





Abstract
The present study aimed to investigate potential effects of curcumin (CUR) and dexamethasone (DXM) on ischaemia–reperfusion (I/R) induced lung injury in rats.
Experimental rats were pre-treated with a single i.p. dose of vehicle, CUR (50 mg·kg−1 or 200 mg·kg−1) or DXM (5 mg·kg−1), 2 h before anaesthesia and subjected to left lung hilus clamping with 90-min ischaemia followed by 4 h of reperfusion.
Pre-treatment with CUR (200 mg·kg−1) or DXM markedly attenuated I/R-induced barrier disruption, lung oedema, tissue inflammation, hypoxaemia 4 h after reperfusion, and overactivation of nuclear factor-κB, inflammatory cytokines, myeloperoxidase and malondialdehyde.
It appears that curcumin attenuates acute lung injury, probably through improving oxidative stress and inhibiting nuclear factor-κB-mediated expression of inflammatory cytokines. Thus, curcumin may be an alternative therapy for improving the outcomes of ischaemia–reperfusion-induced lung injury.
Ischaemia–reperfusion (I/R)-associated acute lung injury (ALI) occurs in many clinical situations such as lung transplantation and becomes life-threatening in ∼20% of transplants, resulting in the primary dysfunction of implanted lungs and a mortality rate of 60% 1, 2. Such compromise usually appears in the early stages of lung transplantation, characterised by nonspecific alveolar damage, lung oedema and hypoxaemia, as reported in clinical studies 3. It is important to elucidate the molecular mechanisms of I/R-ALI in order to develop an effective therapeutic strategy. For instance, the redox-sensitive transcription factor nuclear factor (NF)-κB, which regulates genes encoding proinflammatory mediators, plays a pivotal role in the development of I/R injury. The inhibition of NF-κB activation could attenuate I/R-induced tissue injury 4, 5.
Curcumin (CUR), an active component of the rhizome Curcuma longa, shows wide anti-inflammatory, antioxidant and bactericidal effects 6, 7. CUR downregulates the production of tumour necrosis factor (TNF)-α and interleukin (IL)-1 and inhibits the activation of NF-κB and activator protein-1 7. Dexamethasone (DXM) modulates enzyme systems and inhibits the formation of cytokines, arachidonic acid products and NF-κB activation 8, 9. Pre-treatment with CUR or DXM has been suggested to reduce I/R-induced injury in multiple organs and tissues 10–14. It was proposed that CUR and others might have a similar mechanism to glucocorticoids in the treatment of I/R injury 13. The present study aimed to investigate the effects of CUR or DXM on alveolar–capillary membrane disruption, lung oedema, neutrophil lung tissue infiltration and hypoxaemia in a rat model of I/R-ALI.
MATERIALS AND METHODS
Animals and surgical preparation
Male Sprague–Dawley rats (Animal Center, Fudan University, Shanghai, China) weighing between 250–300 g, were used. The animals had no access to solid food but free access to water 12 h before the experiments. The experimental protocol was approved by the Committee of Animal Care (Fudan University). All animals were handled in accordance with the Guide for the Care and Use of Laboratory Animals 15. Modified operations were performed as described previously 16. Animals were anaesthetised by an i.p. injection of pentobarbital sodium at 50 mg·kg−1 and i.m. injection of atropine at 0.2 mg. After cannulation, rats were mechanically ventilated (Harvard Rodent Ventilator Model 683; Harvard Apparatus, South Natick, MA, USA) with a standardised inspiratory oxygen fraction (FI,O2) of 60% at a rate of 75 breaths·min−1, a tidal volume at 10 mL·kg−1, positive end-expiratory pressure at 2 cmH2O and arterial partial pressure of carbon dioxide (Pa,CO2) at 30–45 mmHg. A 22-gauge cannula inserted into the right carotid artery was used to monitor arterial blood gases (ABG) and draw blood samples. The animals were placed on their right sides, and a left anterolateral thoracotomy in the fifth intercostal space was performed. The left lung was mobilised atraumatically and the inferior pulmonary ligament was divided sharply. At this point, all animals received 50 U of heparin i.v. After blood was harvested from the right carotid artery (CA) for ABG of pre-ischaemia, the pulmonary hilum was occluded with a non-crushing microvascular clamp, including the left main bronchus, artery and vein, for 90 min. After 90-min left-lung ischaemia, the clamp was removed and the lung was ventilated and reperfused for 4 h. At the end of the reperfusion period, ABG were measured from CA and left pulmonary vein (LPV), and the Pa,O2/FI,O2 value was compared with the pre-ischaemia value. Lung tissues were harvested for further analysis after the experiment was terminated. Surgery and tissue analyses were performed blindly.
Experimental groups
Animals were divided randomly into six experimental groups (n = 12 animals per group): naïve animals (control); animals undergoing a sham operation and pre-treated with vehicle (sham); or animals with I/R-ALI and pre-treated with either vehicle, CUR at 50 mg·kg−1, CUR at 200 mg·kg−1 or DXM at 5 mg·kg−1. Of these, 36 animals were used for measurement of lung microvascular permeability and 36 for the lung function and biochemical assays, in order to avoid contamination with Evans blue dye (EBD). CUR (Sigma-Aldrich Co., St. Louis, MO, USA) dissolved in dimethyl sulphoxide (DMSO) and DXM (Tianjin Pharmaceutical Co., Tianjin, China) in physiological saline were administered i.p. 2 h prior to I/R induction. The doses of CUR and DXM used in the present study were based on previous experiments 10, 14 and the current authors’ preliminary studies. In pilot studies, CUR dose ranges of 25–400 mg·kg−1 were tested; a dose of 200 mg·kg−1 showed significant inhibitory effects on I/R-induced changes in vascular permeability and CUR treatment at 200 mg·kg−1 2 h prior to anaesthesia was more effective than treatment after the induction of ischaemia (data not shown). Doses of 50 and 200 mg·kg−1 CUR were used in the current experiments.
Lung tissue oedema and morphology
The left lungs were harvested for measurements of lung tissue oedema by lung wet/dry weight ratio and morphology by staining with haematoxylin and eosin. All microscopic sections were interpreted, blinded, by a pulmonary pathologist. Lung neutrophil sequestration was measured by counting lung tissue neutrophils and was expressed as the number of neutrophils per 10 high-power fields of lung tissue, as described previously 17.
Lung microvascular permeability
Plasma leakage was measured using the EBD method, with minor modifications 18. Animals received 30 mg·kg−1 dye i.v. 30 min before the end of the reperfusion period. After the reperfusion period, median sternotomy was performed and heparin (500 units) was infused into abdominal aorta. An 18-gauge cannula was inserted into the main pulmonary artery. The left atrial appendage and left ventricle were incised to allow free flow of effluent blood from the lung. The pulmonary vasculature was flushed with 50 mL of physiological saline at 20 cmH2O. After the dried tissues were immersed in 3 mL formamide and homogenised, the homogenate was incubated at 37°C for 24 h and centrifuged at 5,000 g for 30 min. The optical density of the supernatant was measured by spectrophotometry at 620 nm. For qualitative examination, lungs were sectioned into 10-μm slices and examined by fluoromicroscopy.
Myeloperoxidase activity and oxidative stress assay
The left lung was used to determine pulmonary tissue myeloperoxidase (MPO) activity. Tissue MPO activity was measured to quantify polymorphonuclear leukocyte accumulation in the lungs 19. The supernatant from lung homogenising buffer was used for determinations of the enzymatic activities of xanthine oxidase (XO) 20, malondialdehyde (MDA) 21 and the total antioxidative capacity (TAOC) 22. The activities of MPO, XO and MDA, and TAOC in the lung tissue were determined using assay kits (Jiancheng Bioengineering Institute, Nanjing, China), according to the manufacturer's instructions.
NF-κB, TNF-α and IL-1β measurements
To observe changes in NF-κB activity, DNA binding activity was measured using an ELISA assay. Nuclear extracts of left lungs were prepared using the Nuclear Extract Kit (Active Motif, Carlsbad, CA, USA). P65 DNA binding activity was measured with 15 μg of nuclear extract with the Trans-AM kit (Active Motif) according to the manufacturer's instructions 11. TNF-α and IL-1β levels in left lungs and serum were determined using a rat TNF-α ELISA kit and IL-1β ELISA kit (R&D Systems, Minneapolis, MN, USA), respectively, as described previously 23.
Statistical analysis
Results are presented as mean±sd. Comparisons between multiple groups were performed by one-way ANOVA procedures, followed by Bonferroni's post hoc test for intergroup comparisons; in the case of unequal variances, a nonparametric Kruskal–Wallis test was performed. A p-value <0.05 was regarded as statistically significant.
RESULTS
Histopathology and lung injury score
Figure 1⇓ shows the different degrees of I/R-ALI induced by the various treatments. Lung tissue oedemas in I/R-ALI animals pre-treated with vehicle or CUR at 50 mg·kg−1 were more obvious than those in sham-operated animals (fig. 1⇓), while pre-treatment with CUR at 200 mg·kg−1 or DXM prevented from I/R-induced lung tissue oedema. The severity of ALI, characterised by lung tissue oedema, leukocyte infiltration and haemorrhage, was more obvious in I/R-ALI animals than in sham-operated animals, while CUR at 200 mg·kg−1 and DXM had preventive effects, as seen morphologically in figure 1⇓.
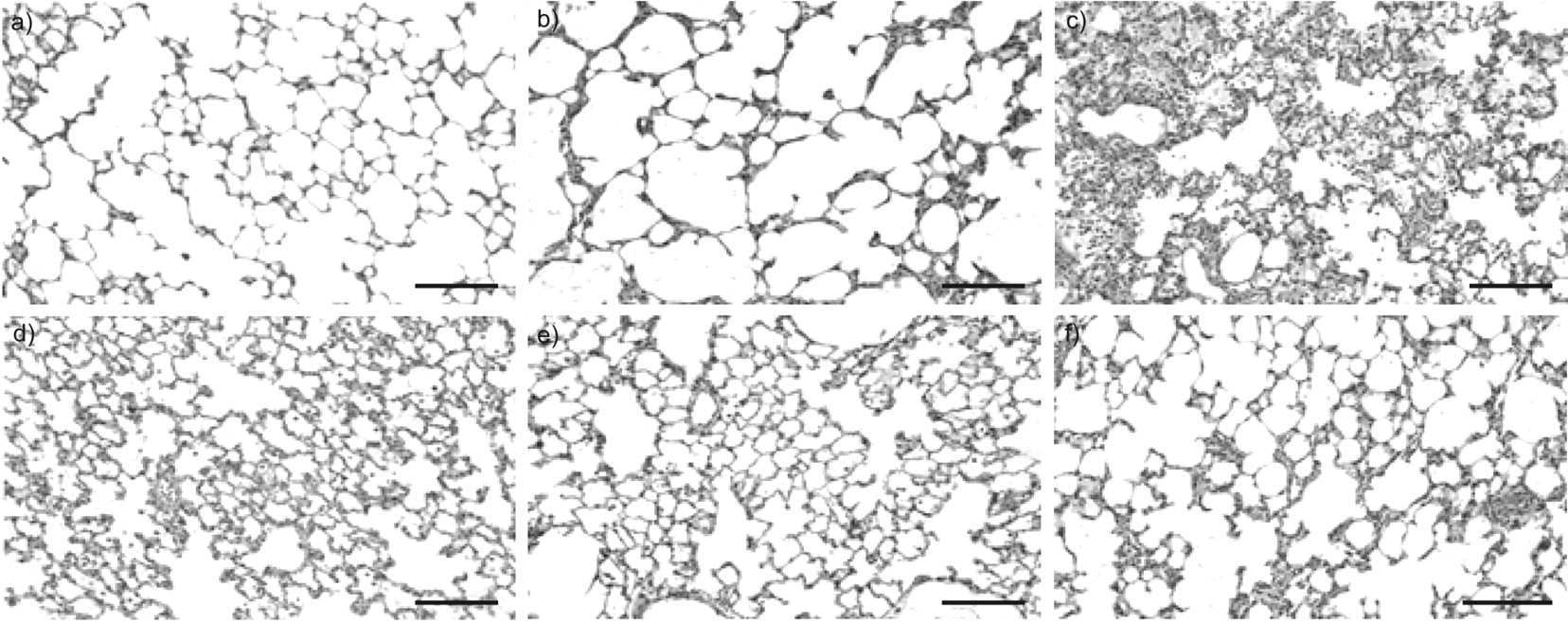
Morphological evaluation of left lungs after 90 min ischaemia and 4 h reperfusion. Lung histopathological slices were stained with conventional haematoxylin and eosin. Lungs from: a) control animal and b) animals undergoing a sham operation and pre-treated with vehicle; or animals with ischaemia–perfusion-associated acute lung injury and pre-treated with c) vehicle, d) curcumin at 50 mg·kg−1, e) curcumin at 200 mg·kg−1, or f) dexamethasone at 5 mg·kg−1. Scale bars = 50 μm.
ABG and lung wet/dry weight ratio
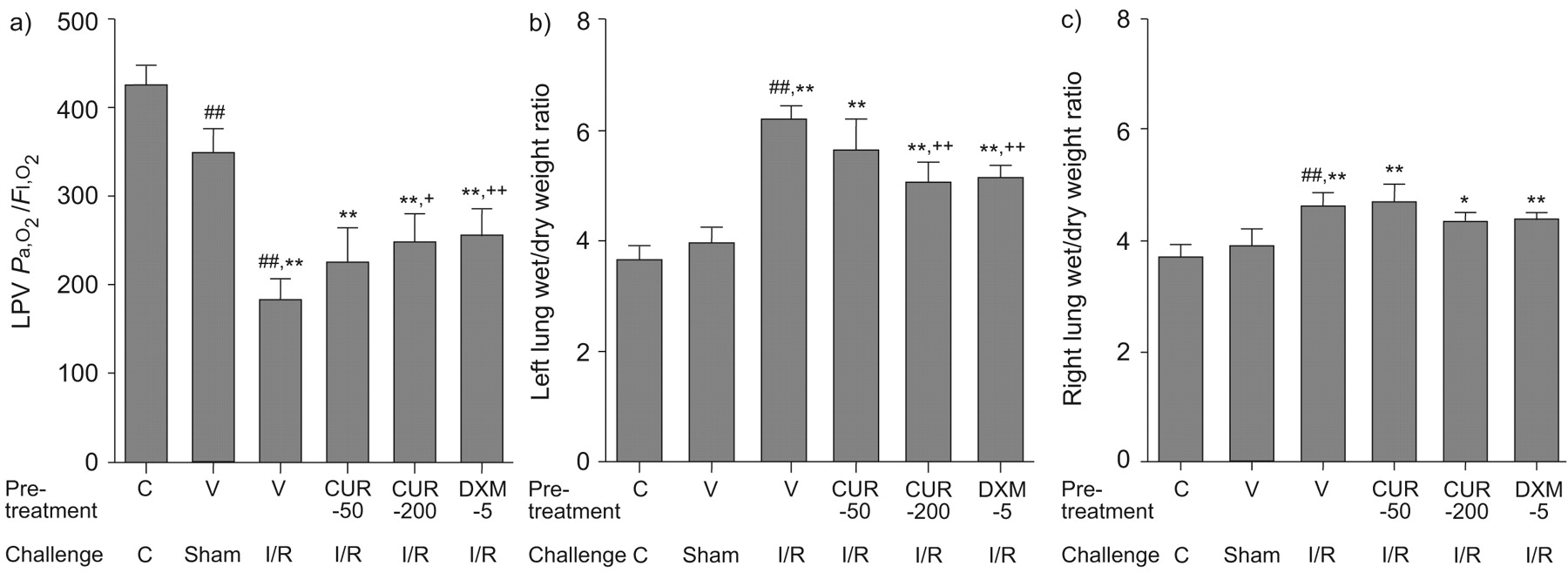
Values of CA Pa,O2/FI,O2, LPV Pa,O2/FI,O2(fig. 2a⇓), left lung water content (fig. 2b⇓) and right lung water content contra-lateral to the I/R side (fig. 2c⇓) in all I/R-ALI animals were significantly lower or higher than those in sham and control animals (p<0.05 and p<0.01, respectively). However, pre-treatment with CUR at 200 mg·kg−1 or DXM significantly prevented I/R-induced changes of LPV Pa,O2 (p<0.05 and p<0.01, respectively; fig. 2a⇓) and left lung water content (p<0.01; fig. 2b⇓), compared with vehicle pre-treatment.
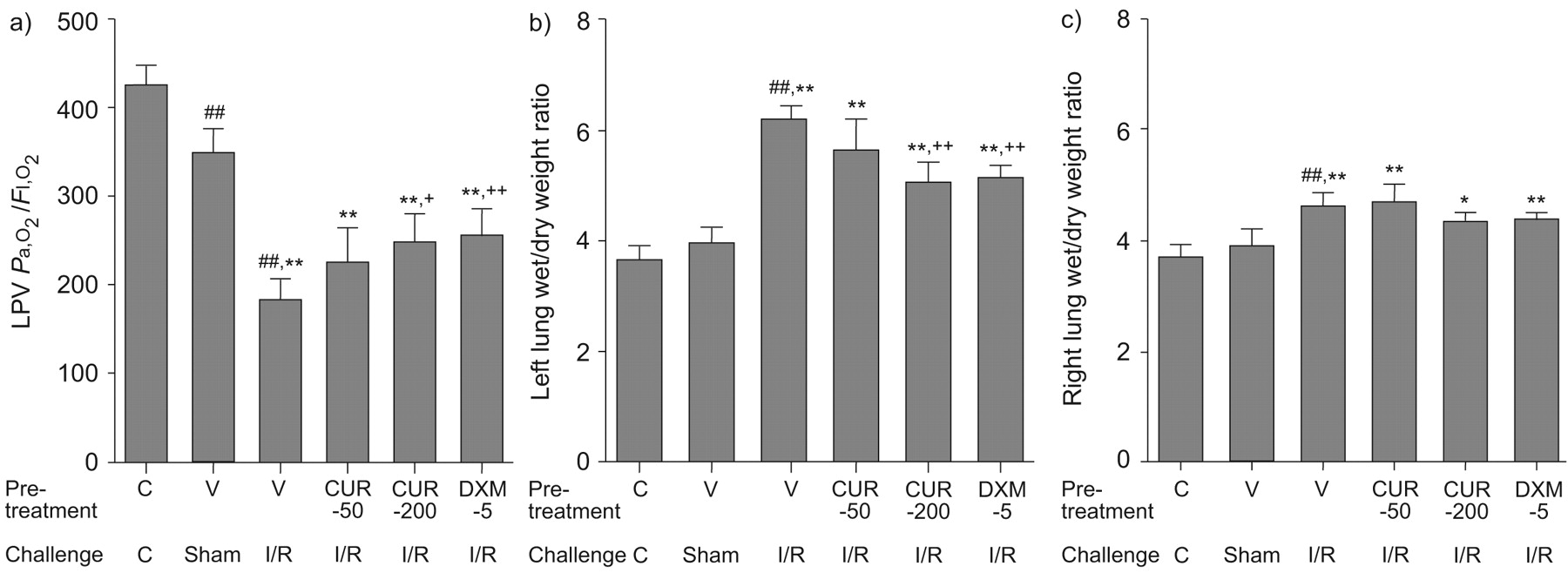
The a) arterial oxygen tension/inspired oxygen concentration (Pa,O2/FI,O2) ratio in the left pulmonary vein (LPV) and lung wet/dry weight ratio of b) the left lungs and c) the right lungs of control (C) and experimental animals. CUR-50: pre-treatment with 50 mg·kg−1 curcumin; CUR-200: pre-treatment with 200 mg·kg−1 curcumin; DXM-5: pre-treatment with 5 mg·kg−1 dexamethasone; V: vehicle; Sham: sham operation; I/R: ischaemia–reperfusion. *: p<0.05 versus sham operation group; **: p<0.01 versus sham operation group; ##: p<0.01 versus control group; and +: p<0.05 versus I/R-associated acute lung injury (ALI); ++: p<0.01 versus I/R-associated ALI.
Lung microvascular permeability
A significant increase in EBD extravasation was found in I/R left lungs of animals pre-treated with vehicle, CUR or DXM, as compared with sham and control animals (p<0.01; fig. 3a⇓). Pre-treatment with CUR at 200 mg·kg−1 or DXM significantly prevented I/R-induced increase in capillary barrier permeability, compared with vehicle (p<0.01). A similar pattern of inhibitory effects of CUR or DXM was also seen in the contralateral right lungs (fig. 3b⇓).

Assessment of lung microvascular permeability by quantification of Evans blue dye (EBD) in the parenchymal tissue of a) left lungs and b) right lungs. c–e) Spontaneous red fluorescence of EBD seen in lung tissue sections. c) No extravasation of EBD with a competent alveolar–capillary membrane was observed in animals undergoing sham operation and pre-treatment with vehicle. d) Obvious extravasation of EBD into the parenchyma was observed in ischaemia–perfusion-related acute lung injury (I/R-ALI) animals pre-treated with vehicle. e) Slight extravasation of EBD into the parenchyma was observed in I/R-ALI animals pre-treated with 200 mg·kg−1 curcumin (CUR-200). C: control; CUR-50: pre-treatment with 50 mg·kg−1 curcumin; DXM-5: pre-treatment with 5 mg·kg−1 dexamethasone; Sham: sham operation; I/R: ischaemia–reperfusion. **: p<0.01 versus sham operation group; ##: p<0.01 versus control group; ++: p<0.01 versus I/R-ALI group pre-treated with vehicle. Scale bars = 50 μm.
Lung tissue neutrophilic infiltration and oxidative stress
Values of MPO activity (fig. 4a⇓) and number of neutrophils (fig. 4b⇓) in left lung tissue increased significantly in all animals with I/R-ALI compared with sham and control animals (p<0.01), while pre-treatment with CUR at both 50 and 200 mg·kg−1 or with DXM significantly prevented I/R-increased MPO activity and neutrophil influx in lung tissue. As shown in table 1⇓, tissue levels of MDA and XO increased significantly and tissue levels of TAOC decreased in I/R-ALI animals pre-treated with vehicle (p<0.01 versus both control and sham animals). Both CUR at 200 mg·kg−1 and DXM showed significantly inhibitory effects on I/R-increased tissue levels of MDA. However, only pre-treatment with CUR at 200 mg·kg−1 had significantly inhibitory effects on I/R-increased tissue levels of XO and I/R-decreased levels of TAOC, as compared with vehicle pre-treatment (p<0.05; table 1⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Neutrophilic infiltration assessed by a) lung myeloperoxidase (MPO) activity and b) number of neutrophils per 10 high-power fields of lung tissue. CUR-50: pre-treatment with 50 mg·kg−1 curcumin; CUR-200: pre-treatment with 200 mg·kg−1 curcumin; DXM-5: pre-treatment with 5 mg·kg−1 dexamethasone; C: control; Sham: sham operation; I/R: ischaemia–reperfusion. **: p<0.01 versus sham operation group; ##: p<0.01 versus control group; +: p<0.05 versus I/R-associated acute lung injury (ALI) group pre-treated with vehicle; ++: p<0.01 versus I/R-associated ALI group pre-treated with vehicle.
Levels of xanthine oxidase(XO), malondialdehyde (MDA) and total anti-oxidative capacity (TAOC) in lungs after 90 min ischaemia and 4 h reperfusion
NF-κB DNA binding activity and cytokine alterations
NF-κB activity in lung tissue was significantly higher in all operated animals than in controls and in all I/R-ALI animals than in sham operation animals (p<0.05 and p<0.01, respectively; table 2⇓). Pre-treatment with 200 mg·kg−1 CUR or with DXM significantly prevented I/R-induced NF-κB over-activation (by 64% and 76%, respectively). Table 2⇓ shows that tissue and serum levels of TNF-α and IL-1β increased significantly after induction of I/R, while 50 mg·kg−1 CUR showed significantly inhibitory effects on I/R-induced serum TNF-α and IL-1β and pre-treatment with CUR at 200 mg·kg−1 or DXM significantly inhibited both lung tissue and serum TNF-α and IL-1β.
Levels of nuclear factor(NF)-κB activities, tumour necrosis factor (TNF)-α and interleukin (IL)-1β in lung tissue (t) and serum (s) after 90 min ischaemia and 4 h reperfusion
DISCUSSION
The present study demonstrates protective effects of CUR similar to DXM on I/R-induced lung oedema, lung capillary endothelial barrier dysfunction, leukocyte infiltration, cytokine overproduction and tissue injury. The aim of using DXM in the present study was to evaluate the protective effects of CUR on I/R-ALI, with DXM used as an effective reference compound. However, it was found that only CUR could prevent I/R-increased tissue levels of XO and I/R-decreased tissue levels of TAOC. This may indicate that CUR and DXM exert their anti-inflammatory effects through different pathways. For example, it is possible that CUR might have more preventive effects on oxidative stress. An advantage of CUR is that oral doses of up to 8,000 mg·day−1 appeared non-toxic to humans when taken for 3 months 24. This suggests a potential use of CUR for long-term therapy for I/R-ALI. It was also noticed that left lung I/R caused an increase of capillary barrier permeability in the contralateral lung, which could be prevented by CUR or DXM pre-treatment.
MPO is an enzyme whose level of activity is known to be directly proportional to the number of neutrophils present 19. The present study demonstrated that I/R increased neutrophilic infiltration in lung tissue, as evidenced by both increased MPO activity and number of neutrophils in the tissue. CUR or DXM had anti-neutrophil influx effects. NF-κB is involved in the control of many genes in the early processes of immune and inflammatory responses 9, including the activation of a number of immune response proteins (e.g. TNF-α, IL-1β, IL-6 and IL-8). NF-κB activation is tightly regulated by its endogenous inhibitor, inhibitor of (I)κB, which complexes with NF-κB in the cytoplasm. CUR has been shown to inhibit phosphorylation and proteolytic degradation of IκB and prevent the release and nuclear transmigration of NF-κB 25, similarly to DXM treatment, in cold-preserved alveolar epithelial cells 8. The present study demonstrates I/R-induced over-activation of NF-κB and hyperproduction of inflammatory cytokines both systemically and in local tissue.
Although both warm lung I/R and prolongation of the duration of cold transplantation partially present common pathological characteristics of I/R injury, lung transplantation-associated lung injury also includes graft rejection, injuries induced by lung flushing with organ preservation solution and complicated surgical manipulation. Cold preservation consumes less metabolic substrate than warm ischaemia, which could prolong the preservation time of the lungs. In addition, flushing with preservation solutions before cold storage could alleviate the radicals and mediators of inflammation release after reperfusion to a greater extent than warm ischaemia. Furthermore, lung I/R can also exist in multiple pathophysiological conditions, e.g. shock, haemorrhage and trauma. Clinical and experimental studies have shown that I/R induces a rapid release of proinflammatory cytokines in the lung 3. It is possible that ischaemia triggers the activation of donor macrophages, resulting in the release of proinflammatory cytokines and the development of I/R-ALI during the early phase of reperfusion 26. That CUR or DXM could reduce levels of TNF-α and IL-1β after reperfusion indicates that they may inhibit activation of macrophages at the early phase of reperfusion. It seems that systemic levels of cytokines were more sensitive to CUR pre-treatment.
Oxidative stress plays an important part in experimentally induced reperfusion injury models 27 and IR-induced lung injury 28. One important mechanism leading to the production of radicals is the accumulation of hypoxanthine and the conversion of the enzyme xanthine dehydrogenase into XO during anoxia, with the degradation of hypoxanthine into superoxide after reoxygenation 29. XO-derived superoxide formation accounts for the major part of total superoxide produced during IR injury 27. A recent study also showed that XO plays a prominent role in ALI because of its ability to generate radicals, such that activation of lung XO contributed to the development of capillary permeability related to ventilator-induced lung injury 30. The current results and others 31 have demonstrated that CUR could prevent I/R-induced XO over-activity, which indicates that CUR may directly prevent the production of superoxide during lung I/R. Thus, CUR has the potential to decrease oxidative stress-induced lipid peroxidation.
The balance between radical production and endogenous antioxidants is disturbed by increasing generation of radicals and reduced antioxidant defences during I/R of the lung, resulting in severe oxidative stress, confirmed by a reduction in TAOC after I/R injury. Antioxidant treatment should reverse oxidative stress and the subsequent inflammatory effects through NF-κB activation. The present study showed that CUR or DXM reduced the concentration of MDA during I/R, while only CUR showed preventive effects on I/R-induced reduction of TAOC. The inhibitory effect of DXM on I/R-induced lipid peroxidation in the lung may result from anti-inflammatory activity rather than from direct antioxidant activity.
CUR is a major constituent of turmeric, while DXM is a synthetic drug. Their usage and dosage were both different in the present study. CUR is liposoluble and needed to be dissolved in DMSO. Although the present study showed preventive effects of both CUR and DXM, more attention should be paid to understanding the potential mechanisms by which CUR may be involved in the metabolism and balance of oxidative stress and antioxidants and to exploring clinical application of CUR for preventing oxidative stress. It should be investigated whether CUR has preventive and therapeutic effects on long-term lung I/R injury, organ dysfunction and the mortality rate of I/R-ALI.
In conclusion, the present study confirmed the protective effects of curcumin on ischaemia–reperfusion-induced lung inflammation, capillary barrier dysfunction, tissue oedema and injury, in a similar manner to the steroid dexamethasone. Curcumin reduces ischaemia–reperfusion-induced acute lung injury, probably through improvement of oxidative stress and nuclear factor-κB-mediated expression of inflammatory cytokines. Thus, curcumin may be an alternative therapeutic strategy for improving the outcome of ischaemia–reperfusion-induced lung injury.
Support statement
The present study was supported by grant B115 from the Shanghai Leading Academic Discipline Project (Shanghai, China).
Statement of interest
None declared.
Acknowledgments
The present authors gratefully thank D. Zhu (Zhongshan Hospital, Fudan University, Shanghai, China) and B. Sun (Children’s Hospital, Fudan University) for providing technical and material assistance.
- Received October 28, 2007.
- Accepted August 29, 2008.
- © ERS Journals Ltd
References










