





Abstract
Aspirin-induced asthma (AIA) is associated with increased production of cysteinyl leukotrienes (CysLT). Although leukotriene CysLT1-receptor antagonists improve lower airway outcomes in AIA, their effects and dose-response in the upper airway is less well documented.
The present study evaluated the dose-response for montelukast (ML) against nasal lysine-aspirin challenge in patients with AIA.
A total of 12 patients with a clear-cut history of AIA were randomised in double-blind cross-over fashion to receive single doses of ML 10 mg, ML 40 mg, or placebo (PL), with nasal lysine-aspirin challenge performed 12 h after dosing. Measurements of peak nasal inspiratory flow (PNIF), nasal blockage visual analogue scale (VAS) and forced expiratory volume in one second (FEV1) were made over 120 min after nasal lysine-aspirin challenge.
Prechallenge values for mean±sem PNIF (L·min−1) were not significantly different comparing all groups: ML 10 mg (132±10), ML 40 mg (125±12) and PL (132±11). There was no significant difference comparing the maximum % PNIF fall from baseline between screening (46±6) and PL (45±6). The maximum % PNIF fall from baseline was significantly greater with PL (45±6) compared to either ML 10 mg (34±6) or ML 40 mg (32±5). There was also a significantly greater mean % PNIF response over 120 min after lysine-aspirin challenge for PL (26±7) compared to either ML 10 mg (14±6) or ML 40 mg (17±6). There were no significant differences for the maximum or mean % PNIF fall from baseline comparing ML 10 mg and ML 40 mg. A significant increase in nasal blockage VAS score was observed between baseline and 60 min or 120 min with PL but not with ML 10 mg or ML 40 mg. There were no significant differences for either the maximum or mean % FEV1 over 120 min as change from baseline comparing all groups.
A single 10 mg dose of montelukast partially protected against the local effects of nasal lysine-aspirin challenge, with no further benefit at 40 mg. Nasal lysine-aspirin challenge appeared to be a reproducible and safe method in assessing patients with aspirin-induced asthma.
- Aspirin-induced asthma
- cysteinyl leukotrienes
- montelukast
- nasal blockage visual analogue scale
- nasal-lysine aspirin challenge
- peak nasal inspiratory flow
This study was supported by a University of Dundee departmental grant from the Anonymous Trust and received no support from the pharmaceutical industry.
Aspirin-induced asthma (AIA) is a syndrome precipitated by ingestion of aspirin and nonsteroidal anti-inflammatory drugs 1. AIA is characterised by the presence of chronic rhinosinusitis, nasal polyposis, and asthma, associated with eosinophilic mucosal inflammation 2 and overproduction ofcysteinyl leukotrienes 1, 3–8. The mechanism of AIA is thought to be due to an accelerated depletion of prostaglandin E2 by aspirin, the former already downregulated because of cyclooxygenase COX‐2 functional deficiency 1. AIA may affect up to 10% of adults with asthma 9 and is frequently preceded by chronic rhinosinusitis and nasal polyposis 1, 10.
Nasal lysine-aspirin challenge had been proposed as a safe test to diagnose AIA, and is without risk of bronchospasm sometimes associated with bronchial aspirin challenge 10. Moreover, nasal provocation with lysine-aspirin may be safer and preferable compared to oral aspirin challenge, the latter being potentially hazardous, especially in patients with a history of aspirin-induced anaphylaxis. Leukotriene receptor antagonists (LTRA), which competitively block CysLT1-receptors 11–13, have been shown to improve lower airway parameters in patients with AIA 14–16. However, the effect of LTRA in the upper airway are poorly characterised in AIA, particularly with respect to nasal lysine-aspirin challenge. It also remains unclear whether patients with AIA may benefit from a higher than conventional dose of LTRA, in view of the increased production of cysteinyl leukotrienes. Therefore, an evaluation of the dose-response for montelukast (ML) in patients with AIA, against nasal lysine-aspirin challenge was undertaken.
Methods
Patients
Selected patients were required to exhibit a clear-cut history of AIA, with the presence of chronic rhinosinusitis, nasal polyposis, asthma, and aspirin sensitivity, in addition to a positive response to nasal lysine-aspirin challenge. Patients had evidence of chronic sinus inflammation on computed tomography scanning and the presence of grade 1–2 nasal polyps were determined via nasal endoscopy. Patients with occlusive grade 3 nasal polyps were excluded, as significant nasal obstruction would have prevented proper measurement of their peak nasal inspiratory flow (PNIF). In order to confirm sensitivity to aspirin, patients were required at screening todemonstrate a positive response to nasal lysine-aspirin challenge, as defined by a maximal fall in PNIF of ≥25% from baseline over a 120‐min period after challenge. Patients stopped any concomitant LTRA during a 1‐week washout period prior to the initial screening challenge, and for the duration of the study. Patients were also required to withhold any short-acting β2‐agonists and long-acting β2‐agonists for ≥6 h and 48 h respectively, prior to each study visit. All patients gave informed consent and the study was approved by the Tayside Committee on Medical Research Ethics.
Study design
The study was conducted in a randomised, double-blind, placebo (PL)-controlled, cross-over fashion. Patients were randomised to receive a single dose of ML 10 mg (Singulair®, Merck Sharp & Dohme Ltd, Hoddesdon, UK), ML 40 mg, or PL. All tablets were encapsulated and were identical in external physical appearance. Patients took the study capsules at 22:00 h and attended the department the next morning at 10:00 h. There was a 1‐week washout period between each study visit.
Measurements
Nasal endoscopy
Subjects with a significant degree of nasal septal deviation of >50% and occlusive grade 3 nasal polyposis were excluded by nasal endoscopy using a rigid 30° Hopkins® Telescope (Karl Storz Endoscopy Ltd, Slough, UK).
Peak nasal expiratory flow
All patients received appropriate instructions and were required to demonstrate good technique in recording their PNIF using the In-Check® PNIF meter (Clement Clarke International Ltd, Harlow, UK) at the initial screening visit. The technique was then further reassessed and reinforced, prior to each nasal challenge, at each study visit.
Spirometry
Spirometry was performed according to the American Thoracic Society criteria 17 using a Vitalograph® compact spirometer (Vitalograph Ltd, Buckingham, UK) with a computer-assisted pneumotachograph head and pressure transducer. The spirometer was calibrated daily with a Vitalograph® 1 L‐precision syringe.
Nasal lysine-aspirin challenge
Nasal lysine-aspirin challenge was performed as previously described 18. In brief, patients were challenged with 25 mg of lysine-aspirin (Aspisol®, Bayer Plc, Newbury, UK) in each inferior turbinate, and had measurements of PNIF and spirometry at 10‐min intervals, over a 120‐min period after challenge. Patients also had recording of nasal blockage symptoms prior to challenge, and at 60 min and 120 min after challenge, using a visual analogue scale (VAS) ranging from 0 (no symptoms) to 10 (very severe symptoms).
Statistical analysis
The primary outcome variable was calculated as the maximum % PNIF fall from baseline over 120 min after nasal lysine-aspirin challenge. The power of the study was 80% with an α-error set at 0.05 (2‐tailed) in order to detect a 25% difference in the maximum response between ML and PL, with a sample size of 12 completed patients in a cross-over design. Secondary outcomes included the average response over 120 min, as well as the nasal blockage VAS score at 60 min and 120 min after challenge. Analysis of variance was used to compare the response to randomised treatments followed by Bonferroni-corrected multiple-range testing set at 95% CI. In addition, data were analysed according to sequence of randomised treatments in order to evaluate any potential carry-over effects.
Results
Patients
A total of 12 patients (five male and seven female) with a mean±sem age of 48±3 yrs were enrolled and all completed the study. All patients were receiving therapy for AIA including inhaled corticosteroids (ICS) (beclomethasone dipropionate: n=3; budesonide: n=2; and fluticasone propionate: n=3), intranasal corticosteroids (fluticasone propionate: n=12), LTRA (n=6), long-acting β2‐agonists (n=1) and short-acting β2‐agonists (n=12). The daily dose of ICS (1,225±358 µg) and intranasal corticosteroids (600±60 µg) remained unchanged throughout the study.
Lysine-aspirin challenge reproducibility
In order to determine the consistency of the nasal response to lysine-aspirin, separate challenges were performed at screening and following PL (fig. 1⇓). There was no significant difference comparing the maximum % PNIF fall from baseline between screening (46±6) and PL (45±6). The coefficient of variation for the reproducibility of the lysine-aspirin challenge was 4.2%.
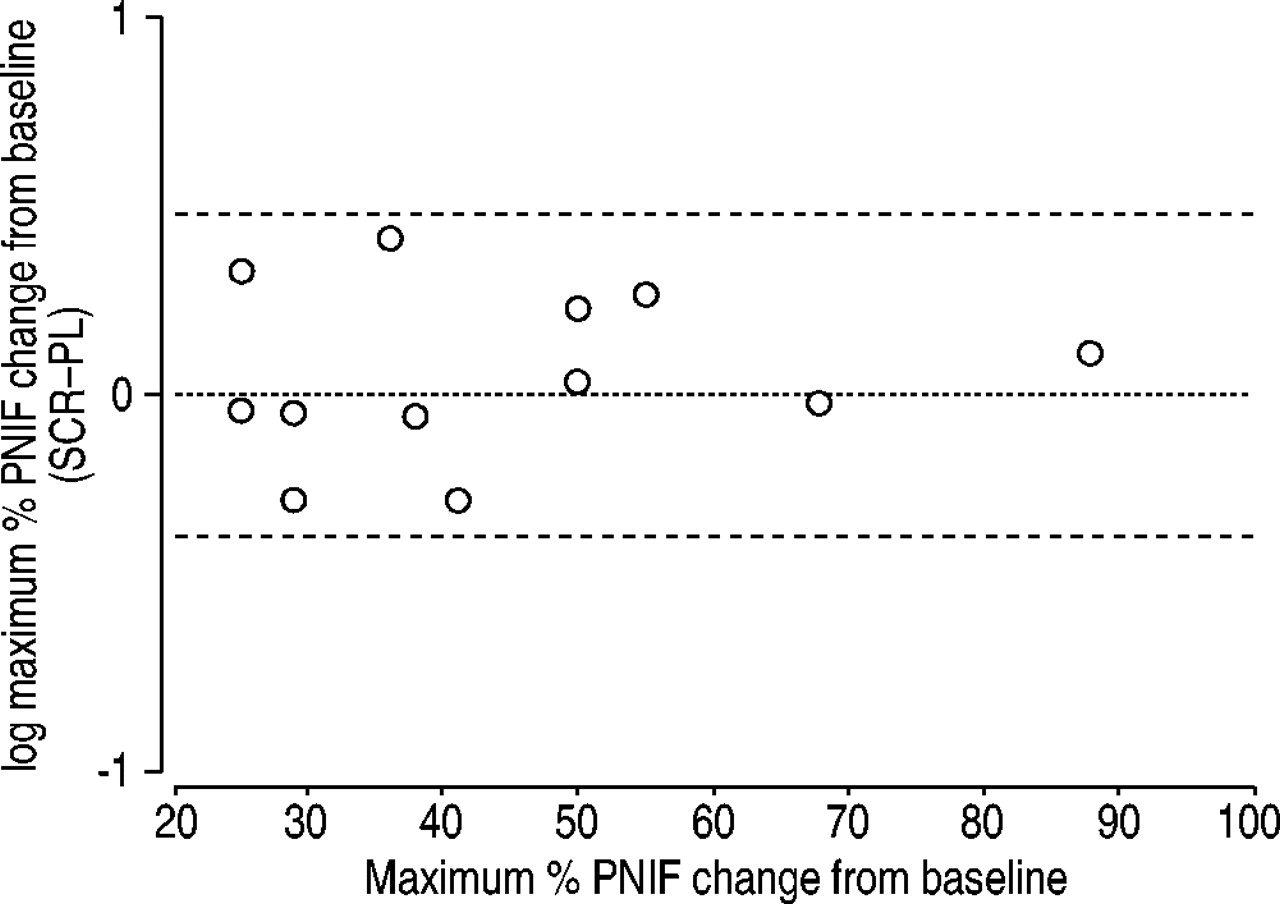
Bland and Altman plot for the maximum percentage (%) peak nasal inspiratory flow (PNIF) change from prechallenge baseline. The middle line indicates the point of no difference between screening (SCR) and placebo (PL), and the dashed lines indicate the 95% CI.
Peak nasal expiratory flow
Prechallenge PNIF (L·min−1) was not significantly different comparing all groups: ML 10 mg (132±10, mean±sem), ML 40 mg (125±12) and PL (132±11). The maximum % PNIF fall from baseline (fig. 2⇓) was significantly greater (p<0.05) with PL (45±6) compared to either ML 10 mg (34±6; mean difference: 12 (95% CI: 4–21)), or ML 40 mg (32±5; mean difference: 13 (95% CI: 2–24)). The average % PNIF fall from baseline over 120 min (fig. 3⇓) was also significantly greater (p<0.05) with PL (26±7) compared to either ML 10 mg (14±6; mean difference: 13 (95% CI: 4–21)), or ML 40 mg (17±6; mean difference: 10 (95% CI: 1–19)). There were no significant differences for both the maximum or average % PNIF fall from baseline over 120 min, comparing ML 10 mg and ML 40 mg. Individual data showed no discernible pattern of any dose-response effect between ML 10 mg and ML 40 mg (fig. 2⇓). Data for absolute PNIF values over 120 min after nasal lysine-aspirin challenge are also shown (fig. 3⇓). There were no significant differences for any outcome variable when data were analysed according to the sequence in which the randomised treatments were given, thus indicating the absence of any carry-over effect.
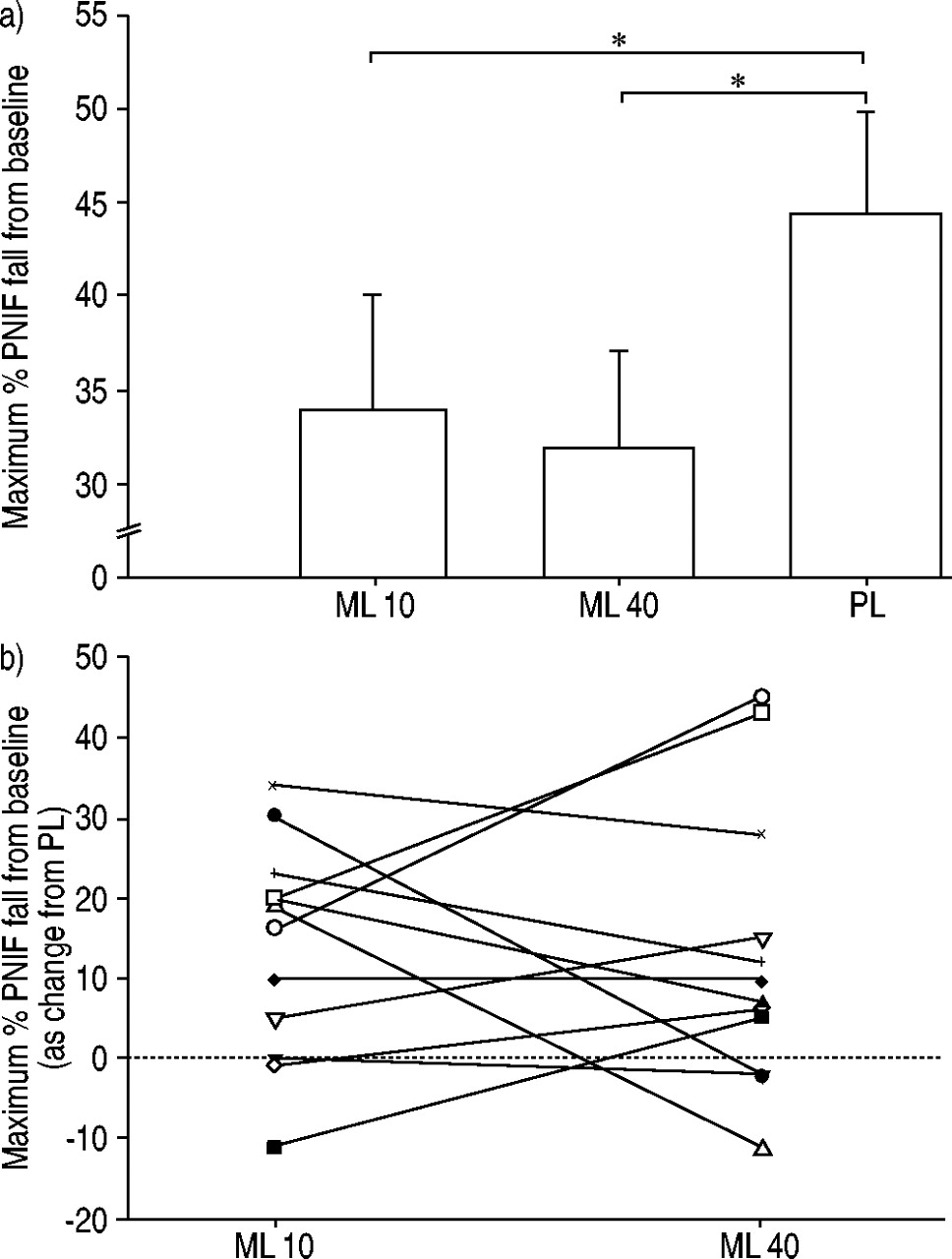
a) Mean±sem maximum percentage (%) peak nasal inspiratory flow (PNIF) fall from prechallenge baseline for montelukast 10 mg (ML 10), montelukast 40 mg (ML 40) and placebo (PL); b) Individual data for maximum % PNIF fall from prechallenge baseline, as change from PL, showing ML 10 and ML 40 values coupled for each individual. *: p<0.05.

a) Time-response profile of percentage (%) peak nasal inspiratory flow (PNIF) change from prechallenge baseline after nasal lysine-aspirin challenge, and mean±sem % PNIF fall from prechallenge baseline over 120 min (AV); b) time-response profile of absolute PNIF values after nasal lysine-aspirin challenge over 120 min. *: p<0.05 between placebo (▾) and montelukast 10 mg (•) or montelukast 40 mg (○).
Nasal blockage visual analogue scale score
In the PL group, nasal blockage VAS score (fig. 4⇓) compared to baseline (1.3±0.5) was significantly greater (p<0.05) at both 60 min (2.7±0.8; mean difference: 1.3 (95% CI: 0.2–2.4)) and 120 min (3.1±0.9; mean difference: 1.8 (95% CI: 0.4–3.1)). There were no significant differences comparing 60 min or 120 min and baseline in both the ML 10 mg and ML 40 mg group. The change from baseline was significantly greater (p<0.05) at 120 min for PL (1.8±0.6) compared to ML 40 mg (0.5±0.4; mean difference: 1.2 (95% CI: 0.1–2.4)).

Mean±sem nasal blockage visual analogue scale score at prechallenge baseline (□), and at 60 (└) and 120 ( ) min after nasal lysine-aspirin challenge. ML 10: montelukast 10 mg; ML 40: montelukast 40 mg; PL: placebo.
) min after nasal lysine-aspirin challenge. ML 10: montelukast 10 mg; ML 40: montelukast 40 mg; PL: placebo.
Forced expiratory volume in one second
Prechallenge FEV1 was not significantly different comparing all groups: ML 10 mg (2.71±0.24 L), ML 40 mg (2.82±0.28 L) and PL (2.73±0.27 L). There were no significant differences for either the maximum or average % FEV1 over 120 min as change from baseline comparing all groups (fig. 5⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time-response profile of percentage (%) FEV1 change from prechallenge baseline after nasal lysine-aspirin challenge. ▾: placebo; •: montelukast 10 mg; ○: montelukast 40 mg.
Discussion
The present study results show that ML partially attenuated the local response to nasal lysine-aspirin challenge in patients with AIA. Moreover, the presented data have also demonstrated that nasal lysine-aspirin challenge is both reproducible and safe when used to assess patients with AIA. ML protected against the effects of lysine-aspirin by attenuating lysine-aspirin induced nasal obstruction, measured objectively with PNIF and subjectively using nasal blockage VAS score.
The current results would suggest a plateau in the dose-response for ML at 10 mg, which is the conventional recommended dose 19. This is perhaps surprising given the overproduction of cysteinyl leukotrienes in AIA 1, 3–8. The effects of ML were observed as add-on therapy to intranasal corticosteroids, the latter being unchanged throughout the study. This was expected as corticosteroids have been shown to have little effect on the biosynthesis of cysteinyl leukotrienes 20.
FEV1 remained virtually unchanged throughout the lysine-aspirin challenge in the present study, suggesting that lysine-aspirin-induced nasal obstruction in the upper airway does not influence the lower airway to trigger bronchoconstriction. This is reassuring given that 25% of patients in the current study have previously reported severe systemic reactions following ingestion of aspirin leading to angio-oedema and severe bronchospasm, requiring hospitalisation. The remaining patients had a history of severe bronchospasm following ingestion of aspirin but no angio-oedema.
A maximal fall in PNIF of ≥25% from baseline was chosen in order to indicate a positive response to nasal lysine-aspirin, in keeping with previous data showing similar cut-off value using acoustic rhinometry 18. PNIF has been shown to be a more sensitive measurement compared to either acoustic rhinometry or rhinomanometry, when used with nasal histamine challenge 21. In addition, PNIF has also been found to have a low degree of intra-individual variability of 8% for repeated measurements over the short-term in patients with allergic rhinitis 22.
The presented data would suggest a potential role for MLin attenuating the nasal response induced by aspirin in patients with AIA, although prospective placebo-controlled randomised chronic dosing studies are required to properly evaluate objective and subjective responses. In an open audit study, ML was found to produce variable responses in patients with nasal polyposis, with no difference in subjective response between aspirin tolerant and intolerant patients 23. However, as ML has been shown to benefit aspirin intolerant patients with asthma, it would seem rational that ML may also benefit patients with concomitant chronic rhinosinusitis and nasal polyposis. It is conceivable that the present study may have missed a difference in the nasal response between the doses of ML as there is sometimes a prolonged response after aspirin challenge, which is attributable to the influx of inflammatory cells. Moreover, although ML protected against the effects of nasal lysine-aspirin in the current study, it did not completely obliterate the response. This would be in keeping with a previous observation showing ML to be only partially effective in altering the response to oral aspirin challenge 24. As there are multiple mediators involved in the pathogenesis ofAIA, the partial protection observed with ML would indicate a lack of antagonism of other receptors, such as prostaglandin PGD2-receptors and histamine H1-receptors.
In conclusion, montelukast at a clinically recommended dose of 10 mg partially protected against the local effects of nasal lysine-aspirin challenge, which in turn appears to be areproducible and safe method in assessing patients with aspirin-induced asthma. There was no benefit attained by increasing the dose of montelukast to 40 mg.
- Received September 4, 2003.
- Accepted March 9, 2004.
- © ERS Journals Ltd
References









