





Figures
- Fig. 1—
Flow chart showing the study selection. RCTs: randomised controlled trials; ICS: inhaled corticosteroids; COPD: chronic obstructive pulmonary disease; CV: cardiovascular.
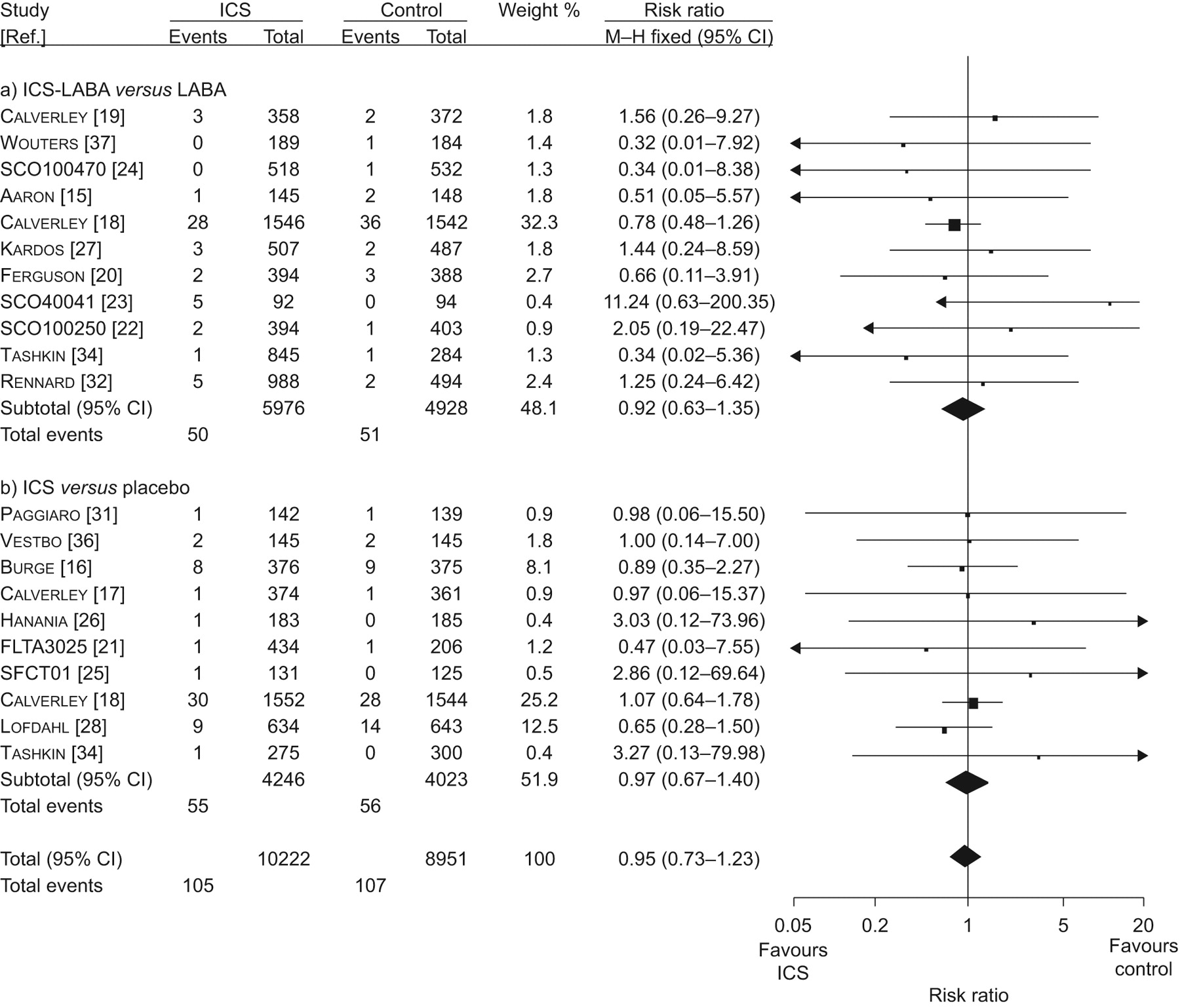
- Fig. 2—
Meta-analysis of randomised controlled trials of inhaled corticosteroids (ICS) versus controls for myocardial infarction. a) ICS-long acting β2-agonists (LABA) versus LABA and b) ICS versus placebo. a) Chi-squared = 6.16; degrees of freedom (df) = 10 (p = 0.80); I2 = 0%. Test for overall effect: z = 0.43 (p<0.67). b) Chi-squared = 2.79; df = 9 (p = 0.97); I2 = 0%. Test for overall effect: z = 0.16 (p<0.87). Overall: Chi-squared = 9.06; df = 20 (p = 0.98); I2 = 0%. Test for overall effect: z = 0.41 (p<0.68). M–H: Mantel–Haenszel.
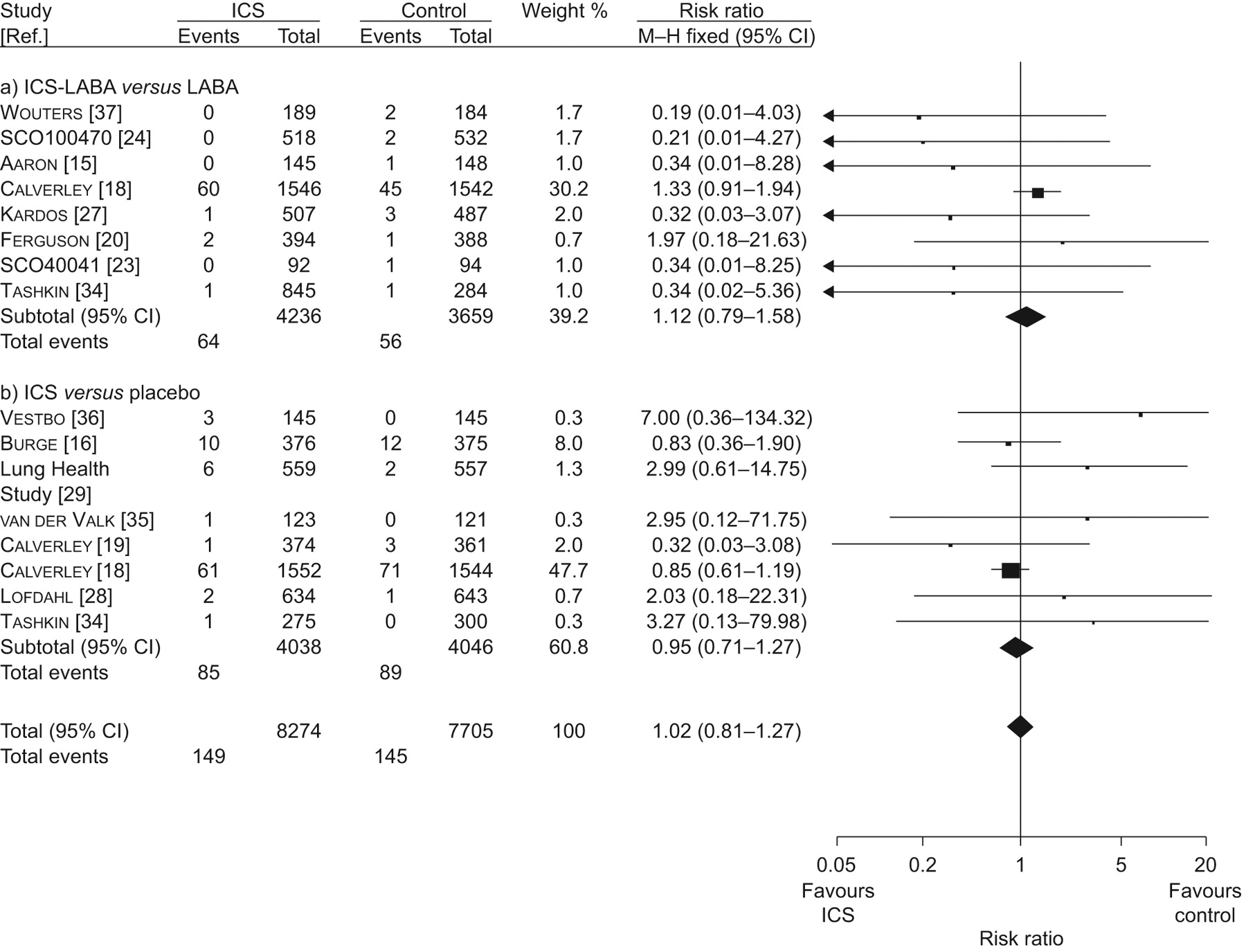
- Fig. 3—
Meta-analysis of randomised controlled trials of inhaled corticosteroids (ICS) versus controls for cardiovascular death. a) ICS-long acting β2-agonists (LABA) versus LABA and b) ICS versus placebo. a) Chi-squared = 6.46; degrees of freedom (df) = 7 (p = 0.49); I2 = 0%. Test for overall effect: z = 0.62 (p<0.53). b) Chi-squared = 6.55; df = 7 (p = 0.48); I2 = 0%. Test for overall effect: z = 0.33 (p<0.74). Overall: Chi-squared = 13.85; df = 15 (p = 0.54); I2 = 0%. Test for overall effect: z = 0.14 (p<0.89). M–H: Mantel–Haenszel.
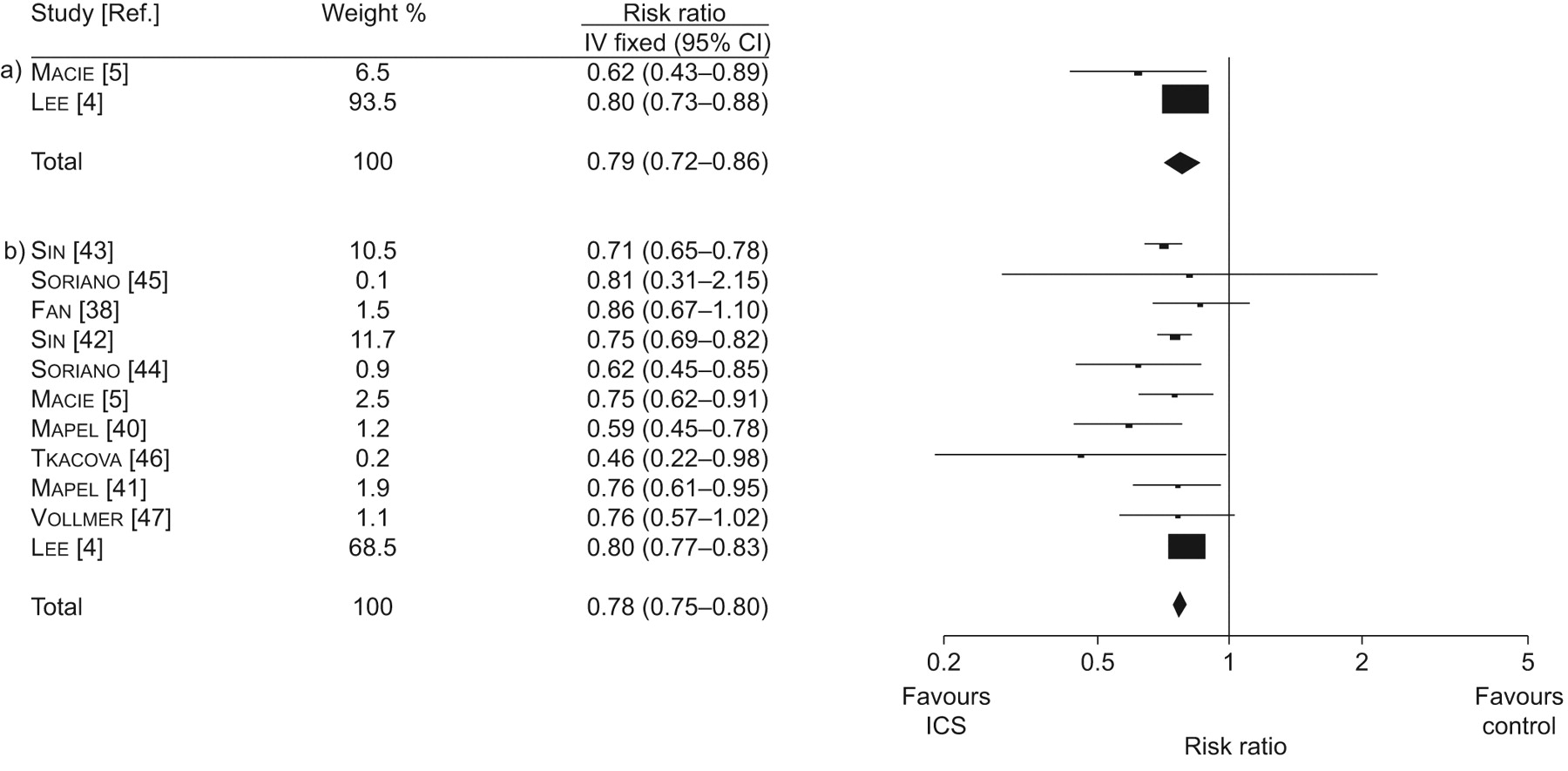
- Fig. 4—
Meta-analysis of inhaled corticosteroids (ICS) versus controls for a) cardiovascular death and b) overall mortality in observational studies. a) Chi-squared = 1.79; degrees of freedom (df) = 1 (p = 0.18); I2 = 44%. Test for overall effect: z = 5.10 (p<0.00001). b) Chi-squared = 14.95; df = 10 (p = 0.13); I2 = 33%. Test for overall effect: z = 16.22 (p<0.00001). IV: inverse variance.
- Fig. 5—
Funnel plots of risk ratios for overall mortality in the a) trials and b) observational studies. ▪: inhaled corticosteroid (ICS) long acting β2-agonists (LABA) versus LABA; •: ICS versus placebo.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1—
Characteristics of randomised controlled trials included in the analysis of cardiovascular(CV) events and mortality
Study [Ref.] Location Treatment duration weeks COPD criteria Primary outcome Concomitant cardiac conditions and exclusions Drug Male Age yrs FEV1 % pred Prior ICS use Current smokers Aaron 15# 27 centres in Canada 52 FEV1/FVC <70% COPD exacerbation HTN: 41.4 %; CAD: 22.8%; CHF: 3.5% Salmeterol/fluticasone combination 50/500 μg b.i.d. 57.9 67.5±8.9 39.4±11.9 70.8 32.4 HTN: 43.9%; CAD: 21.0%; CHF: 1.4% Excluded CHF with LV dysfunction Salmeterol xinafoate 50 μg 57.4 67.6±8.2 38.0±13.1 78.8 24.3 Burge 16 18 UK hospitals 156 FEV1/FVC <70% Decline in FEV1 NA Fluticasone propionate 500 μg b.i.d. 75 63.7±7.1 50.3±14.9 51.1 36.4 Placebo 74.2 63.8±7.1 50.0±14.9 57.0 39.2 Calverley 17 196 centres in 25 countries 52 ERS FEV1 NA Salmeterol/fluticasone combination 50/500 μg b.i.d. 75 62.7±8.7 44.8±14.7 50 52 Salmeterol xinafoate 50 μg b.i.d. 70 63.2±8.6 44.3±13.8 49 51 Fluticasone propionate 500 μg b.i.d. 70 63.5±8.5 45±13.6 54 53 Placebo 75 63.4±8.6 44.2±13.7 52 47 Calverley 19 109 centres in 15 countries 52 GOLD FEV1 and HRQoL NA Formoterol 9 μg/budesonide 400 μg b.i.d. 78 64±NA 36±10 47 33 Excluded any CV disorder Formoterol 9 μg b.i.d. 75 63±NA 36±10 48 36 Budesonide 400 μg b.i.d. 74 64±NA 36±10 51 39 Placebo 75 65±NA 36±10 46 30 Calverley 18 44 centres in 42 countries 156 ERS Mortality NA Salmeterol/fluticasone combination 50/500 μg b.i.d. 75 65±8.3 44.3±12.3 47 43 Salmeterol xinafoate 50 μg 76 65.1±8.2 43.6±12.6 45 43 Fluticasone propionate 500 μg b.i.d. 75 65±8.4 44.1±12.3 47 43 Placebo 76 65±8.2 44.1±12.3 51 43 Ferguson 20 94 centres in North America 52 ATS Rate of exacerbations NA Salmeterol/fluticasone combination 50/250 μg b.i.d. 58.3 64.9±9.0 39.8±13.9 15 40 Salmeterol xinafoate 50 μg b.i.d. 52.0 65.0±9.1 50.6±15.4 18 38 FLTA3025 21 55 centres in the USA 24 ATS FEV1 NA Fluticasone propionate 500 μg b.i.d. 66 63.3±10 1301±500+ NA NA Fluticasone propionate 250 μg b.i.d. 72 65.2±8.7 1240±486+ NA NA Placebo 70 64.8±9.5 1221±502+ NA NA Hanania 26 76 centres in the USA 24 ATS FEV1 Excluded abnormal ECG Salmeterol/fluticasone combination 50/250 μg b.i.d. 61 63±NA 41±11 23 43 Salmeterol xinafoate 50 μg b.i.d. 58 64±NA 42±12 20 51 Fluticasone propionate 250 μg b.i.d. 66 63±NA 42±11 28 48 Placebo 58 65±NA 42±12 30 47 Kardos 27 95 centres in Germany 52 GOLD COPD exacerbations NA Salmeterol/fluticasone combination 50/500 μg b.i.d. 74 63.8±8.3 40.4±8.9 40.6 49.7 Salmeterol xinafoate 50 μg b.i.d. 77.6 64±8.2 40.3±8.5 44.4 49.9 Lung Health Study 29 10 centres 160 FEV1/FVC <70 % Rate of decline in FEV1 Excluded recent MI Triamcinolone 600 μg b.i.d. 64 56.2±6.8 64.9±13.5 NA 90.5 Placebo 62.1 56.4±6.8 63.4±13.2 NA 89.8 Lofdahl 28 39 centres in 9 EU countries 156 FEV1/FVC <70 % Rate of decline in FEV1 32 (15 on budesonide, 15 on placebo with previous ischaemic cardiac events) Budesonide 400 μg b.i.d. 73.5 52.5±7.5 76.8±12.4 NA 39.4 pack-yrs Placebo 72.2 52.4±7.7 76.9±13.2 NA 39.2 pack-yrs Mahler 30 Multicentre trial in the USA 24 ATS FEV1 and TDI NA Salmeterol/fluticasone combination 50/500 μg b.i.d. 62 61.9±NA 41±NA 28 46 Salmeterol xinafoate 50 μg b.i.d. 64 63.5±NA 40±NA 31 46 Fluticasone propionate 500 μg b.i.d. 61 64.4±NA 41±NA 25 46 Placebo 75 64±NA 41±NA 18 54 Paggiaro 31 13 European centres 24 ERS Exacerbations NA Fluticasone propionate 500 μg b.i.d. 99 62±NA 59±18 NA 49 Placebo 78 64±NA 55±17 NA 49 Rennard 32 237 centres in 9 countries 52 FEV1/FVC <70% FEV1 HTN 41.6% Budesonide 160/ formoterol 4.5 μg b.i.d. 62.3 63.2±8.9 33.8±11.4 NA 34.8 Cardiac disease 17.7% Budesonide 80/ formoterol 4.5 μg b.i.d. 62.8 63.6±9.2 34.5±11.5 NA 37.0 Cardiac failure 2.9% Formoterol 4.5 μg b.i.d. 65.3 62.9±9.1 33.7±11.2 NA 41.2 Placebo 65.3 62.9±9.1 35.5±11.9 NA 39.5 SCO100250 22 98 centres in the USA and Canada 52 FEV1/FVC <70% Rate of exacerbations NA Salmeterol/fluticasone combination 50/250 μg b.i.d. 51 65.4±NA <50§ NA NA Salmeterol xinafoate 50 μg b.i.d. 57 65.3±NA <50§ NA NA SCO100470 24 135 centres in Europe and Asia-Pacific 24 GOLD FEV1 and TDI score NA Salmeterol/fluticasone combination 50/250 μg b.i.d. 78.3 63.5±9.3 1654±459+ NA 42 Salmeterol xinafoate 50 μg b.i.d. 77.2 63.7±9.0 1681±465+ NA 44 SCO40041 23 31 centres in the USA 156 GOLD Bone mineral density NA Salmeterol/fluticasone combination 50/250 μg b.i.d. 59.7 65.4±8.36 <70% NA NA Salmeterol xinafoate 50 μg b.i.d. 62.7 65.9±9.52 <70% NA NA SFCT01/SCO30002 25¶ 49 centres in Italy and Poland 52 FEV1/VC <88% Time to exacerbations NA Fluticasone propionate 500 μg b.i.d. 83.9 64.6±8.7 NA NA NA Placebo 80 65.7±9.0 NA NA NA Szafranski 33 89 centres in 11 countries 52 GOLD Number of severe exacerbations and FEV1 NA Budesonide/formoterol 160/4.5 μg 2 inhalations b.i.d. 76 64±NA 36±NA 26 30 Excluded if relevant CV disorder For 4.5 μg 2 inhalations b.i.d. 76 63±NA 36±NA 28 38 Budesonide 200 μg 2 inhalations b.i.d. 80 64±NA 37±NA 24 36 Placebo 83 65±NA 36±NA 26 34 Tashkin 34 194 sites in 5 countries 26 FEV1/FVC <70% FEV1 NA Budesonide 320/ formoterol 9 μg b.i.d. 67.9 63±NA 33.7±11.8 NA 40.8 Budesonide 160/ formoterol 9 μg 64.4 63±NA 34.1±10.9 NA 39.5 Budesonide 160 μg + formoterol 4.5 μg 74.2 64±NA 33.5±10.7 NA 37.3 Budesonide 160 μg 67.6 63±NA 33.5±10.8 NA 40.0 Formoterol 4.5 μg 65.5 64±NA 33.6±11.3 NA 38.4 Placebo 69.0 63±NA 34.6±10.5 NA 36.0 van der Valk 35 Pulmonary clinics 26 ATS Exacerbations and HRQoL Cardiac insufficiency excluded Fluticasone propionate 500 μg b.i.d. 85.4 64.1±6.8 57.5±14.1 86.2 22.0 Placebo 83.5 64±6.7 56.1±14.8 80.2 33.0 Vestbo 36 Community in Denmark 156 FEV1/VC<70% Rate of FEV1 decline NA Budesonide 400 μg b.i.d. 58.6 59.0±8.3 86.2±20.6 NA 75.9 Placebo 62.1 59.1±9.7 86.9±21.1 NA 77.2 Wouters 37 39 centres in the Netherlands 52 FEV1/VC <88% Rate of FEV1 decline Excluded if they had MI, angina or heart failure 3 months prior to entry Salmeterol/fluticasone combination 50/500 μg b.i.d. 73 63±7.9 47.4±13.9 85 39 Salmeterol xinafoate 50 μg b.i.d. 75 64±7.7 48.2±12.9 87 35 Data are presented as % or mean±sd, unless otherwise stated. COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 s; % pred: % predicted; ICS: inhaled corticosteroid; FVC: forced vital capacity; HTN: hypertension; CAD: coronary artery disease; CHF: chronic heart failure; LV: left ventricle; NA: not available; ERS: European Respiratory Society; GOLD: Global Initiative for Chronic Obstructive Lung Disease; HRQoL: health-related quality of life; ATS; American Thoracic Society; EU: European Union; ECG: electrocardiogram; MI: myocardial infarction; TDI: transitional dyspnoea index; VC: vital capacity. #: treatment with tiotropium bromide 18 μg·day−1 in both arms and an additional tiotropium arm; ¶: also had an additional salmeterol/fluticasone combination arm; +: reported in mL as % pred; §: FEV1 <50% pred, exact mean and sd data were unavailable.
- Table 2—
Risk of bias assessment of included randomised controlled trials of inhaled corticosteroids in chronic obstructive pulmonary disease(COPD)#
Study [Ref.] Sequence generation Allocation concealment AE monitoring Drug Withdrawal rates Lost to follow-up Aaron 15 Adequate, central allocation Adequate AE captured by monthly telephone questionnaire and checklist Salmeterol/fluticasone combination = 145 15 (10.3) 2 (1.3) Salmeterol xinafoate = 148 20 (13.5) 2 (1.3) Burge 16 Adequate, computer generated, stratified by centre Adequate AEs and SAEs recorded throughout the study Fluticasone propionate = 372 160 (43.0) 16 (4.3) Placebo = 370 195 (52.7) 18 (4.9) Calverley 17 Adequate, computer generated Adequate AE or SAE occurring during therapy Salmeterol/fluticasone combination = 358 89 (24.9) 8 (2.2) Salmeterol xinafoate = 372 119 (32.0) 8 (2.2) Fluticasone propionate = 374 108 (29.0) 8 (2.1) Placebo = 361 140 (38.8) 6 (1.7) Calverley 19 Unclear Unclear AEs recorded at 1, 2, 3, 6, 9 and 12 months of treatment Formoterol/budesonide = 254 74 (29) 4 (1.6) Formoterol = 255 111 (44) 4 (1.6) Budesonide = 257 102 (40) 4 (1.6) Placebo = 256 106 (41) 6 (2.3) Calverley 18 Adequate, schedule central allocation Adequate AEs reviewed at each visit Salmeterol/fluticasone combination = 1533 522 (34.1) 29 (1.9) Salmeterol xinafoate = 1521 561 (36.9) 15 (1.0) Fluticasone propionate = 1534 587 (38.3) 24 (1.6) Placebo = 1524 673 (44.2) 21 (1.4) Ferguson 20 Unclear Unclear AE collected at start and end Salmeterol/fluticasone combination = 394 117 (29.7) 10 (2.5) Salmeterol xinafoate = 388 149 (38.4) 10 (2.6) FLTA3025 21 Unclear Unclear AEs and SAEs recorded at each visit Fluticasone propionate = 434 147 (33.9) NA Placebo = 206 79 (38.3) NA Hanania 26 Unclear Unclear AE reporting at each visit Salmeterol/fluticasone combination = 178 53 (30) NA Salmeterol xinafoate = 177 57 (32) NA Fluticasone propionate = 183 49 (27) NA Placebo = 185 59 (32) NA Kardos 27 Adequate, centrally generated block Adequate AEs and SAEs recorded during run in and follow-up Salmeterol/fluticasone combination = 507 99 (19.5) 4 (0.8) Salmeterol xinafoate = 487 103 (21.1) 3 (0.6) Lofdahl 28 Unclear Unclear Angina pectoris, MI, CAD and myocardial ischaemia reported as AE and SAE Budesonide = 634 176 (27.7) NA Placebo = 643 189 (29.4) NA Lung Health Study 29 Unclear Unclear AEs every 3 months Triamcinolone = 559 28 (5.0) NA Reviewed deaths to determine cause of death Placebo = 557 38 (6.8) NA Mahler 30 Unclear Unclear AEs and SAEs documented Salmeterol/fluticasone combination = 165 52 (31.5) NA Salmeterol xinafoate = 160 45 (28.2) NA Fluticasone propionate = 168 68 (40.5) NA Placebo = 181 69 (38.1) NA Paggiaro 31 Adequate, computer generated Adequate AE defined as untoward medical occurrence during treatment Fluticasone propionate = 142 19 (13.3) 0 Placebo = 139 27 (19.4) 2 (1.4) Rennard 32 Unclear Unclear AEs, vital signs and ECGs at study visit Budesonide 320 μg/formoterol 9 μg b.i.d. = 494 134 (27.1) 9 (1.8) Budesonide 160μg/formoterol 9 μg b.i.d. = 494 143 (28.9) 12 (2.4) Formoterol = 495 157 (31.7) 12 (2.4) Placebo = 481 175 (36.3) 13 (2.7) SCO100250 22 Unclear Unclear AEs and SAEs recorded after study medication but no later than last date after study medication Salmeterol/fluticasone combination = 394 125 (31.7) NA Salmeterol xinafoate = 403 156 (38.7) NA SCO100470 24 Unclear Unclear AEs and SAEs recorded at each study visit Salmeterol/fluticasone combination = 518 59 (11.4) NA Salmeterol xinafoate = 532 74 (13.9) NA SCO40041 23 Unclear Unclear On therapy AEs and SAEs monitored Salmeterol/fluticasone combination = 92 36 (39.1) NA Salmeterol xinafoate = 94 39 (41.5) NA SFCT01/SCO30002 25 Unclear Unclear All AEs occurring after subject consented to participate until end of follow-up Fluticasone propionate = 131 34 (26.0) NA Placebo = 125 40 (32.0) NA Szafranski 33 Unclear Unclear AEs detected at visits 2–8, with ECGs at visits 1, 6 and 8 Budesonide/formoterol = 208 59 (28) NA Formoterol = 201 64 (32) NA Budesonide = 198 62 (31) NA Placebo = 205 90 (44) NA Tashkin 34 Unclear Unclear AEs, vital signs and ECGs at study visit Budesonide 160 μg/formoterol 4.5 μg b.i.d. = 277 NA NA Budesonide/formoterol = 281 NA NA Budesonide + formoterol = 287 NA NA Budesonide = 275 NA NA Formoterol = 284 NA NA Placebo = 300 NA NA van der Valk 35 Adequate, permuted blocks, stratified Adequate 3- and 6-month follow-up Fluticasone propionate = 123 1 (0.8) 0 Placebo = 121 1 (0.8) 0 Vestbo 36 Adequate, computer generated Adequate Participants seen every 3 months Budesonide = 145 36 (24.8) 0 Placebo = 145 51 (35.2) 0 Wouters 37 Adequate Adequate AE collected at start and end of treatment Salmeterol/fluticasone combination = 189 34 (18.0) 0 Salmeterol xinafoate = 184 46 (25.0) 0 Data are presented as n or n (%). AE: adverse event; SAE: serious adverse event; NA: not available; MI: myocardial infarction; CAD: coronary artery disease; ECG: electrocardiogram. #: all randomised controlled trials were double blinded.
- Table 3—
Cardiovascular(CV) events and all-cause mortality in randomised controlled trials of inhaled corticosteroids in chronic obstructive pulmonary disease
Study [Ref.] Intervention Total participants Participants MI CV death Overall mortality Aaron 15# Salmeterol/fluticasone combination 145 1 0 6 Salmeterol xinafoate 148 2 1 6 Placebo 156 2 1 4 Burge 16¶ Fluticasone propionate 376 8 10 32 Placebo 375 9 12 36 Calverley 17¶ Salmeterol/fluticasone combination 358 3 0 2 Salmeterol xinafoate 372 2 0 3 Fluticasone propionate 374 1 1 3 Placebo 361 1 3 7 Calverley 19 Formoterol/budesonide 254 NA NA 5 Formoterol 255 NA NA 13 Budesonide 257 NA NA 6 Placebo 256 NA NA 5 Calverley 18¶,+ Salmeterol/fluticasone combination 1546 28 60 193 Salmeterol xinafoate 1542 36 45 205 Fluticasone propionate 1552 30 61 246 Placebo 1544 28 71 231 Ferguson 20¶ Salmeterol/fluticasone combination 394 2 2 6 Salmeterol xinafoate 388 3 1 3 FLTA3025 21¶ Fluticasone propionate 434 1 0 0 Placebo 206 1 0 0 Hanania 26¶ Salmeterol/fluticasone combination 178 0 0 0 Salmeterol xinafoate 177 0 0 0 Fluticasone propionate 183 1 0 0 Placebo 185 0 0 0 Kardos 27¶ Salmeterol/fluticasone combination 507 3 1 7 Salmeterol xinafoate 487 2 3 9 Lung Health Study 29 Triamcinolone 559 NA 6 15 Placebo 557 NA 2 19 Lofdahl 28 Budesonide 634 9 2 8 Placebo 643 14 1 10 Mahler 30¶ Salmeterol/fluticasone combination 165 0 0 0 Salmeterol xinafoate 160 0 0 0 Fluticasone propionate 168 0 0 0 Placebo 181 0 0 3 Paggiaro 31¶ Fluticasone propionate 142 1 0 0 Placebo 139 1 0 2 Rennard 32 Budesonide/formoterol 988 5 NA 9 Formeterol 495 2 NA 2 Placebo 481 1 NA 4 SCO100250 22¶ Salmeterol/fluticasone combination 394 2 0 4 Salmeterol xinafoate 403 1 0 6 SCO100470 24¶ Salmeterol/fluticasone combination 518 0 0 3 Salmeterol xinafoate 532 1 2 3 SCO40041 23¶ Salmeterol/fluticasone combination 92 5 0 5 Salmeterol xinafoate 94 0 1 7 SFCT01/SCO30002 25¶ Fluticasone propionate 131 1 0 0 Placebo 125 0 0 0 Szafranski 33 Formoterol/budesonide 208 NA NA 6 Formoterol 201 NA NA 6 Budesonide 198 NA NA 5 Placebo 205 NA NA 9 Tashkin 34 Budesonide/formoterol 845 1 1 7 Formoterol 284 1 1 1 Budesonide 275 1 1 2 Placebo 300 0 0 1 van der Valk 35¶ Fluticasone propionate 123 0 1 4 Placebo 121 0 0 0 Vestbo 36 Budesonide 145 2 3 4 Placebo 145 2 0 5 Wouters 37¶ Salmeterol/fluticasone combination 189 0 0 2 Salmeterol xinafoate 184 1 2 4 Data are presented as n. MI: myocardial infarction; NA: not available. #: reported as serious adverse event of MI or acute arrhythmia; ¶: CV adverse event data extracted from manufacturers clinical trials register; +; CV mortality data extracted from regulatory agencies as unavailable in publications.
- Table 4—
Characteristics of observational studies of inhaled corticosteroids(ICS) and cardiovascular (CV) events or mortality
Study [Ref.] Participants Design Data source Duration weeks Participants included ICS exposure Ascertainment of ICS exposure Outcomes Outcome ascertainment Risk estimates ICS (versus controls) with outcomes Bias and limitations Fan 38 2654 ICS users, 5398 non-users PC US VA DB 78 1. Outpatient visit or hospitalisation with ICD-9 diagnosis of COPD.2. Using at least one pulmonary prescription during 90 days before index visit.3. Age >45 yrs.4. Participant in the ACQUIP RCT for ≥1 yr. Becl (44%), triam (45%), fluni (6%), flu (5%) Prescription for inhalers, subdivided by 90-day exposure periods.“User” if prescription filled for >80% of each 90 days. Death Records date of death for veterans whose families file for the benefit. HR of death ICS versus controls.Low dose (HR 0.96; 95% CI 0.69–1.33); medium/high doses (HR 0.86; 95% CI 0.67–1.10)Adjusted for distance from hospital, pulmonary prescriptions, prior hospitalisations, comorbidity. Significant baseline differences in age, marital status, race, comorbidity, COPD clinic visits and hospitalisations, respiratory prescription use.Assumes VA system provides records on all prescriptions and patients compliant.No ascertainment of death by checking, DB known to identify 98.8% of deaths among Medicare-eligible patients. Huiart 39 371 cases, 1864 controls Nested CC Canadian Health Insurance DB in Saskatchewan 130 New patients with COPD.1. At least 3 inhaler prescriptions.2. Age >55 yrs with no previous use or ICS in 5 yrs.3. Register in health plan for 5 yrs.4. Entry time 3rd prescription between Jan 1990–Dec 1997.Matched for age, duration and frequency of exacerbations.Excluded lengthy hospital admissions. Becl or bud Exposed if recently received ICS prescription in 12 months prior to index date. MI Discharge diagnosis from the hospital DB, and death from vital statistics.Compared to medical charts, diagnostic agreement in hospital DB as high as 97%. RR for AMI with ICS:crude RR 0.86 (95% CI 0.68–1.09); adjusted RR 0.83 (95% CI, 0.63–1.08),adjusted for AMI risk factors and severity of COPD: sex, HTN, DM, HLD, CV disease, number of COPD exacerbations and respiratory prescription. Important baseline differences: sex, risk factors and history of CVD, hospitalisations in past 3 months.No dose information available; duration of exposure extrapolated from quantity dispensed, rather than compliance. Matching for COPD severity inaccurate as relied on co-prescription exposure.Limited data on smoking. Lee 4 32130 cases, 320501 controls for mortality (3159 cases, 31534 controls for CV death) Nested CC US VA, CMS and NDI 260 1. Age >45 yrs of US VA care for >1 yr. 2. ICD-9 diagnosis of COPD between Oct 1, 1999 and Sept. 2003 at two or more outpatient visits within 12 months or primary diagnosis of COPD. NA Any exposure to respiratory prescription in the 180 days before index date. No details on accuracy of pharmacy data. Death, CVD DB captures approximately 98% of veteran deaths. Random sample of 40% with CV death: IHD disease, cardiomyopathy, cardiac arrest, or arrhythmias. Adjusted OR for ICS: all-cause death 0.80 (95% CI 0.78– 0.83); CVD 0.80 (95% CI 0.72–0.88), adjusted for respiratory and cardiac prescriptions, exacerbations, and presence of CV disease. Imbalances in comorbid cardiac conditions and cardiac prescription use, and COPD exacerbations. Confounding by indication. Did not ascertain COPD severity or smoking status. Unlikely to find significant differences due to low rates of exposure. Matched on sex, age, region, and year of diagnosis. Immortal time bias. Uncertain accuracy of diagnosis of CVD. Macie 5 1629 ICS users, 2393 non-users Cohort, nested CC Manitoba Population Health Research Repository (Canada) 39 1. Discharged from hospital with primary ICD code of COPD between Apr 1996–Mar 2000.2. Age >35 yrs.3. Resident of the province ≥1 yr prior and 1 yr post-discharge until death.Patient who died within 90 days of hospital discharge excluded. NA Provincial retail pharmacies capture all dispensing of prescriptions except for in-patient drugs.DB has anonymous recipient IDs and information about the prescription dispensed. Death, CVD Death from any cause in the 275 days after hospital discharge. Analysis of death certificates for: COPD, asthma; CV and other causes. Adjusted HR for death with ICS within 90 days of discharge.Aged >65 yrs, 0.75 (0.61–0.91).Note: absolute mortality among age >65 yrs: 11.7% in ICS users; 13.1% in non-users.ICSs reduced the risk of death by 23% (95% CI 6–37%) and CV deaths by 38% (95% CI 11–57%) compared to bronchodilators. Significant baseline differences: age, Charlson score, respiratory prescriptions. Confounding exists.No prescription data while hospitalised so patients admitted in first 90 days of study received less ICS and likely to be high mortality group.Difficulty in judging actual drug usage, and cause of death. Mapel 40 786 ICS users, 397 SABA users RC Two regional MCOs in the USA 96 1. Aged >40 yrs.2. Had >90-day use of an ICS or SABA.3. At least two outpatient visits or one hospital admission with relevant ICD-9 code between 1995–2000.Follow-up 1st day following 90-day period to death or disenrolment. NA Pharmacy claims for ≥90-day cumulative of: 1) ICS alone, 2) LABA alone, or 3) ICS + LABA. Death Death obtained from state vital statistics records and matched on name, SSN and DOB. HR for mortality: ICS versus SABA 0.59 (95% CI 0.46–0.78). Significant baseline differences: age, sex, presence of asthma, disease severity. Confounding by indication.No ascertainment of exposure, compliance or use.Misclassification bias in COPD diagnosis (asthma).Uncertain risk of immortal time bias. Mapel 41 742 ICS users, 1832 SABA users RC, nested CC Four US integrated HMOs 156 At least one in-patient or two outpatient visits for COPD based on ICD-9 codes from Sep 2000 to Sep 2001.Matched on sex, age, data survival follow-up. Flu/sal, any ICS Pharmacy records of prescriptions using National Drug Codes. Duration extrapolated from units dispensed. Prescriptions reviewed for missing data. Death Death during study period Sept 2000–Sept 2003 ascertained through local vital statistic registers, matched by name, sex DOB and SSN. HR for mortality ICS versus SABA 0.76 (0.61–0.95).HR for mortality in propensity matched cohort: ICS versus SABA 0.75 (0.58–0.97).RR for death with ICS in nested CC RR 0.86 (95% CI 0.46–0.96). Significant baseline differences: age, hospitalisation for COPD, comorbidities. Discrepancy between prescription and actual use.Duration extrapolated.Industry funded. Sin 43 11481 ICS users, 11139 non-users RC CIHI hospital discharge DB in Ontario (Canada) 52 1. ICD-9 code for at least one hospitalisation with main discharge diagnosis of COPD between April 1, 1992 and March 31, 1997.2. Aged >65 yrs.3. Survive ≥30 days after discharge. Becl, bud, triam, fluni Ontario Drug Benefit database. Death Captures all decedents of Ontario, including date of death. Adjusted RR for death with ICS use (within 90 day post-discharge RR 0.71 (95% CI, 0.65 to 0.78), adjusted for age, sex, Charlson score exacerbations and co-medication. Stratified analysis on Charlson score, sex, and age did not change association. Significant baselines differences: age, Charlson index, prescriptions and emergency visits.Confounding by indication.No verification of actual medication usage. Risk of immortal time bias. Sin 42 3343 ICS users, 3397 non-users RC CIHI hospital discharge in Alberta (Canada) 128 1. ICD-9 code for at least one hospitalisation with main discharge diagnosis of COPD between April 1, 1994 and March 31, 1998.2. Aged >65 yrs.3. Excluded those with primary diagnosis of asthma. ICS Crosschecked with Alberta Blue Cross DB with record of quantity and date dispensed.Doses imputed. Death Vital statistics with electronic file of all deceased persons in Alberta, including dates of death. All cause death for ICS users versus non-users.Crude RR 0.61 (95% CI 0.56–0.66). Adjusted RR 0.75 (95% CI 0.68–0.82), adjustments for age, sex, comorbid conditions, ICU stay and use of other pulmonary prescription. Significant baseline differences in age, Charlson comorbidity score and use of prescriptions.Unclear, which ICS studied, and what doses.No verification of actual use.Unclear risk of immortal time bias. Soriano 45 431 ICS users, 3620 non-users RC UK GPRD 156 1. Newly diagnosed COPD between 1990–1999.2. Aged >50 yrs.3. Received ≥3 prescriptions over 6 months.4. Alive for 6 months after entry. Flu Prescriptions in 90 days post-hospital discharge. Death Date of death identified with Specific OMIS code. HR for fluticasone (3 yr death).HR 0.62 (95% CI 0.45–0.85), Adjusted for age, sex, year of entry, smoking, comorbid conditions and oral steroid use. Significant baseline differences: age, sex, prescription use, comorbidity.No verification of actual use.Risk of immortal time bias.Industry funded. Soriano 44 3049 ICS users, 627 SABA users RC UK GPRD 1990–1999 52 1. Newly diagnosed COPD.2. Aged >50 yrs.3. 1st hospitalisation for COPD related condition.4. At least 1 prescription for respiratory condition in first 90 days after discharge. Beclo, bud, flu Based on prescription by GP in 90 days post-discharge. Death NA Death rate in 1 yr 17.1% in ICS users versus 24.3% in control group. Significant baseline differences in age, smoking prescription, and hospitalisation.Confounding by indication.Ascertainment of mortality.Unclear risk of immortal time bias.Drug dosage unclear.Actual use may differ.Industry funded. 5. Excluded if died or re-admitted within 30 days. Tkacova 46 55 ICS users, 90 non-users RC Slovakian university hospital 52 1. Documented outpatient clinic visit or an in-patient hospitalisation with primary diagnosis of COPD.2. At least one bronchodilator before the index visit or hospitalisation date.3. LTOT prescription between 1996–2002.4. Stable condition at the time of LTOT initiation.Prescribing physician recorded details of prescription at time of initiation of O2. Becl (n = 45), flu (n = 6), bud (n = 4) Whether patients were or were not receiving ICS at time of LTOT initiation. Death Survival data from records of home O2 vendors captured death. HR for death with ICS use.HR 0.38 (95% CI 0.18–0.79). Adjusted HR 0.46 (95% CI 0.21–0.98), adjusted for age, sex, co-medication, Pa,O2 and Pa,CO2.ICS users had significantly greater 1-yr survival (46/55 or 84%) than non-users (54/90 or 60%).(Log-rank statistics p<0.05). Significant baselines differences in use of SABA, arterial hypertension and severity of COPD.Misclassification as exposure status based on single time-period, and patients may have started on ICS after that.Risk of confounding as no adjustment for risk factors. Vollmer 47 863 regular ICS users, 996 irregular ICS users, and 1043 non-users RC US Kaiser Permanente 208 1. Aged >50 yrs as of Jan 2000.2. Enroled between 1998–1999.3. Outpatient or ED visit with ICD-9 COPD code.4. ≥6 prescriptions of respiratory drugs, with ≥1 prescription dispensed Sept–Dec 1999. NA EMR.One or more dispensing event during each of the three preceding 2 months. Death Vital statistics registers of Oregon and Washington. 29.5% had incomplete follow-up. RR for death (no asthma): never smokers: 0.47 (0.19–1.16, p = 0.10); ex-smokers: 0.76 (0.56–1.02, p = 0.07); current smokers 1.09 (0.65–1.83, p = 0.74); adjusted for age, sex, comorbidity, use of home O2, pulmonologist, COPD hospitalisation or ED care, and propensity to use ICS. Significant baselines differences: smoking, co-existing asthma, pulmonologist care, ED care.No verification of compliance.Incomplete follow-up.Industry funded. PC: prospective cohort; VA: Veterans Affairs; DB: database; ICD: International Statistical Classification of Diseases and Related Health Problems; COPD: chronic obstructive pulmonary disease; ACQUIP: Ambulatory Care Quality Improvement Project; RCT: randomised controlled trial; Becl: beclometasone; triam: triamcinolone; fluni: flunisolide; flu: fluticasone; HR: hazard ratio; CC: case–control; bud: budesonide; MI: myocardial infarction; RR: relative risk; AMI: acute myocardial infarction; HTN: hypertension; DM: diabetes mellitus; HLD: hyperlipidaemia; CVD: cardiovascular disease; CMS: Center for Medicaid Services; NDI: National Death Index; NA: not available; IHD: ischaemic heart disease; ID: identification; SABA: short-acting β-agonist; MCO: managed care organisation; LABA: long-acting β-agonist; RC: retrospective cohort; SSN: social security number; DOB: date of birth; HMO: health maintenance organisation; Sal: salmeterol; CIHI: Canadian Institute of Health Information; ICU: intensive care unit; GPRD: General Practitioner Research Database; OMIS: Oxford Medical Information Systems; GP: general practitioner; LTOT: long-term oxygen therapy; Pa,O2: arterial oxygen tension; Pa,CO2: arterial carbon dioxide tension; ED: emergency department; EMR: Electronic Medical Record.










