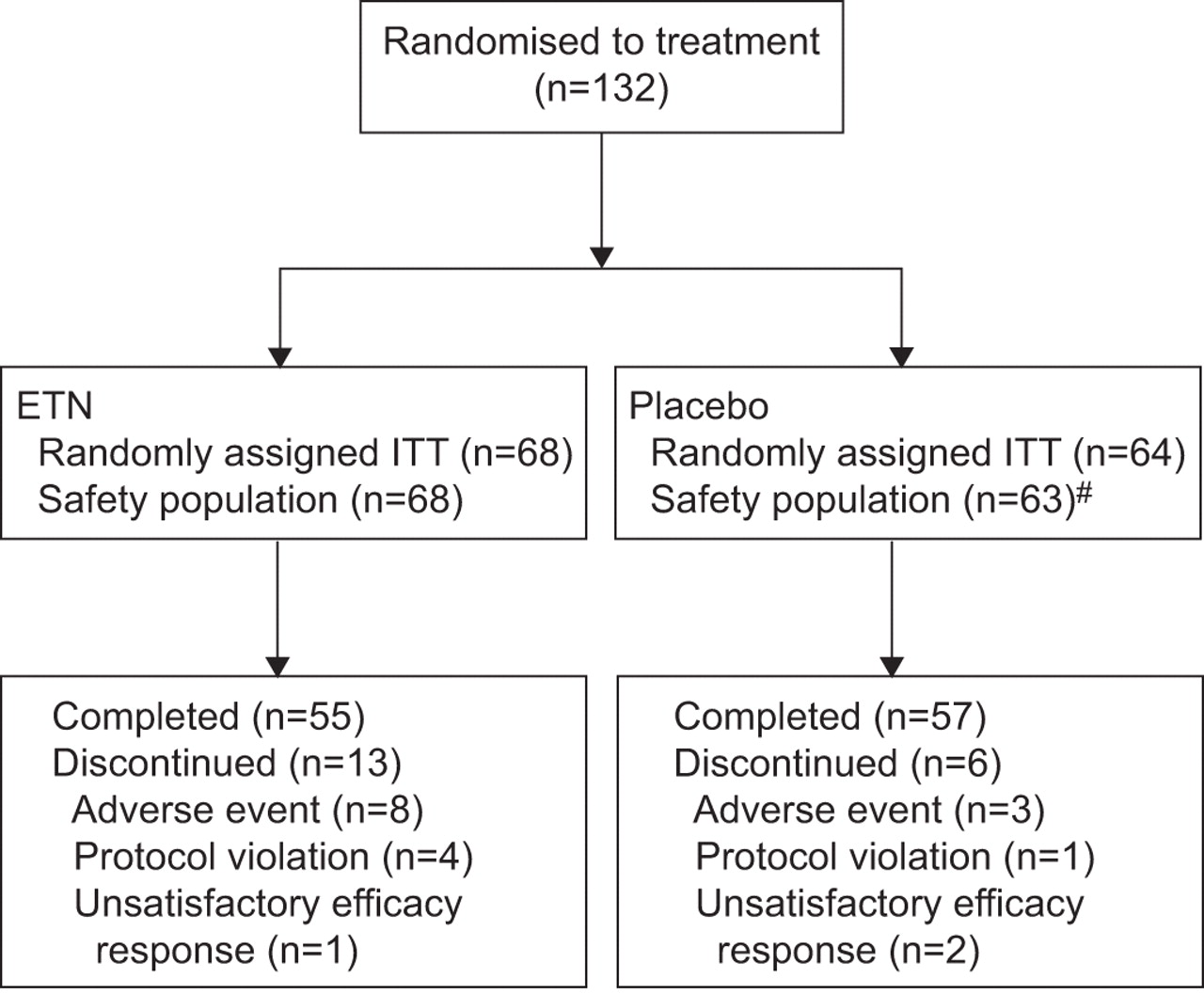
In total, 132 subjects were randomised (ITT population); however, one subject randomised to placebo did not receive study medication. Therefore, 131 subjects were included in the safety analysis. The disposition of all subjects randomised to treatment is shown in figure 1. No significant differences in baseline and demographic characteristics were observed between treatment groups for the safety population (table 1). At the time of enrolment, 90% of the subjects taking ETN and 89% of the subjects receiving placebo were using inhaled LABAs.

Subject disposition. ETN: etanercept; ITT: intent-to-treat population. #: one subject randomised to placebo did not receive the study medication.
Clinical efficacy
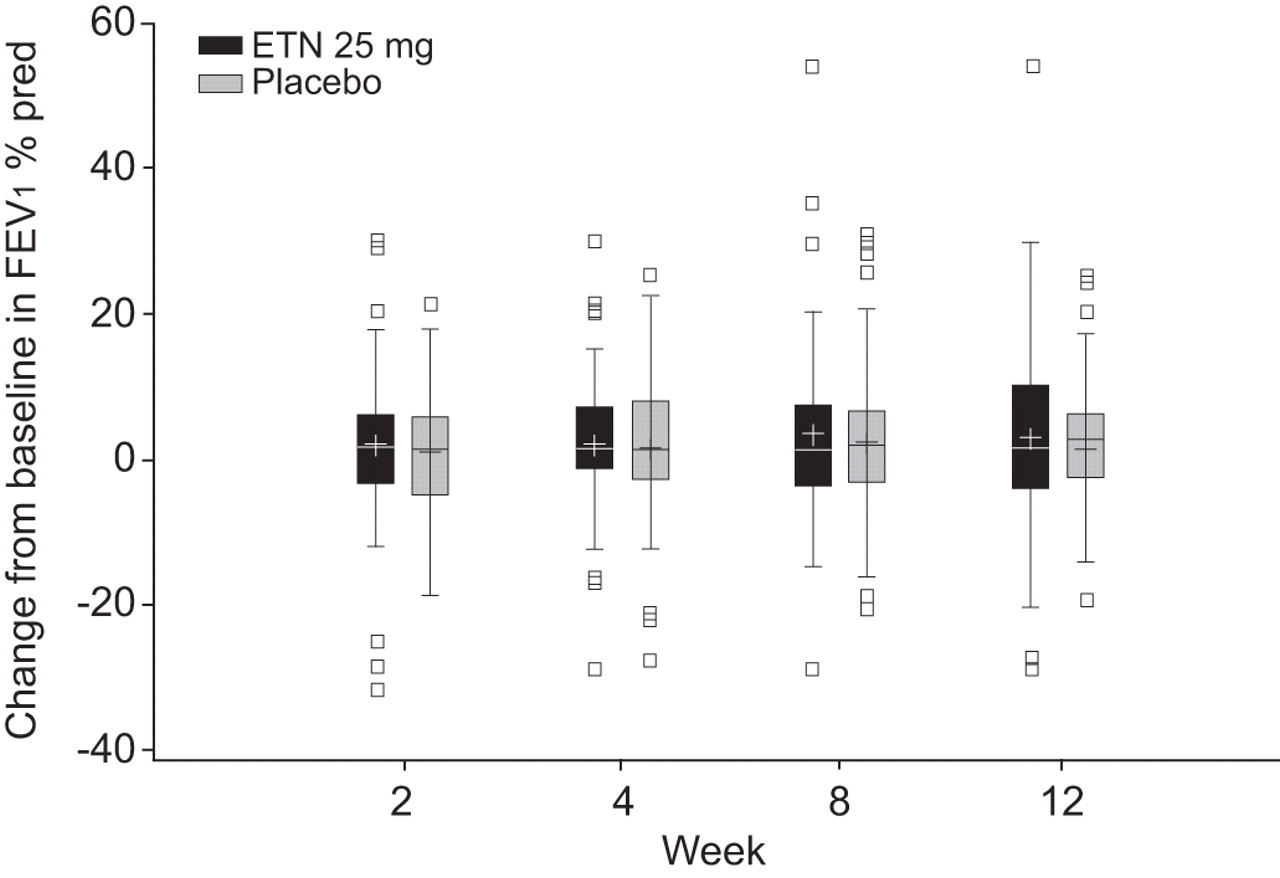
No statistically significant differences between ETN and placebo were shown for any of the primary or secondary end-points. At week 12, the adjusted mean±se changes from baseline in FEV1 % pred were 3.0±1.3 and 1.7±1.3% for the ETN and placebo groups, respectively. No significant changes from baseline were observed between treatments for the primary efficacy end-point at weeks 2, 4 or 8 (fig. 2).

{kind=link}
{kind=link}
Box and whisker plots for change from baseline in forced expiratory volume in 1 s (FEV1) % predicted in the intent-to-treat population (last observation carried forward). At week 12, the adjusted mean±se change from baseline in FEV1 % pred was 3.0±1.3% for the etanercept (ETN) group, compared with 1.7±1.3% for the placebo group. No significant difference between treatments was observed (p = 0.51). Similar findings were observed at weeks 2, 4, and 8. Boxes represent interquartile range (IQR) and whiskers represent the minimum and maximum values with 1.5 IQR; —: median; +: mean; □: outliers.
Results for the secondary clinical efficacy end-points are provided in table 2. At week 12, morning PEF, ACQ-5 score, asthma exacerbations, methacholine PC20 and AQLQ score were not significantly different between subjects taking ETN and those taking placebo. Methacholine challenge testing was required for all subjects in the study, unless contraindicated by local guidelines. At baseline, only 16 ETN and 12 placebo subjects had PC20 determinations, and at week 12, only nine ETN and 12 placebo subjects completed the PC20 methacholine challenge.
Subgroup analyses were performed to examine whether there was greater efficacy of ETN among subjects who were taking oral corticosteroids at baseline had lower baseline FEV1 % pred or greater FEV1 reversibility after administration of short-acting β-agonists. At week 12, no significant difference in FEV1 % pred between ETN and placebo subjects was observed among either those taking oral steroids or those who were not (data not shown). Likewise, no significant differences at week 12 between treatments were evident when the data were analysed by FEV1 % pred tertiles (≤60%, >60% and ≤71.5%, and >71.5% pred; data not shown). Furthermore, no significant difference between ETN and placebo was shown for FEV1 reversibility when results were analysed by tertile subgroups (≤16%, >16% and ≤24%, and and >24% improvement from pre-bronchodilator FEV1 % pred at baseline; data not shown).
Safety
The frequency of treatment-emergent adverse events (AEs) did not differ significantly between the treatments (table 3). Noninfectious AEs occurred in 41 (60%) subjects in the ETN group compared with 31 (49%) subjects in the placebo group (p = 0.222; table 3). The most common noninfectious AE reported was injection site reaction, occurring more frequently in the ETN group than in the placebo group (36 versus 11%, respectively; table 3).
Treatment-emergent infections were reported in 30 (44%) ETN subjects compared with 34 (54%) placebo subjects; the most common treatment-emergent infection was respiratory tract infection (table 3). No significant difference in the incidence of any infection was shown between the ETN and placebo groups.
There was one serious noninfectious AE reported in the study. This was an anaphylactoid reaction that occurred in a subject in the ETN group and was temporally related to ETN administration (table 4). Subjects reporting serious or medically important infectious AEs are shown in table 4. The incidence of serious or medically important infections was not significantly different between treatments (ETN: two (2.9%) subjects; placebo: five (7.9%) subjects). No deaths or malignancies were reported during the 12-week study or during the 2–4 weeks of follow-up. Eight ETN subjects and three placebo subjects discontinued from the study because of AEs (fig. 1). Overall, ETN was well tolerated, and there were no unexpected safety findings in this study population.
DISCUSSION
This study evaluated the efficacy and safety of 25 mg ETN administered twice weekly by subcutaneous injection in subjects with moderate-to-severe persistent asthma. ETN failed to demonstrate clinical efficacy on any of the clinical or lung function end-points in this study population of subjects who predominately had severe asthma. These findings contrast with those from earlier, smaller studies of various study designs, investigating the clinical efficacy of ETN in different asthmatic study populations, which showed that ETN was associated with significant improvements in asthma symptoms, airway hyperresponsiveness and quality of life [14, 23].
Although the negative findings from the present study are consistent with the results of other small placebo-controlled ETN trials reported by Morjaria et al. [24] (n = 39; 12-week study) and Rouhani et al. [30] (n = 21; 2-week study), and with the outcomes of controlled studies involving other anti-TNF agents, including infliximab for 8 weeks (n = 38) [3] and golimumab for 24 weeks (n = 309) [25], the current findings should be viewed in the context of the study design. First, it is important to note that the subjects included in this study were categorised as having moderate-to-severe asthma according to the NHLBI guidelines [27]. Therefore, the asthma in this population may not have been as severe as in other studies with ETN. However, in a randomised, placebo-controlled trial of 39 subjects with severe, corticosteroid-refractory asthma, no significant differences between 12 weeks of ETN or placebo were found for certain end-points, specifically, improvements in AQLQ scores, lung function, morning PEF, bronchial hyperresponsiveness or exacerbation rates [24]. In contrast to the study by Morjaria et al. [24] and the present study, Berry et al. [23] (n = 20) reported that 10 weeks of ETN compared with placebo was associated with an improvement in PC20, AQLQ and post-bronchodilator FEV1 in subjects with refractory asthma. Furthermore, the subjects in the current study demonstrated less airway hyperresponsiveness to methacholine at baseline than those studied by Berry et al. [23], and also Howarth et al. [14], who had reported asthma-symptom improvements with 12 weeks of ETN in an open-label, uncontrolled study. Taken together, these observations suggest that, given the heterogeneous nature of asthma, the severity of the disease may be critical in data analysis and interpretation. Furthermore, selection of patients with noneosinophilic asthma may have yielded different results, as patients with eosinophilic asthma had reduced levels of TNF from sputum cells relative to those in patients with noneosinophilic asthma [31].
Secondly, the short-term follow-up of 12 weeks may not have been adequate to observe a clinically significant response with ETN in this particular study population. Studies with longer term follow-up may be required. Additionally, this 12-week study was too short to observe any malignancies with etanercept. However, eight malignancies were previously reported by Wenzel et al. [25] in a 76-week safety analysis of golimumab treatment in 309 patients with severe persistent asthma.
Thirdly, the study lacked biochemical analyses of TNF-α or other clinically important biomarkers. In the study by Berry et al. [23], expression of membrane-bound TNF-α on peripheral blood mononuclear cells correlated with responsiveness to ETN. In hindsight, a similar analysis of TNF-α status might have provided a biomarker of responsiveness to ETN. This biomarker approach to subphenotyping of severe asthma has recently been successful in identifying responders to the anti-interleukin-5 monoclonal antibody mepolizumab, using sputum eosinophilia, despite the use of high-dose corticosteroids as an enrolment criterion [8, 9]. However, in another study of an unselected population of patients with severe asthma, mepolizumab was found to be ineffective [32].
In the present study, standard analyses were used to evaluate lung function, symptoms and airway responsiveness in patients with asthma. Based on the results from the recent study of golimumab showing possible benefits among subjects with FEV1 reversibility >12% at baseline, we attempted to analyse our data in a similar manner. Because we required FEV1 reversibility of ≥9% during the screening period for subject eligibility, there were only seven ETN and 10 placebo subjects with FEV1 reversibility <12%, so we analysed our data by FEV1 reversibility tertiles. However, these analyses showed no significant difference between ETN and placebo for FEV1 reversibility by tertile subgroup (≤16%, >16% and ≤24%, and >24% improvement from pre-bronchodilator FEV1 % pred at baseline). Severe corticosteroid refractory asthma is characterised by reduced bronchodilator reversibility, possibly as a consequence of airway wall remodelling [33, 34]. It remains possible that selection of patients on the basis of greater bronchodilator response and/or bronchial hyperresponsiveness might have revealed some efficacy.
With regard to safety, no unexpected findings were observed during this study. ETN was shown to be a well-tolerated therapy. The occurrence of infections in this study was similar to that observed in previous studies examining the efficacy of ETN in subjects with asthma [3, 14]. These safety findings are consistent with the favourable safety profile associated with the long-term administration of 25 mg ETN twice weekly for other indications. However, in a 24-week study that included ≤76 weeks of follow-up, subjects with severe asthma treated with golimumab had a significantly higher rate of infection than those in the placebo arm [25]. One possible explanation for the lower infection rate with ETN than with other anti-TNF-α monoclonal antibodies may be the lesser binding affinity of ETN for membrane-bound TNF-α as compared with that of the monoclonal antibodies. This may prevent or lessen the rate of apoptosis of immunocompetent cells [35, 36]. A previous report showed that infliximab and adalimumab, but not ETN, induced apoptosis and cell-cycle arrest in T-cells transfected with transmembrane TNF-α [37]. These findings suggest that different anti-TNF-α therapies have different biologic effects on transmembrane TNF-α. Additional studies are needed to fully characterise the differences in the mechanisms of the anti-TNF-α therapies.
In conclusion, the safety profile for ETN in subjects with moderate-to-severe persistent asthma is similar to that seen in subjects with other inflammatory diseases, such as rheumatoid arthritis, ankylosing spondylitis, psoriasis and psoriatic arthritis [38–41]. Considering the efficacy findings from this study as well as from the studies with golimumab and infliximab, it seems unlikely that asthma will be among the chronic inflammatory disorders for which TNF blockade is indicated. Although there is ample evidence that TNF-α is generated in asthmatic airways, its role in disease causation is questionable. Nonetheless, this may not exclude a small subgroup of subjects with asthma in whom TNF-α may play a prominent role. Future studies are warranted to investigate the role of TNF blockade in the aetiology of asthma and to gain a better understanding of the specific asthmatic study population suitable for TNF-α therapy.
Acknowledgments
Medical writing support for this manuscript was provided by C. Bradley (Precise Publications LLC, Pluckemin, NJ, USA) and was funded by Wyeth, which was acquired by Pfizer Inc. in October 2009. The authors thank the other investigators who participated in the study: R. Niven (Wythenshawe Hospital, Manchester, UK), B. Higgins (Sir William Leech Centre, Freeman Hospital, Newcastle upon Tyne, UK), S.H. Arshad (University Hospital of North Staffordshire, Stoke-on-Trent, UK), R. Makitaro (Oulu University Hospital, Oulu, Finland), S. Saarelainen (Tampere University Hospital, Pikonlinna, Finland), G. Stalenheim (Lungkliniken, Dept of Pulmonary Disease, Uppsala, Sweden), R. Louis (Centre Hospitalier Universitaire de Liege, Sart Tilman, Belgium), M. Daenen (Erasmus, Genk, Belgium), Hendrich Timmer (Streekziekenhuis Midden Twente, Hengelo, the Netherlands), M. Aubier (Hôpital Bichat, Centre d’Investigation Clinique, Paris, France), P. Chanez (Hôpital Arnaud de Villeneuve, Montpellier, France), M. Humbert (Hopital Antoine Béclère, Clamart, France), J. Schul (Virginia Adult and Pediatric Allergy and Asthma PC, Richmond, VA, USA), A. Halsey (Brandon-Valico Center for Allergy and Asthma Research LLC, Valrico, FL, USA), R. Saff (Allergy and Asthma Diagnostic Treatment Center, Tallahassee, FL, USA), M. White (Institute for Asthma and Allergy, Wheaton, MD, USA), H. Windom (Adult and Peadiatric Allergy, Sarasota, FL, USA), S. Goldstein (Allergy and Asthma Care of Long Island, Commack, NY, USA), I. Tillie-Leblond (Hôpital Albert Calmette, Lille, France), G. Serfilippi (Pulmonary and Critical Care Services PC, Albany, NY, USA), J. Gluck (Florida Center for Allergy and Asthma Research, Miami, FL, USA), M. Tarpay (Allergy and Asthma Center, Oklahoma City, OK, USA), D. Cypcar (Regional Allergy and Asthma, Asheville, NC, USA), K. Drain (Spokane Allergy and Asthma Clinic, Spokane, WA, USA), T. Lee (Peachtree Allergy and Asthma Clinic PC, Atlanta, GA, USA), B. Goodman (Aero Allergy Research Labs of Savannah Inc., Savannah, GA, USA), J. Given (Allergy and Respiratory Center, Canton, OH, USA) and J. Corren (Allergy Medical Clinic, Los Angeles, CA, USA).
Permission to use the ACQ-5 was kindly provided by E.F. Juniper (Qoltech, Bosham, UK).
Footnotes
Support Statement
This study was sponsored by Wyeth, which was acquired by Pfizer Inc. in October 2009. Medical writing support for this manuscript was provided by C. Bradley (Precise Publications LLC, Pluckemin, NJ, USA) and was funded by Wyeth.
Clinical Trial
This study is registed at ClinicalTrials.gov with identifier number NCT00141791.
Statement of Interest
Statements of interest for S.T. Holgate, M. Noonan, P. Chanez, I. Pavord, A. Hakulinen, L. Paolozzi, J. Wadjula, C. Zang, H. Nelson, D. Raible and the study itself can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received April 23, 2010.
- Accepted October 26, 2010.
- ©ERS 2011