





Abstract
The proportion of recurrent tuberculosis (TB) cases caused by re-infection has varied widely in previous studies. The aim of the present study was to determine the relative frequency of relapse and exogenous re-infection in patients with second episodes of TB, using DNA fingerprinting.
A population-based retrospective longitudinal descriptive study was conducted in Madrid (Spain) during 1992–2004. The study consisted of 645 patients with culture-confirmed TB. Of these, 20 (3.1%) were retained because they presented with a second isolate of Mycobacterium tuberculosis. Finally, 12 of these cases were excluded because they did not complete the full treatment prescribed. All strains were typed by restriction fragment length polymorphism analysis and some by mycobacterial interspersed repetitive unit-variable number of tandem repeats analysis. The patients with recurrent TB were compared with those without recurrent TB.
For seven out of the eight patients, the restriction fragment length polymorphism patterns of the Mycobacterium tuberculosis strains from the episodes of recurrent disease showed identical initial and final genotypes, indicating relapse; the remaining recurrent case showed different genotypes, suggesting exogenous re-infection.
Re-infection is possible among people in developed countries, but the rates are lower than those occurring in high-risk areas. The risk factors for recurrent tuberculosis should be taken into account in the follow-up of treatment and tuberculosis control strategies.
The role of re-infection compared to relapse in the recurrence of tuberculosis (TB) in general is still unclear and has potential implications for public health 1, 2. The relative contributions of re-infection and relapse are likely to depend upon the epidemiological context. In populations at high risk of infection, there is a substantial chance of repeated infection, and hence re-infection may be a major contributor to the overall rate of TB in adults. However, in populations with a low risk of infection, there is little probability of repeat infection, and thus most cases of second episodes of TB in adults are probably the result of relapse 3.
With the introduction of short-course combination therapy, the relapse rate has dropped from 21 to 1–2% 4, calling into question, in an era of effective treatment regimens, the notion that multiple episodes of TB in one patient are almost always caused by endogenous reactivation. The Mycobacterium tuberculosis genotype can now be characterised by DNA fingerprinting, which can reveal whether a new episode of the disease was caused by infection with the same strain that caused a previous episode or a different strain.
In the present study, DNA fingerprinting was used to determine the relative frequency of relapse and exogenous re-infection in patients with second episodes of TB. The aim was to determine the importance of this distinction in terms of the efficacy of current treatment regimens, and the control of TB.
MATERIALS AND METHODS
Study population and data collection
The present investigation was a population-based retrospective longitudinal descriptive study. The cohort of TB patients included those whose diagnosis was confirmed between January 1, 1992 and December 31, 2004 in the 10th health district of Madrid (Spain).
Patients who met the following criteria were included in the analysis: 1) patients suffering from an episode of TB with a positive culture for M. tuberculosis; and 2) patients suffering from a subsequent episode of TB with an isolate of M. tuberculosis after completing the full anti-TB treatment. The treatment regimens used included: 1) 2 months of isoniazid (H), rifampicin (R) and pyrazinamide (Z) followed by ≥4 months of H and R; and 2) 2 months of H, R, Z and ethambutol (E) followed by ≥4 months of H and R. Patients who yielded a second isolate of M. tuberculosis but who did not complete the full treatment prescribed were defined as noncompliant and excluded from the study.
Patient information was obtained from the Regional Tuberculosis Case Register (of the Regional Programme of Tuberculosis Prevention and Control of the Autonomous Community of Madrid), which contains information on demographics, treatment, bacteriology and outcome for all suspected and confirmed cases of TB.
Procedures
All M. tuberculosis strains were sent to the laboratory of the Mycobacteria Genetics Group (Faculty of Medicine, Saragossa University, Saragossa, Spain) and subjected to standardised insertion sequence (IS) 6110-based restriction fragment length polymorphism (RFLP) typing, as described elsewhere 5. Since differentiation of M. tuberculosis strains carrying few IS6110 copies is poor, all strains with four or less IS6110 copies were subjected to subtyping by means of spoligotyping analysis 6. Similarity among strains was compared using BioNumerics version 4.5 software (Applied Maths, Kortrijk, Belgium).
All patients in clusters were investigated for possible cross-contamination. Laboratory cross-contamination was considered if: 1) the patient showed no clinical evidence of TB; 2) each patient yielded a single positive culture but a negative smear for acid-fast bacilli; and 3) the sample was processed on the same day as other patients’ cultures and showed identical RFLP patterns.
Isolates taken from seven out of the eight patients that belong to the recurrent TB group could be typed by means of the mycobacterial interspersed repetitive unit-variable number of tandem repeats (MIRU-VNTR) system based on 15 loci 7.
Drug susceptibility testing for H, R, streptomycin and E was performed by the proportion method and, from 2004, using another system (BACTEC MGIT 960; Becton Dickinson Microbiology Systems, Sparks, MD, USA).
Definition of relapse and re-infection
A patient whose isolates of M. tuberculosis from the first and second episodes of TB were identical on RFLP analysis with each DNA sample was considered to have TB due to relapse. A patient whose isolates from the first and second episodes of TB were different was considered to have TB due to a new exogenous infection.
Statistical analysis
The epidemiological variables were subjected to univariate analysis. Patients who had a re-infection or relapse were compared with patients with no re-infection or relapse on the basis of selected demographic, epidemiological, clinical and diagnostic features. The Chi-squared test or Fisher’s exact test were performed to test the association of recurrent TB with predictor variables. Predictor variables that were associated with recurrent TB to a significant degree (p<0.005) were included in a bivariate correlation model and linear regression analysis to calculate the odds ratios with their confidence intervals.
RESULTS
Out of the total 645 patients with positive cultures assessed during the study period, 20 (3.1%) were studied because they yielded a second isolate of M. tuberculosis after receiving treatment. After a careful review of all clinical charts, eight (1.2%) of these cases were included as they had completed the full treatment prescribed, and were assigned to the recurrent TB group; 12 were excluded from the study as they had not completed the full treatment prescribed, and were assigned to the noncompliance group. None of the positive cultures for M. tuberculosis from the eight patients arose due to cross-contamination.
During the study period (January 1992 to December 2004), DNA from cultures of M. tuberculosis was available for at least one RFLP analysis for 529 (83.6%) out of 633 patients. Fingerprinting results were available for all eight patients with at least two cultures positive by RFLP analysis and for seven out of the eight patients by MIRU-VNTR analysis. All isolates from these patients showed five or more copies of IS6110.
The demographic and clinical characteristics of the eight patients with recurrent TB are shown in table 1⇓. The mean age of these eight patients was 38.6±9.5 yrs (median 36.5 yrs); the majority of the patients were male 6. All of the patients were born in Spain; four were infected with HIV, five had a history of drug use, five were alcohol abusers and another seven were smokers. None of the patients had a medical history of diabetes, end-stage renal disease or cancer, or had been treated with immunosuppressant drugs. Seven patients had pulmonary disease alone and one had both pulmonary and extrapulmonary disease. Chest radiography revealed evidence of cavitary disease in five patients during the first episode of TB and in two during the second episode. Seven patients yielded a positive acid-fast direct smear during the first or second episodes.
Demographic, epidemiological, clinical and diagnostic characteristics of eight recurrent tuberculosis patients
The mean±sd interval between cure and subsequent diagnosis (isolation of a subsequent culture-positive specimen) was 54.4±37 months (median (range) 64.5 (9–113) months).
Age, sex and a positive acid-fast direct smear were not found to be risk factors for recurrent TB. However, drug and alcohol abuse, HIV infection, smoking and chest radiography showing a cavitary lesion were identified as significant risk factors for recurrent TB, as shown in table 2⇓.
Risk factors for recurrent tuberculosis
Isolates taken from the patients during the first and second episodes of disease were susceptible to all of the antimicrobial agents tested.
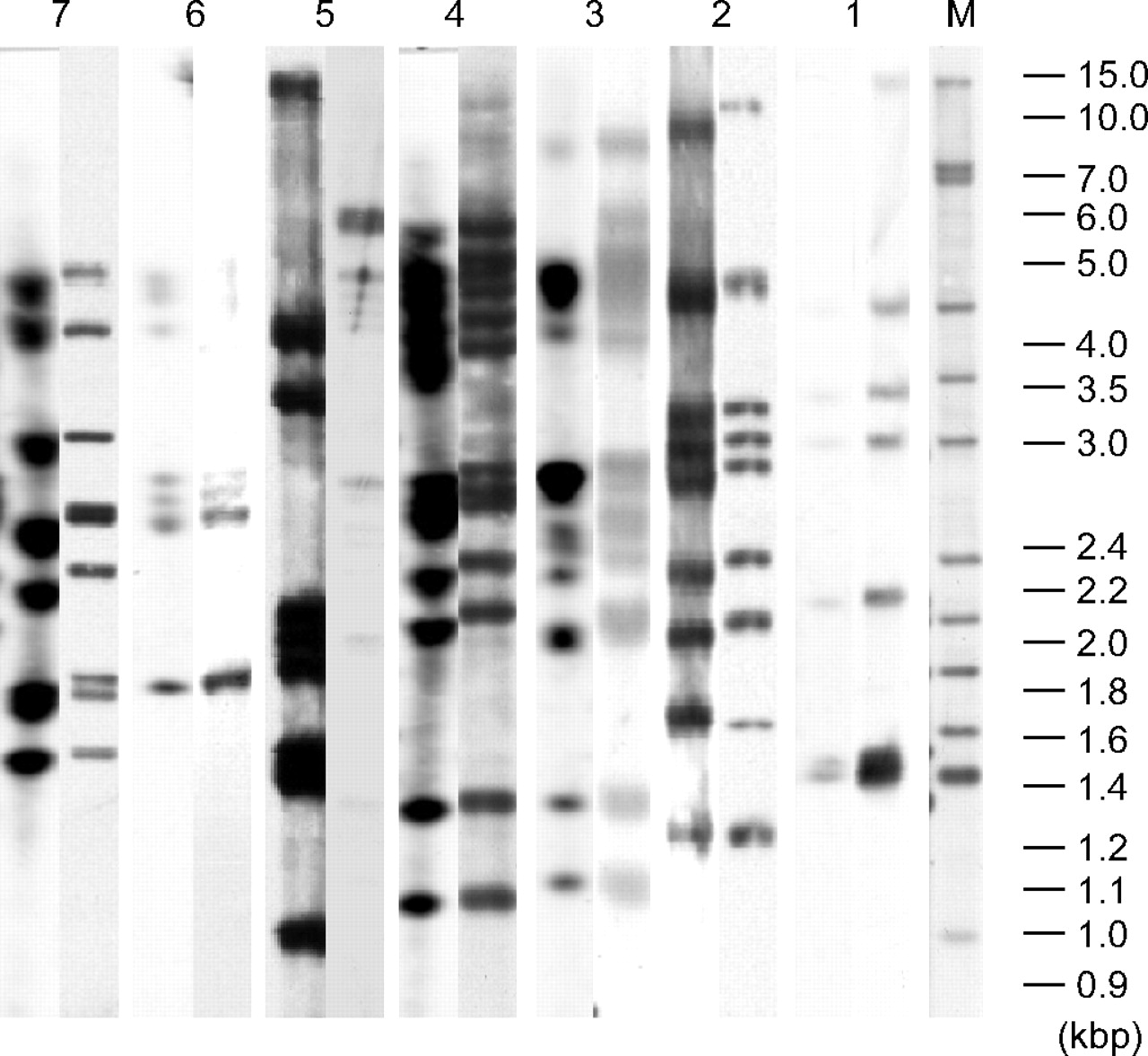
For seven out of the eight patients, the RFLP patterns of the strains of M. tuberculosis from the episode of recurrent disease indicated identical initial and final genotypes, indicating relapse. The remaining recurrent case showed different genotypes in the two episodes, suggesting exogenous re-infection (fig. 1⇓; table 3⇓). The same results were obtained when MIRU-VNTR analysis was used.
{kind=link}
Restriction fragment length polymorphism patterns of bacterial isolates from first and second episodes of tuberculosis in seven patients. The pairs of lanes are numbered by patient number, with the first lane in each pair being the initial isolate and the second the subsequent isolate (the isolates from patient 8 belong to the same cluster as those from patient 7). The isolates for patient 8 were not included and appear the same as patient 7. This was due a problem in cluster 12, where the resolution was too poor. M: Mycobacterium tuberculosis reference strain Mt14323 marker.
Epidemiological and clinical characteristics and genotypic classification of eight patients with post-primary pulmonary tuberculosis after previous cure
Isolates from the eight patients with recurrent TB were studied in relation to the complete RFLP database for the 10th health district of Madrid (covering the period 1992–2004 and including 541 patients). It was established that five patients belonged to clusters of strains present in the community (table 4⇓). No matching strains were identified in the database for the remaining patients. Both isolates from the patient showing exogenous re-infection belonged to different clusters; the first strain belonged to a cluster containing only two other strains (the index case and their son), and the second to a cluster with six other strains from a restaurant outbreak. The strains from the four patients showing relapse belonged to three clusters; two (patients 7 and 8) were brothers and belonged to a long-standing (12 yrs) cluster containing only their strains, another (patient 3) belonged to a medium-sized cluster (eight patients), and the other (patient 6) to a large (14 patients) long-standing (11 yrs) cluster.
Characteristics of the clusters to which the eight recurrent tuberculosis patients belonged
DISCUSSION
The possibility of persons previously infected with M. tuberculosis being exogenously re-infected has been debated since the middle of the twentieth century. However, it was supposed that this rarely occurred given the immunity conferred by the initial infection. In the present study, 1.2% of all TB patients experienced a recurrent episode. This percentage is similar to those found in previous studies in areas with a low and moderate incidence of TB, e.g. 1.5% in Northern Italy 8 and 2.4% in Gran Canaria 9, and is slightly lower than found in studies from the USA and Canada (6.8%) 10 and Madrid (7%) 11. Since most patients are monitored closely, this could explain the low percentage of recurrent TB in the 10th health district of Madrid.
The extent to which exogenous re-infection occurs depends upon the prevalence of disease; the higher the prevalence the greater the likelihood of exogenous re-infection 3. Studies from environments with a high incidence produce conflicting evidence, since the proportion of cases attributable to re-infection ranges 12–75% 4, 12–15. On the few occasions where exogenous re-infection has been documented in areas with a low incidence of the disease, it has usually involved a selected population, e.g. alcoholic residents of a homeless shelter or patients with advanced HIV infection 16–19. In the scarce population-based studies, the percentage of exogenous re-infection varies from study to study. In the present study, one of the eight patients exhibited exogenous re-infection; this is on a par with the results of a study from Northern Italy 8, in which it was found in five (16%) of the 32 patients. However, other studies have shown higher rates: 44% in Gran Canaria 9, 33% in Madrid 11 and 24–31% in Texas (USA) 20. These differences compared with the exogenous re-infection rates determined in other studies may be explained by the criteria applied when selecting the patients with TB recurrence, since noncompliant patients were excluded from the present study; furthermore, the rate of patients with mixed infection is difficult to prove, as demonstrated by van Rie et al. 21. Differences in methods can contribute, to varying degrees, to the heterogeneity of the study results. It is very important that the same timing and bacteriological definition of recurrence be applied.
Two subjects (patients 3 and 6) who were found to have the disease due to relapse were infected with individual strains that belonged to a cluster circulating within the community during these patients’ respective disease-free intervals 22. Another two (patients 7 and 8), who were brothers and belonged to the same long-standing cluster, were considered to have had their disease re-activated. It is possible that some of these patients had contracted a new exogenous infection with the same strain. The present results may thus underestimate the extent of exogenous re-infection. It is, therefore, considered necessary to continue with the present study.
There are no empirical data reflecting the changes in the level of immunity following primary infection, but it is assumed that re-infection is rare in immunocompetent persons during the first 2–5 yrs following first infection 4. In the present study, the only patient exhibiting exogenous re-infection (patient 5) was an immunocompetent person, and there were 6 yrs between the two episodes. Unlike in other studies 23, 24, this patient only reported a history of alcohol abuse. These results suggest that re-infection and progression to active disease is possible once treatment has been discontinued in immunocompetent persons living in an area with a moderate incidence of TB. The majority of the present cases of relapse tended to occur 4 yrs after the previous episode had been cured. However, two patients, one with HIV infection and the other with severe underlying lung disease, suffered reactivation at 16 and 9 months, respectively.
In the present study, significant differences were found between the recurrent and nonrecurrent groups in the distribution of drug and alcohol abuse, HIV infection, smoking and chest radiographic results showing a cavitary lesion. Despite the present study being limited to a small number of patients with recurrent TB, these risk factors might be taken into account during follow-up treatment and when reviewing TB control strategies.
The controversy with regard to the endogenous as opposed to exogenous pathogenesis of TB is of importance when planning clinical trials and national TB control programmes. Where episodes of pulmonary TB following previous cure are the result of exogenous re-infection, the effectiveness of the drug regimen cannot be evaluated on the basis of the relapse rate without the additional information provided by RFLP analysis of bacterial isolates. In the evaluation of national TB control programmes for a specific area, RFLP analysis can be used to evaluate the effectiveness of the treatment regimens currently used.
In conclusion, the present data seem to confirm the fact that re-infection is possible among people in developed countries, but at a lower rate than in high-risk areas. Relapse of a previous infection remains the more probable cause of recurrence in the 10th health district of Madrid. However, this scenario could change in the future, on the basis of social, microbiological and epidemiological factors. Re-infection may be a major contributor to the overall rate of TB in adults in immigrant populations from high-risk areas in particular, especially those living in poor socioeconomic conditions. These events should be considered when planning clinical trials and national tuberculosis control programmes.
Acknowledgments
The authors would like to thank A. Hiess for revision of the English in this manuscript.
- Received January 15, 2007.
- Accepted April 30, 2007.
- © ERS Journals Ltd
References










