





Abstract
Ventilator-associated pneumonia (VAP) affects mortality, morbidity and cost of critical care. Reliable risk estimation might improve end-of-life decisions, resource allocation and outcome. Several scoring systems for survival prediction have been established and optimised over the last decades. Recently, new biomarkers have gained interest in the prognostic field. We assessed whether midregional pro-atrial natriuretic peptide (MR-proANP) and procalcitonin (PCT) improve the predictive value of the Simplified Acute Physiologic Score (SAPS) II and Sequential Related Organ Failure Assessment (SOFA) in VAP.
Specified end-points of a prospective multinational trial including 101 patients with VAP were analysed. Death <28 days after VAP onset was the primary end-point.
MR-proANP and PCT were elevated at the onset of VAP in nonsurvivors compared with survivors (p = 0.003 and p = 0.017, respectively) and their slope of decline differed significantly (p = 0.018 and p = 0.039, respectively). Patients with the highest MR-proANP quartile at VAP onset were at increased risk for death (log rank p = 0.013). In a logistic regression model, MR-proANP was identified as the best predictor of survival. Adding MR-proANP and PCT to SAPS II and SOFA improved their predictive properties (area under the curve 0.895 and 0.880).
We conclude that the combination of two biomarkers, MR-proANP and PCT, improve survival prediction of clinical severity scores in VAP.
- Biomarker
- midregional pro-atrial natriuretic peptide
- procalcitonin
- prognosis
- risk stratification
- ventilator-associated pneumonia
Ventilator-associated pneumonia (VAP) remains an important cause of mortality despite therapeutical and preventive advances 1. Up to one-third of all mechanically ventilated patients develop pneumonia and mortality may exceed 50% in particular groups 2, 3. Furthermore, VAP is associated with a significant increase in hospital stay and excess costs exceed US$ 40,000 per patient 4. Outcome in VAP is determined by several factors, including host characteristics, such as immunological status and comorbidities, intrinsic characteristics of the infection and therapeutic measures 5. In this context, different clinical presentations, ranging from subtle to very obvious, combined with severe underlying diseases, make risk stratification in VAP particularly challenging. Several clinical severity scores, such as the Acute Physiology and Chronic Health Evaluation (APACHE), Simplified Acute Physiological Score (SAPS) and Sequential Related Organ Failure Assessment (SOFA), have been shown to predict outcome in critically ill patients 6. However, most of them are time-consuming and lack clinical usability. Recently, circulating biomarkers have been suggested for outcome prediction in infection 7, 8.
Pro-atrial natriuretic peptide (pro-ANP, amino acids 1–98), a stable fragment of the atrial natriuretic peptide (ANP) precursor, is secreted in in equimolar quantities with ANP 9. ANP is a member of the natriuretic peptide family, which, together with the associated prohormones, comprises established markers of congestive heart failure 10. N-terminal proANP has shown to be of prognostic relevance in cardiovascular disease and myocardial infarction 11. Furthermore, a significant difference in proANP levels between survivors and nonsurvivors has been assessed in respiratory tract infections including pneumonia, sepsis and VAP 12–15.
Procalcitonin (PCT) is a classical hormokine, which is secreted next to the hormonal pathway in a cytokine-like manner 16. Besides being well known for its diagnostic performance in bacterial conditions, PCT also provides prognostic information 7, 17–19. Accordingly, high and increasing PCT levels were independent predictors of death in critically ill patients, including those with VAP 20–23.
Patients developing VAP are mechanically ventilated for severe underlying disease. Therefore, we investigated whether the combination of two biomarkers, assessing the haemodynamic (midregional (MR)-proANP) and the infectious (PCT) consequences of VAP, could add to the predictive value of clinical severity scores. We analysed data of a well-characterised cohort of 101 patients with clinically diagnosed VAP. The primary end-point was death <28 days after VAP onset.
MATERIALS AND METHODS
Setting and study population
Data from a prospective multicentre trial including 101 patients with clinically diagnosed VAP were analysed 24. In brief, the main objective of the study was to evaluate PCT-guided antibiotic de-escalation in VAP compared to usual care. The study took place in seven medical and surgical intensive care units (ICUs) (UMass Memorial Medical Center, Worcester, MA, USA; University Hospital Lausanne, Lausanne, Switzerland; and University Hospital Basel, Basel, Switzerland). The analysis of prognostic predictors in the study population was a predefined secondary end-point of the protocol. The study was approved by the institutional review boards of all participating institutions and registered in the Current Controlled Trials Database as “ProVAP”-Study (identifier number ISRCTN61015974). Written informed consent was obtained from all included patients or their legal representatives.
Diagnostic criteria
Diagnosis of VAP was established using a clinical approach, according to the American Thoracic Society guidelines 1, 25. It was defined as a new or progressive infiltrate on chest radiography associated with at least two out of the following: purulent tracheal secretions, fever (body temperature >38°C (100.4°F)), and leukocytosis or leukopenia (leukocyte count >11,000 or <3,000 cells·μL−1, respecitively). ICU patients were eligible for the study if they met all the following criteria: 1) intubated for mechanical ventilation for ≥48 h; 2) >18 yrs; and 3) clinically diagnosed VAP. Patients were excluded if they: 1) were pregnant; 2) were enrolled in another trial; 3) had received immunosuppressants or long-term corticosteroid therapy (>0.5 mg·kg−1·day−1 for >1 month); 4) were immunosuppressed; or 5) had a coexisting extrapulmonary infection diagnosed in the first 3 days and requiring antibiotic therapy for ≤3 days. Microbiologically confirmed VAP was defined by a significant growth of quantitative cultures of endotracheal aspirates, bronchoalveolar lavage or protected specimen brush specimens 1.
Baseline assessment and follow-up
At the time of enrolment, the following information was recorded from each subject: age, sex, pre-existing comorbidities, severity of the underlying medical condition(s), primary reason for initiating mechanical ventilation, duration of prior mechanical ventilation, antibiotic use within 14 days of VAP onset, body temperature, heart rate, mean arterial pressure (MAP), arterial oxygen saturation (Sa,O2), arterial oxygen tension (Pa,O2)/inspiratory oxygen fraction (FI,O2) ratio, leukocyte count (white blood cells; WBCs), and MR-proANP and PCT serum levels. The following indices were calculated: SAPS II, SOFA score, Organ Dysfunction and/or Infection (ODIN) score and Clinical Pulmonary Infection Score (CPIS). During the 28-day follow-up period, the following information was recorded: body temperature; heart rate; MAP; Sa,O2; Pa,O2/FI,O2; WBCs; SOFA, ODIN and CPIS; mechanical ventilation status; antibiotic use; and survival throughout the 28-day study period. Serum MR-proANP and PCT levels were determined at VAP onset and daily for 10 consecutive days after VAP diagnosis.
Outcome assessment
All patients were followed-up for 28 days or until death. Patients deceased before day 28 were classified as nonsurvivors; all others were classified as survivors. No patient was lost to follow-up.
MR-proANP and PCT measurements
MR-proANP measurements were performed with 50 μL serum using a test based on the time-resolved amplified cryptate emission (TRACE) technology (MR-proANP KRYPTOR; BRAHMS AG; Hennigsdorf, Germany). The lower detection limit of the assay is 6 pmol·L−1 and the functional assay sensitivity (defined as the lowest value with an interassay coefficient of variation <20%) is 23 pmol·L−1 9. The median MR-proANP level of healthy subjects was 45 pmol·L−1. PCT was measured in 50 μL serum using TRACE technology (PCT sensitive KRYPTOR; BRAHMS AG; Hennigsdorf, Germany). A lower detection limit of 0.02 ng·mL−1 and a functional assay sensitivity of 0.06 ng·mL−1 were identified 26.
Statistical analyses
Discrete variables are presented as n (%) and continuous variables as median (interquartile range (IQR)). Comparability of groups was analysed by Chi-squared test, Fisher’s exact test or Mann–Whitney U-test, as appropriate. Correlation analyses were performed using Spearman’s ρ. To detect the time-course of the biomarkers across survivors and nonsurvivors, a linear mixed-effect model with the fixed factors day, group and random factor subject was performed on the log-transformed parameters. In order to study possible different time-courses, the interaction between day and group was determined. The log-transformed values of the markers at VAP onset were also included in the model to adjust for potential different baseline values in the study groups. Time to death was analysed by Kaplan–Meier survival curves and compared by the log rank test. Area under the curve (AUC) values for receiver operating characteristic (ROC) curves were calculated from logistic regression models in which each factor enters individually or combined. Values are calculated from a nonlinear regression model where each predictor is modelled as a five-knot cubic spline 27. AUC values are presented as mean±se. In order to predict survival, an L1-penalised logistic regression model was performed. This is an adaptation of Lasso regression to generalised linear models 28. This approach is justified when the number of predictors is large compared with the number of observations and over-fitting has to be considered. Cut-offs with the highest accuracy were identified using the Youden’s index (maximal difference between sensitivity and 1-specificity). Nomograms provide excellent graphical depictions of the variables in a regression model, in addition to enabling the user to obtain predicted values manually. A nomogram was calculated using R version 2.9.2 (R Development Core Team, Vienna, Austria). All tests were two-tailed; p-values of <0.05 were defined as significant. Data were analysed using statistical software (Statistical Package for Social Sciences version 16 for Windows; SPSS, Chicago IL, USA).
RESULTS
Baseline characteristics
A total of 101 patients were included in the study. Detailed baseline characteristics for survivors and nonsurvivors are summarised in table 1. The median age was 57 yrs (IQR 43–70 yrs). Cardiac comorbidities were reported as follows: arterial hypertension (n = 31), coronary artery disease (n = 30), myocardial infarction (n = 17), cardiac arrhythmia (n = 16), congestive heart failure (n = 11) and aortic aneurysm (n = 5). Microbiological analyses of respiratory tract secretions identified a causative organism in 74 (76%) patients. The most frequently isolated bacteria were Staphylococcus aureus (30%), Pseudomonas aeruginosa (25%) and Klebsiella species (13%). 75% of all patients received antibiotics within 14 days prior to study inclusion. Appropriate initial antibiotic therapy, defined as a regimen combining an aminoglycoside or a fluoroquinolone plus a β-lactam or an antipseudomonal carbapenem, was applied in 86% of cases. 20 patients died during the study period. Deaths were due to traumatic brain injury/subarachnoid hemorrhage (n = 8), respiratory failure/acute respiratory distress syndrome (n = 5), septic shock (n = 3), cardiogenic shock (n = 2), multiorgan failure (n = 1) and acute liver failure (n = 1).
MR-proANP in VAP
At VAP onset, median MR-proANP was 163 pmol·L−1 (IQR 98–374 pmol·L−1). Elevated MR-proANP was associated with age, heart rate, MAP, and the presence of cardiac, pulmonary and renal comorbidities (tables 2 and 3). MR-proANP was significantly elevated in nonsurvivors (median 373 pmol·L−1 (IQR 114–784 pmol·L−1) versus 149 pmol·L−1 (IQR 93–278) pmol·L−1; p = 0.003). There was a significant effect of the interaction between day and group, reflecting a different decrease of MR-proANP in survivors and nonsurvivors (p = 0.018; fig. 1a). Kaplan–Meier survival function was significantly different across MR-proANP quartiles at VAP onset (log rank p = 0.013; fig. 2). In ROC analysis, the mean±se AUC of MR-proANP at VAP onset to predict mortality was 0.801±0.062. An MR-proANP threshold of 660 pmol·L−1 had the highest accuracy for predicting death. The associated sensitivity and specificity were 45% and 97%, respectively. Accordingly, the positive likelihood ratio was 17.3. We assessed a positive and negative predictive value of 82% and 87%. The use of the 660-pmol·L−1 MR-proANP cut-off yielded an odds ratio of 30.7 (95% CI 5.9–161.0) for predicting death at VAP onset.

Time-course of a) midregional pro-atrial natriuretic peptide (MR-proANP; p = 0.018) and b) procalcitonin (PCT; p = 0.039) during the first 10 days after ventilator-associated pneumonia onset, comparing survivors (n = 81) and nonsurvivors (n = 20); p-values are in respect of biomarker trend over time, in survivors and nonsurvivors.

Kaplan–Meier estimates of the survival probability within 28 days of ventilator-associated pneumonia onset in midregional pro-atrial natriuretic peptide quartiles of 0–98 (–—), 99–164 (-----), 165–360 (– – –) and >361 pmol·L−1 (···). Log rank p = 0.013.
PCT in VAP
Median PCT on VAP onset was 0.69 ng·mL−1 (IQR 0.22–2.34 ng·mL−1) and significantly correlated with Sa,O2, renal disease and sex (tables 2 and 3). Age, and cardiac and pulmonary comorbidities did not influence PCT levels. PCT levels were significantly elevated in nonsurvivors (1.36 ng·mL−1 (IQR 0.38–6.04 ng·mL−1) versus 0.58 ng·mL−1 (IQR 0.19–2.00 ng·mL−1); p = 0.017). A significant effect of the interaction between day and group indicates a different decrease of the marker across the time (p = 0.039; fig. 1b). The median relative decrease of PCT within 72 h after VAP onset was 26% in survivors and 7% in nonsurvivors. PCT quartiles did not differ in survival (log rank p = 0.076). The mean±se AUC for PCT on VAP onset to predict mortality was 0.712±0.069.
Combination of MR-proANP, PCT and ICU scores
At VAP onset, the mean±se AUCs of SAPS II and SOFA to predict 28-day mortality were 0.736±0.067 and 0.768±0.065, respectively (fig. 3a and b). 25 parameters, such as age, vital signs, laboratory values, comorbidities, SAPS II, SOFA, ODIN, and PCT and MR-proANP serum levels at VAP onset were included in an L1-penalised logistic regression model analysing 28-day survival. MR-proANP was identified as the best predictor of survival, followed by SOFA and SAPS II. Adding MR-proANP at VAP onset to clinical scores significantly improved the AUC for SAPS II to 0.859±0.055 (p = 0.024). The AUC of SOFA plus MR-proANP was enhanced to 0.848±0.056 (p = 0.095). A further refinement of the model was achieved by including PCT at VAP onset. SAPS II in conjunction with MR-proANP and PCT significantly improved survival prediction compared with SAPS II alone (AUC 0.895±0.048; p = 0.003; fig. 3a). Similarly, predictive properties of SOFA increased by adding MR-proANP and PCT (AUC 0.880±0.051; p = 0.087; fig. 3b). In order to refine risk estimation in a clinically feasible fashion, we designed a two-dimensional diagram for risk stratification in VAP (fig. 4). In this nomogram, MR-proANP and SAPS II assessed at VAP onset predict the risk of death within the following 28 days. PCT did not provide useful additional information.
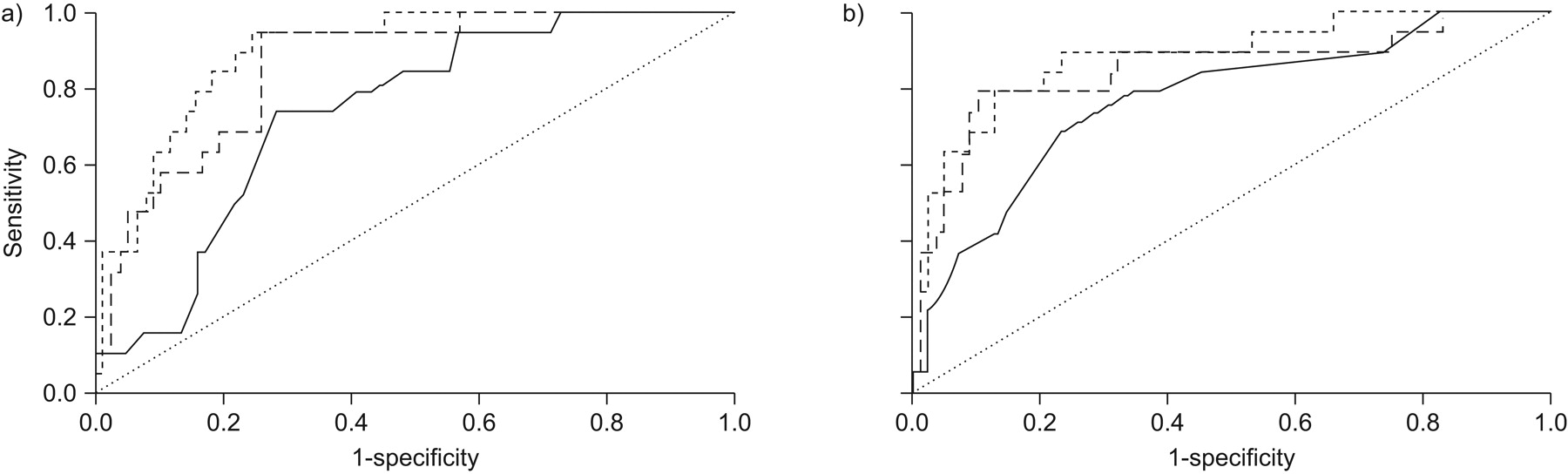
Receiver operating characteristic curves showing a stepwise improvement of a) Simplified Acute Physiologic Score (SAPS) II (—: SAPS II, area under the curve (AUC) 0.736; – – –: SAPS II plus midregicnal pro-atrial natriuretic peptide (MR-proANP), AUC 0.859; -----: SAPS II plus MR-proANP plus procalcitonin (PCT), AUC 0.895) and b) Sequential Related Organ Failure Assessment (SOFA) (—: SOFA, AUC 0.768; – – –: SOFA plus MR-proANP, AUC 0.848; ---: SOFA plus MR-proANP plus PCT, AUC 0.880) by adding MR-proANP and PCT.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
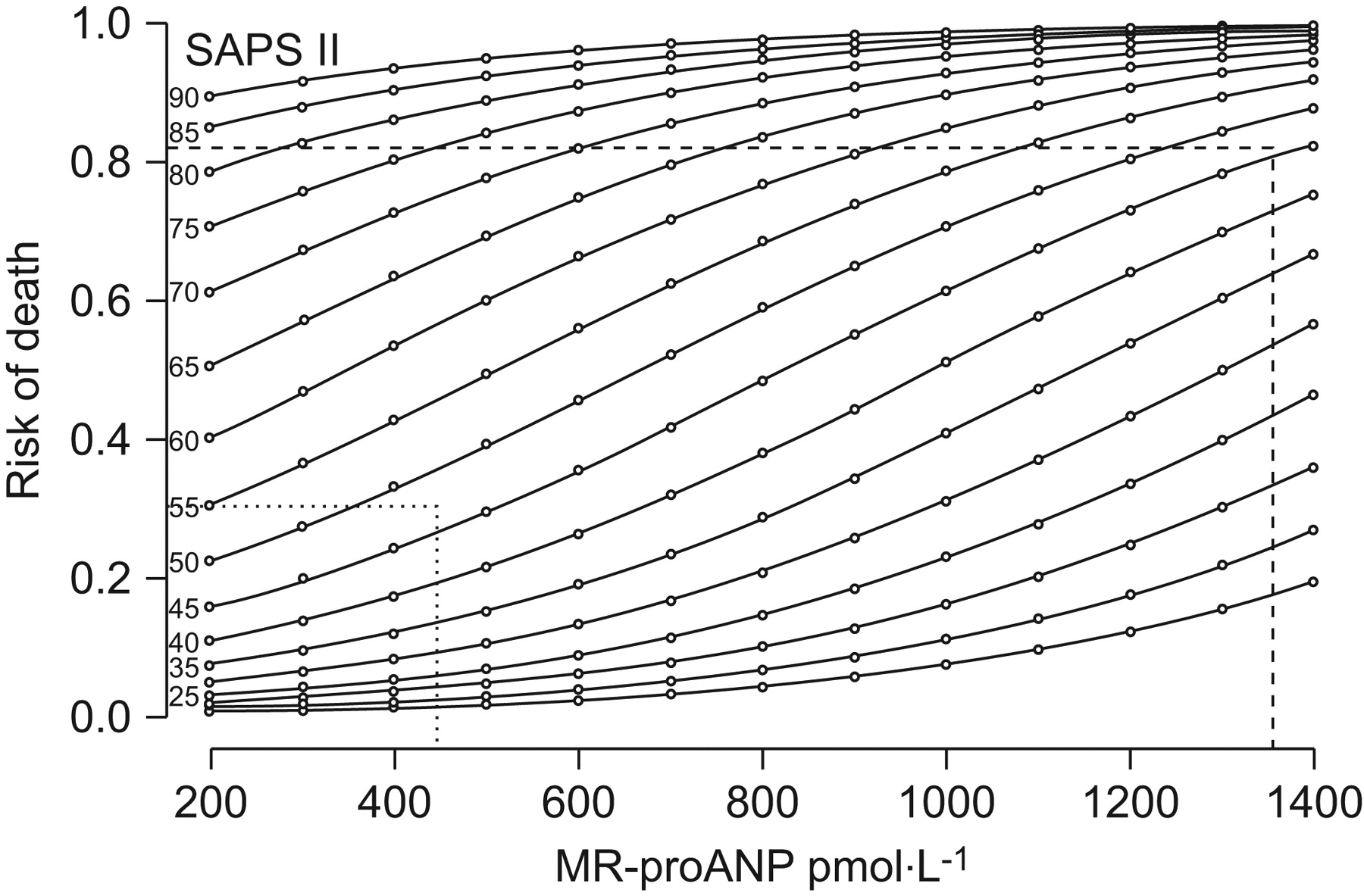
Nomogram to estimate survival, combining Simplified Acute Physiologic Score (SAPS) II and midregicnal pro-atrial natriuretic peptide (MR-proANP) assessed at ventilator-associated pneumonia (VAP) onset. MR-proANP adds prognostic information mainly in the group of intermediate SAPS II. Two patients with an identical SAPS II (47 points) are shown. The first patient (survivor; ···), with a MR-proANP level of 449 pmol·L−1 at VAP onset, had an estimated risk of death around 30%; the second patient (nonsurvivor; -----), with a MR-proANP level of 1,360 pmol·L−1, had a risk >80%.
The predictive values of MR-proANP, PCT and clinical scores were also analysed in the subgroup of patients with microbiologically confirmed VAP (n = 74). Compared with patients with clinically diagnosed VAP, the AUC for PCT at VAP onset to predict mortality within 28 days was higher in patients with microbiologically diagnosed VAP (mean±se AUC 0.767±0.065 versus 0.712±0.065). In contrast, the predictive property of MR-proANP at VAP onset was similar in both populations (AUC 0.820±0.060 versus 0.801±0.060). Combining MR-proANP with SOFA or SAPS II enhanced AUC values compared with the single score (SOFA AUC 0.848±0.056, p = 0.071; SAPS II AUC 0.906±0.046, p = 0.019). The conjunction of MR-proANP, PCT and SOFA at VAP onset predicted survival with a significantly better accuracy compared with the SOFA score (AUC 0.900±0.047; p = 0.032).
DISCUSSION
We report three main findings. First, circulating MR-proANP and PCT levels at VAP onset are significantly elevated in nonsurvivors compared with survivors. Secondly, a single MR-proANP determination at VAP onset is a suitable marker for survival prediction. Finally, the combination of MR-proANP and PCT improves survival prediction of SAPS II and SOFA, two well established ICU scores.
Circulating natriuretic peptides, such as ANP and brain natriuretic peptide, are primarily of cardiac origin. They were mainly established for diagnostic purposes in congestive heart failure but have also been evaluated for prediction and treatment guidance 29–31. Recently, their diagnostic use in the ICU has been challenged 32. However, natriuretic peptides have gained relevance beyond cardiac disease. In intensive care, natriuretic peptides were repeatedly suggested to predict survival 15, 33–35.
Elevated ANP levels have been reported in lower respiratory tract infections, sepsis and other pulmonary diseases 12–14, 36–38. In VAP, we found elevated MR-proANP to be associated with cardiac, renal and pulmonary comorbidities. Congestive heart failure results in increased left cardiac pressures and volume overload. Similarly, acute pulmonary disease leads to transient pulmonary hypertension resulting in right heart strain 39. Both represent major stimuli for ANP release. Renal failure elevates proANP levels, most probably due to an inappropriate renal clearance 40. Therefore, the associated underlying comorbidities in VAP lead to increased MR-proANP levels and represent an additional risk for death. VAP itself represents another ANP-releasing stimulus. Accordingly, it was suggested that the lung may possess its own “ANP system”, rather than being dependent on the circulating ANP 41. Moreover, lymphoid organs have been suggested to secrete ANP 42, 43. Recently, elevated tumour necrosis factor (TNF)-α was associated with increased ANP independently of left ventricular function 44. This indicates that TNF-α might exert direct cardiotoxic effects or stimulate ANP release. Therefore, it is tempting to hypothesise that in inflammatory conditions such as VAP, ANP secretion is partially mediated through cytokine release.
We have shown that MR-proANP is elevated in nonsurvivors and that the slope of decline differs significantly between survivors and nonsurvivors in VAP. Our results are consistent with the findings reported by Seligman et al. 15 suggesting MR-proANP to be associated with mortality and the severity of sepsis in a VAP cohort. Notably, that study has restricted the analysis to VAP patients presenting a clinical pulmonary infection score above six on day 3 and analysed proANP levels only at two time-points (day 0 and 4). In our cohort, MR-proANP levels were persistently increased over the 10 days following VAP onset in nonsurvivors. We report a similar mortality prediction of proANP in VAP compared with Berdal et al. 35, who assessed 70 unselected mechanically ventilated, critically ill patients. Thus, MR-proANP seems to reflect multiple comorbidities and infectious conditions related to survival in intensive care. Despite the exceptionally high mortality and resource utilisation in VAP, specific tools assessing mortality are scarce 45. Herein, we propose a MR-proANP cut-off (660 pmol·L−1) to identify patients at an extremely high risk for death.
PCT first emerged as a diagnostic and prognostic marker of bacterial infection. Recently, several interventional trials showed PCT was beneficial for guiding therapy in lower respiratory tract infections, including VAP 24, 46–49. PCT at VAP onset presented an AUC of 0.712 for predicting survival in our population. AUC values were slightly better on day 3 and 5 after VAP onset (data not shown) However, since parameters assessed at VAP onset are statistically more robust and clinically more relevant we focused on the very first day. Nonetheless, our figures are lower than those described by others 20, 21, 50. Duflo et al. 20 reported an AUC of 0.79 using PCT for predicting VAP-associated mortality. However, all patients included in their study met three out of three diagnostic parameters. Additionally, only microbiologically diagnosed VAP cases were analysed. Therefore, a great proportion of patients meeting fewer diagnostic criteria for VAP might have been missed. Moreover, the selection of cases with severe bacterial infection might have lead to an overestimation of the PCT performance. Restricting the population to microbiologically confirmed cases of VAP has also increased the predictive property of PCT in our study. However, patient numbers were too small to stratify microbiologically confirmed and unconfirmed cases. It has been proposed that PCT kinetics levels might predict survival in VAP and critical ill patients 22, 23. Consistent with those findings, we report a different decline of PCT levels in survivors and nonsurvivors. Luyt et al. 21 suggested PCT to be strongly related to unfavourable outcome in VAP. The superiority of PCT in the previous study might be explained by more restrictive inclusion criteria and the use of a combined end-point. Nevertheless, the clinical significance of a combined end-point including death, VAP recurrence and extrapulmonary infection is greatly diverse. In our trial, we used death as the sole clinical end-point. The findings show that PCT is a predictor of survival in VAP. However, its value is limited and it is unlikely that PCT sufficiently predicts survival. Therefore, we do not support a single PCT measurement for risk assessment in VAP.
Disease-specific scores, ranging from the Apgar score to the Mini-Mental State Examination, have been verified over decades and remain cornerstones for guiding therapy. In intensive care, due to multiple organ dysfunction, nondisease-specific scores are probably more suitable to assess mortality. SAPS II and SOFA are two of the most widespread ICU scoring systems. They are powerful tools for quantifying disease severity and estimating mortality 51–54. Nevertheless, most studies investigating ICU scores were performed to describe the outcome of a patient group as a whole. Thus, the value in an individual patient may be limited 55, 56. In our study, we showed that both SAPS II and SOFA can successfully predict the outcome of individual VAP patients. However, a single MR-proANP measurement had a similar value for predicting survival as scores composed of six (SOFA) or 15 (SAPS II) parameters, including another sub-score (Glasgow Coma Scale). Therefore, MR-proANP is potentially superior to every one of the 18 parameters included in SOFA and SAPS II. In this context, this is the first study to report that adding biomarkers stepwise improves the performance of clinical scores for survival prediction in VAP. Out of 25 parameters included in our L1-penalised model, MR-proANP was identified as the most important variable, followed by SOFA and SAPS II.
PCT was clearly inferior to MR-proANP, and its additional contribution to ICU scores and MR-proANP was small. However, both PCT and MR-proANP were able to improve ICU scores, independently. Together, they might comprise a wide spectrum of disease in VAP and intensive care. Thus, we suggest circulating biomarkers, such as MR-proANP and PCT, to be complementary to ICU scores, such as SAPS II and SOFA.
Practicability and time efficiency are important requirements for critical care measures. Based on our data, we have suggested an easily applicable nomogram combining MR-proANP and SAPS for survival prediction. Especially in patients with moderately elevated SAPS II scores, the additional determination of MR-proANP markedly improves risk stratification. Prompt risk stratification has been shown to influence patient management, decrease costs and potentially improve clinical outcome 57–60. However, clinical impact and costs, particularly with regard to new biomarkers, need to be addressed in future studies.
Our study has several limitations. First, the small sample size may influence discrimination. Thus, our results need to be considered hypothesis-generating and larger prospective trials are essential to validate the findings of this pilot study. Secondly, the clinical diagnostic criteria for VAP remain a subject of debate. For this reason, we provide results for both clinically and microbiologically diagnosed VAP. Thirdly, cardiac function certainly affects MR-proANP release and survival. Therefore, interaction and/or confounding are likely. In a restricted population (patients with echocardiography), neither patients with systolic nor those with diastolic dysfunction were at increased risk for death (data not shown). Nevertheless, when analysing the restricted population, MR-proANP was a strong predictor of survival. Finally, in contrast to SOFA, the use of SAPS II after ICU admission has not been evaluated. Nonetheless, a reassessment of disease severity at the moment of VAP diagnosis is considered to allow a better and more precise stratification of risk and prediction of mortality 45, 61.
In summary, the combination of MR-proANP and PCT improves the diagnostic performance of SAPS II and SOFA in VAP survival. By complementing, rather than replacing, clinical judgements, the combination of prognostic scores and biomarkers represent a new and promising approach for risk stratification in VAP.
Acknowledgments
We thank A. Meyer (Clinic of Pulmonary Medicine and Respiratory Cell Research, University Hospital, Basel, Switzerland), S. Heard, J. Longtine and K. Longtine (all Division of Anesthesiology, UMass Memorial Medical Center, Worcester, MA, USA) for data supply and most helpful support during the study and A. Schötzau (Schötzau & Simmen Statistical Consulting, Basel) for statistical advice.
Footnotes
For editorial comments see page 486.
Support Statement
D. Stolz was supported by grants from the Swiss National Foundation (PP00P3_128412/1), the Liechtenstein Foundation and the “Freiwillige Akademische Gesellschaft Basel”. N. Thakkar was supported by the Will Rogers Foundation. Additional funding was granted by the Clinic of Pulmonary Medicine, University Hospital Basel, Basel, Switzerland.
Clinical Trial
This study was registered in the Current Controlled Trials Database as “ProVAP”-Study (identifier number ISRCTN61015974).
Statement of Interest
Statements of interest for D. Stolz and the study itself can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received February 11, 2010.
- Accepted May 25, 2010.
- ©ERS 2011
REFERENCES










