





Abstract
The atypical respiratory pathogens Chlamydia pneumoniae, Mycoplasma pneumoniae and Legionella pneumophila are now recognised as a significant cause of acute respiratory-tract infections, implicated in community-acquired pneumonia, acute exacerbations of chronic bronchitis, asthma, and less frequently, upper respiratory-tract infections.
Chronic infection with C. pneumoniae is common among patients with chronic obstructive pulmonary disease and may also play a role in the natural history of asthma, including exacerbations. The lack of a gold standard for diagnosis of these pathogens still handicaps the current understanding of their true prevalence and role in the pathogenesis of acute and chronic respiratory infections.
While molecular diagnostic techniques, such as polymerase chain reaction, offer improvements in sensitivity, specificity and rapidity over culture and serology, the need remains for a consistent and reproducible diagnostic technique, available to all microbiology laboratories.
Current treatment guidelines for community-acquired pneumonia recognise the importance of atypical respiratory pathogens in its aetiology, for which macrolides are considered suitable first-line agents. The value of atypical coverage in antibiotic therapy for acute exacerbations of chronic bronchitis and exacerbations of asthma is less clear, while there is no evidence to suggest that atypical pathogens should be covered in antibiotic treatment of upper respiratory-tract infections.
The term “atypical pathogen” most commonly refers to Chlamydia pneumoniae, Mycoplasma pneumoniae and Legionella pneumophila. Once believed to be of little clinical significance, a wealth of data accumulated over the past decade suggests that these are important respiratory pathogens in a wide range of respiratory-tract infections (RTIs) and are capable of causing severe, as well as mild-to-moderate, illness.
Although the role of atypical pathogens 1, and of C. pneumoniae in particular 2, has been reviewed previously, there has been little focus on appropriate coverage of these pathogens in treatment decisions for patients with RTIs. In addressing this issue, this review examines the role of atypical pathogens in the aetiology of upper and lower RTIs, in both adults and children, and discusses the value of appropriate coverage of these pathogens in empirical antibiotic prescribing.
Organisms
Chlamydia pneumoniae
C. pneumoniae, an obligate intracellular bacteria, was first recognised as a respiratory pathogen in 1986 3 (fig. 1⇓). It was originally known as TWAR; a name derived from the first C. pneumoniae isolate TW-183T, obtained in 1965 from a conjunctival swab, and AR-39, the first pharyngeal isolate 4.
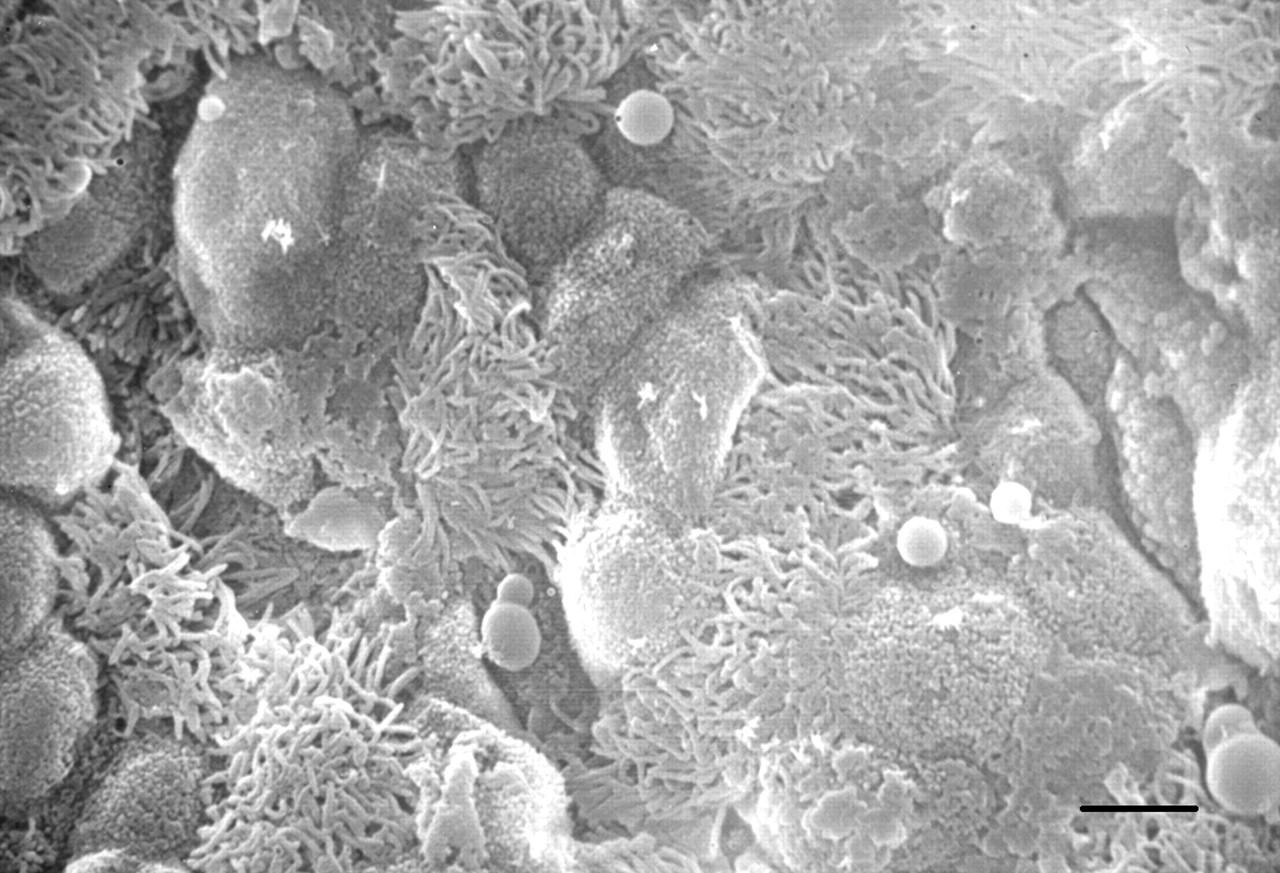
Scanning electron microscopy of the epithelial layer of the trachea from mice after infection with Chlamydia pneumoniae. Scale bar=10 µm.
Since its identification in the late 1980s, C. pneumoniae has emerged as the most common nonviral intracellular human respiratory pathogen 5–7 and an important cause of acute and chronic infection of the upper and lower respiratory tract in both immunocompetent and immunocompromised hosts 5. Among patients with community-acquired pneumonia (CAP), C. pneumoniae is one of the more common aetiological agents 1.
Legionella pneumophila
Legionellae are intracellular Gram-negative, aerobic bacilli that can replicate in respiratory monocytic cells. At least 48 species of Legionella, comprising 70 distinct serogroups, have been identified, of which L. pneumophila is responsible for themajority of cases of legionellosis, the clinical syndrome associated with Legionella sp. infection 8. Legionellosis consists of two distinct clinical entities: Legionnaire's disease, a severe and potentially fatal form of pneumonia, and Pontiac fever, a self-limiting acute febrile illness 8.
Legionnaire's disease was first described in 1977, following a major outbreak of pneumonia among members of the American Legion attending a convention in Philadelphia the previous year 9. It has since been recognised as an important aetiological agent of CAP, responsible for both sporadic and large-scale outbreaks 8.
Mycoplasma pneumoniae
As the first of the atypical pathogens to be identified as a cause of RTI, for many years M. pneumoniae was known as the Eaton agent, after Eaton et al. 10 identified this pleuropneumonia-like organism from the sputum of patients with “primary atypical pneumonia” in 1944. It was subsequently renamed M. pneumoniae and identified as a common cause of respiratory disease in man 11. Of the many species of Mycoplasma known to infect man, M. pneumoniae is the only one that causes RTIs 12.
Identification
For the majority of RTIs, an aetiological diagnosis is never established. In the case of lower RTIs, sputum, and to a lesser extent pleural fluid and bronchoalveolar aspirates, are often contaminated with indigenous bacterial flora. Furthermore, once a sample has been collected, the laboratory tests are often slow, insensitive and laborious. This is especially true with the identification of atypical intracellular pathogens, for which culture and serology have traditionally been employed for diagnosis. Similarly, in the case of upper RTIs, swab samples are often contaminated. Other diagnostic techniques, such as tympanocentesis, may not always be appropriate for paediatric patients or in the outpatient setting.
The variable sensitivity and specificity of currently available tests make diagnosis of an acute infection unreliable, and compromise the reliability of prevalence data based on paired sera. Diagnosis protocols developed in the research laboratory may not translate well to clinical practice, where clinical samples from the patient population are much more diverse, and where financial support and technology may not be comparable 13. In addition, species such as C. pneumoniae have emerged relatively recently as an important cause of RTI and were not investigated until a short time ago.
Nonetheless, as the recent guidelines from the Infectious Disease Society of America (IDSA) have emphasised, an aetiological diagnosis can be useful for prognostic and therapeutic purposes, as well as advancing current knowledge of epidemiologically important pathogens 14. A definitive diagnosis for example, allows antibiotic therapy to be targeted against particular pathogens, rather than being purely based on empirical selection. This has implications for infections due to the intracellular atypical respiratory pathogens Chlamydia and Legionella, and for Mycoplasma, which lacks a conventional cell wall and is thereby refractory to treatment with β‐lactam antibiotics. Penicillins and cephalosporins are also unable to penetrate inside cells, a prerequisite for efficacy against obligate intracellular pathogens, such as C. pneumoniae and L. pneumophila.
However, new techniques are emerging with the promise of more rapid and reliable identification of atypical pathogens. A microimmunofluorescence assay for the identification of C.pneumoniae infection has shown that the antibody response to an acute primary infection is characterised by a rise in immunoglobulin (Ig)M titre, followed by increases in IgG, whereas in cases of re-infection, only IgG and IgA antibody titres increase. Within 2–3 months of an acute infection, IgM levels are no longer detectable, but persistent levels of IgG and IgA antibody suggest evidence of persistent or chronic C.pneumoniae infection 5.
Molecular techniques, such as polymerase chain reaction (PCR), hold more promise for diagnosis, and may offer advantages in rapidity, sensitivity and specificity over conventional culture and serology 13. The technique has already been successfully applied to the rapid identification of C.pneumoniae, M. pneumoniae and L. pneumophila in respiratory secretions 13. However, while PCR is emerging as one of the most accurate methods for the rapid identification of atypical respiratory pathogens, much work remains in developing PCR assays that can be readily adopted by routine diagnostic laboratories 13. Unlike microbiological testing, diagnosis with PCR has a limited ability to test antimicrobial susceptibility and does not provide an isolate archive, should further testing be necessary. Also, reproducibility may be difficult to achieve outside the research laboratory, since clinical samples are frequently from diverse patient populations, necessitating adjustment of PCR protocols with regard to sample preparation and amplification conditions. Furthermore, positive results may not distinguish between colonisation and infection 13.
In vitro susceptibility
Although the β‐lactams are ineffective against atypical respiratory pathogens, several classes of commonly used antibiotics possess in vitro activity against C. pneumoniae, M.pneumoniae and L. pneumophila, including the macrolides, fluoroquinolones, tetracyclines and ketolides.
Macrolides exhibit excellent in vitro activity against atypical respiratory pathogens, and have traditionally been considered drugs of first choice for infections due to atypical pathogens 15–23. Against contemporary isolates of C. pneumoniae, the minimum inhibitory concentration minimal inhibitory concentration of 90% bacteria values of the macrolides (erythromycin, roxithromycin, clarithromycin and azithromycin) are typically in the range of 0.016–0.5 mg·L−1 15, 21, 22, 24, 25. Macrolides are especially potent against strains of M. pneumoniae, with recent studies showing MIC90 values of 0.0019, 0.0019 and 0.0039 mg·L−1 for erythromycin, clarithromycin and roxithromycin respectively 19, and of <0.0005 mg·L−1 for azithromycin 15. The newer macrolides tend to exhibit greater in vitro activity against L. pneumophila than do the older agents, such as erythromycin 20. Against 85 isolates of L. pneumophila serogroup 1, the MIC90 values were 0.06 mg·L−1 for clarithromycin, 0.5 mg·L−1 for azithromycin and 1 mg·L−1 for erythromycin 17.
The fluoroquinolones also exhibit good in vitro activity against atypical respiratory pathogens 15–20, 22, 26. This class includes traditional agents, such as ciprofloxacin and ofloxacin, along with the newer respiratory fluoroquinolones (levofloxacin, gatifloxacin and moxifloxacin) and several investigational agents, such as gemifloxacin and garenoxacin. Against C. pneumoniae, the newer fluoroquinolones appear more potent than earlier derivatives, with MIC90 values forciprofloxacin typically ∼1 mg·L−1 as compared with: 0.25–0.5 mg·L−1 for levofloxacin; 0.06 mg·L−1 for moxifloxacin and gemifloxacin; and 0.007 mg·L−1 for garenoxacin 16,22, 24–26. Newer fluoroquinolones, such as levofloxacin, are active in vitro against clinical isolates of M. pneumoniae, with MIC90 values of 0.125–0.25 mg·L−1 similar to tetracyclines, but inferior to macrolides 15, 19. They are, however, highly potent agents against L. pneumophila. Against 85 isolates of L. pneumophila serogroup 1, MIC90 values ranged from 0.016 mg·L−1 for levofloxacin, moxifloxacin, grepafloxacin and gemifloxacin, to 0.03 mg·L−1 for ciprofloxacin and ofloxacin 17.
Tetracyclines may also be used to treat infections caused by C. pneumoniae and M. pneumoniae. However, their in vitro potency is often inferior to that of the macrolides and fluoroquinolones 15, 16, 19, 23. Furthermore, there is evidence to suggest that strains of M. pneumoniae are developing resistance to tetracycline 23.
Chemically related to the macrolides, the ketolides are the most recent class of antibiotics to be developed for the treatment of RTIs and include the investigational agents telithromycin and ABT-773. They share the potent in vitro activity of the macrolides against atypical respiratory pathogens 20, 21, 25. Against strains of C. pneumoniae, the MIC90values of telithromycin and ABT-773 are typically 0.06 mg·L−1 (range: 0.015–0.25 mg·L−1) and 0.015 mg·L−1 (range: 0.008–0.15 mg·L−1), respectively 21, 25. ABT-773 shows similar in vitro activity to azithromycin against L. pneumophila, exhibiting MIC90 values of 0.015 and 0.03 mg·L−1, respectively 20.
Community-acquired pneumonia
Prevalence
The failure to identify the causative pathogens, in as many as 50% of patients with symptoms of CAP, has made it difficult to determine its true microbial aetiology and, in particular, the causative role of atypical pathogens, since the observed prevalence rates are dependent on the diagnostic tests used 27. Furthermore, some patients with CAP have mixedinfections involving typical respiratory pathogens, e.g. as Streptococcus pneumoniae, Haemophilius influenzae and Moraxella catarrhalis, as well as atypical pathogens, which cannot be diagnosed initially with readily available clinical specimens.
While S. pneumoniae is still considered the major cause of CAP, surveys suggest that atypical respiratory pathogens are an increasingly frequent cause of illness, accounting for anything from 6–20% of ambulatory cases to ≥40% among patients hospitalised for CAP (table 1⇓) 1, 27, 28,. Other authors have estimated the contribution of atypical pathogens as 25% in Europe 42 and 22% in the USA 43.
Prevalence of atypical respiratory pathogens (Chlamydia pneumoniae, Mycoplasma pneumoniae and Legionella spp.) in patients with community-acquired pneumonia (CAP)
Children are among those at high risk of contracting CAP due to infection with C. pneumoniae or M. pneumoniae 44, and studies suggest that incidence is age-related 45, 46. In one study, the incidence of C. pneumoniae was two-fold higher in children ≥5 yrs old than in those <5 yrs old 45. In a separate study, in which the aetiology of CAP was determined in paediatric outpatients using a complete panel of diagnostic tests, C. pneumoniae was identified in 6% of patients aged between 6 months and 12 yrs, ranking behind S. pneumoniae (27%), viruses (20%) and M. pneumoniae (7%) 47.
Elderly patients and those with comorbid cardiopulmonary diseases are also at increased risk of CAP due to C. pneumoniae, in whom the infection may develop into severe pneumonia 48, 49. A survey, conducted among 101 elderly patients hospitalised for CAP, showed that infection with C. pneumoniae was second only to S. pneumoniae in frequency, when identified in 21% of patients with an aetiological diagnosis 50.
Legionellae have consistently been identified as a common cause of severe CAP, but their role in mild-to-moderate illness remains controversial 51. Certainly, Legionella spp. are isolated with increasing frequency in patients with severe symptoms of pneumonia, and in many studies are the second highest cause of severe CAP after S. pneumoniae 51. In a recent review of 41 prospective studies which sought to identify the microbial aetiology of CAP, L. pneumophila was identified as the causative pathogen in 1.9% of outpatients, 4.9% of hospitalised patients and 7.9% of intensive care unit patients 52. Other independent studies have also reported a high prevalence of L. pneumophila infection among CAP patients admitted to hospital 31, 32. In one study, 20% of patients hospitalised for CAP had legionellosis 32.
Recent surveys indicate that L. pneumophila remains the primary cause of legionellosis, responsible for over 80% of cases, of which the majority are due to serogroup-1 pathogens 53. The considerable variation in prevalence of L pneumophila, observed at different times in the same location, suggests that infection due to this organism may be a seasonal and epidemic phenomenon 54–57. Among other species recently isolated from patients with CAP, L. longbeachae occurred with a frequency of 3.9%, L. bozemanii with a frequency of 2.4%, and L. micdadei, L. dumoffii, L. feeleii, L. wadsworthii and L. anisa with a combined frequency of 2.2% 53. Interestingly, L. longbeachae constituted 30.4% of clinical isolates in Australia and New Zealand 53.
Legionella spp. are emerging as one of the most common causes of severe CAP, with current figures probably an underestimate of the true prevalence of legionellosis, given that many species and serogroups cannot be identified accurately by contemporary commercial microbiological tests 51.
An Asian epidemiological study determined the frequency of infection with M. pneumoniae, C. pneumoniae and Legionella spp., in patients presenting with symptoms of CAP at 12 medical centres in Asian countries, using standardised laboratory techniques and interpretation criteria (Ngeow etal., Institute for Medical Research,Bacteriology Division, Jalan Pahang, Kuala Lumpur, Malaysia, unpublished data). Aetiological diagnosis was based on seroconversion or significant changes in antibody titre together with the presence of bacterial DNA in respiratory secretions, in the case of M. pneumoniae and C. pneumoniae infections, or bacterial antigen in urine, in the case of L. pneumophila serogroup 1. Results for paired (acute and convalescent) sera from 1,374 patients showed that 23.5% of cases were caused by infection with atypical pathogens, with M. pneumoniae, C. pneumoniae, and L. pneumophila accounting for 12.2%, 4.7% and 6.6% of cases respectively. Persisting high antibody titres, indicative ofpast exposure to M. pneumoniae, C. pneumoniae and L. pneumophila, were seen in 10.2%, 4.8% and 18.9% of patients respectively, reflecting the overall high prevalence (33.9%) of these pathogens in the aetiology of CAP in Asia.
Clinical course of atypical infection
The term “primary atypical pneumonia”, which was used to describe pneumonia due to infection with M. pneumoniae in the late 1930s and early 1940s, is no longer considered appropriate asadiagnosis in patients infected with atypical respiratory pathogens. Indeed, it is now widely recognised that the clinical course of CAP is similar whether caused by typical or atypical respiratory pathogens 29. Therefore, it is unwise to select antibiotic therapy solely on the basis of clinical manifestations, such as fever, chills, productive cough and pleuritic chest pain, or radiological evidence of CAP 58, even when legionellosis is suspected.
Therapy
Given the prevalence of atypical pathogens in the aetiology of CAP and the likelihood that current figures underestimate their true prevalence, empirical antibiotic therapy for CAP should ideally provide coverage against atypical pathogens. Treatment should be based on the premise that all patients with CAP could be potentially infected with C. pneumoniae, M. pneumoniae or Legionella spp., either alone or as part of a mixed infection 27; an approach that is, in fact, advocated in several new treatment guidelines for CAP.
C. pneumoniae is commonly found in infections of mixed aetiology and may predispose to co-infection with other microorganisms, e.g. S. pneumoniae 59. In patients co-infected with C. pneumoniae and S. pneumoniae, the clinical picture isoften more severe than that seen with monomicrobial infection and, as one study showed, can result in prolonged hospitalisation if antibiotic therapy is directed solely to the eradication of S. pneumoniae 60.
The need to provide coverage against atypical pathogens in empirical prescribing for CAP is now recognised in national guidelines, in which macrolides with proven activity against atypical pathogens are widely advocated 14, 27, 61–64. Studies have shown that the inclusion of a macrolide in treatment regimens can improve clinical outcome in children with lower RTIs due to atypical pathogens 65, including those with CAP 66, in whom it is especially difficult to determine the microbial aetiology.
For empirical therapy, the IDSA 14, Center for Disease Control and Prevention 63, Canadian Infectious Disease Society and Canadian Thoracic Society (CIDS/CTS) 64, and the American Thoracic Society (ATS) 27 all recommend macrolides for first-line use in outpatients without modifying factors. The British Thoracic Society 61 and South African Thoracic Society (SATS) 62 guidelines, respectively, support the use of macrolides as an alternative monotherapy in outpatients or as monotherapy when atypical infection is suspected. In outpatients with modifying factors, such as the elderly or those with comorbidity, the ATS 27 and CIDS/CTS 64 suggest macrolides are used in conjunction with other antibiotics. The inclusion of macrolides in combination regimens is also widely advocated for patients hospitalised with CAP. SATS guidelines 62 recommend the use of macrolides as an adjunct to β‐lactams or fluoroquinolones, if atypical infection is suspected.
A number of studies have shown that adherence to guidelines for empirical prescribing in CAP results in significant improvement in clinical outcome 67–71. Treatment consistent with the ATS guidelines 27, for example, in which macrolides are recommended for atypical coverage, has been shown to significantly reduce length of hospitalisation as well as mortality from CAP 67, 69, 70.
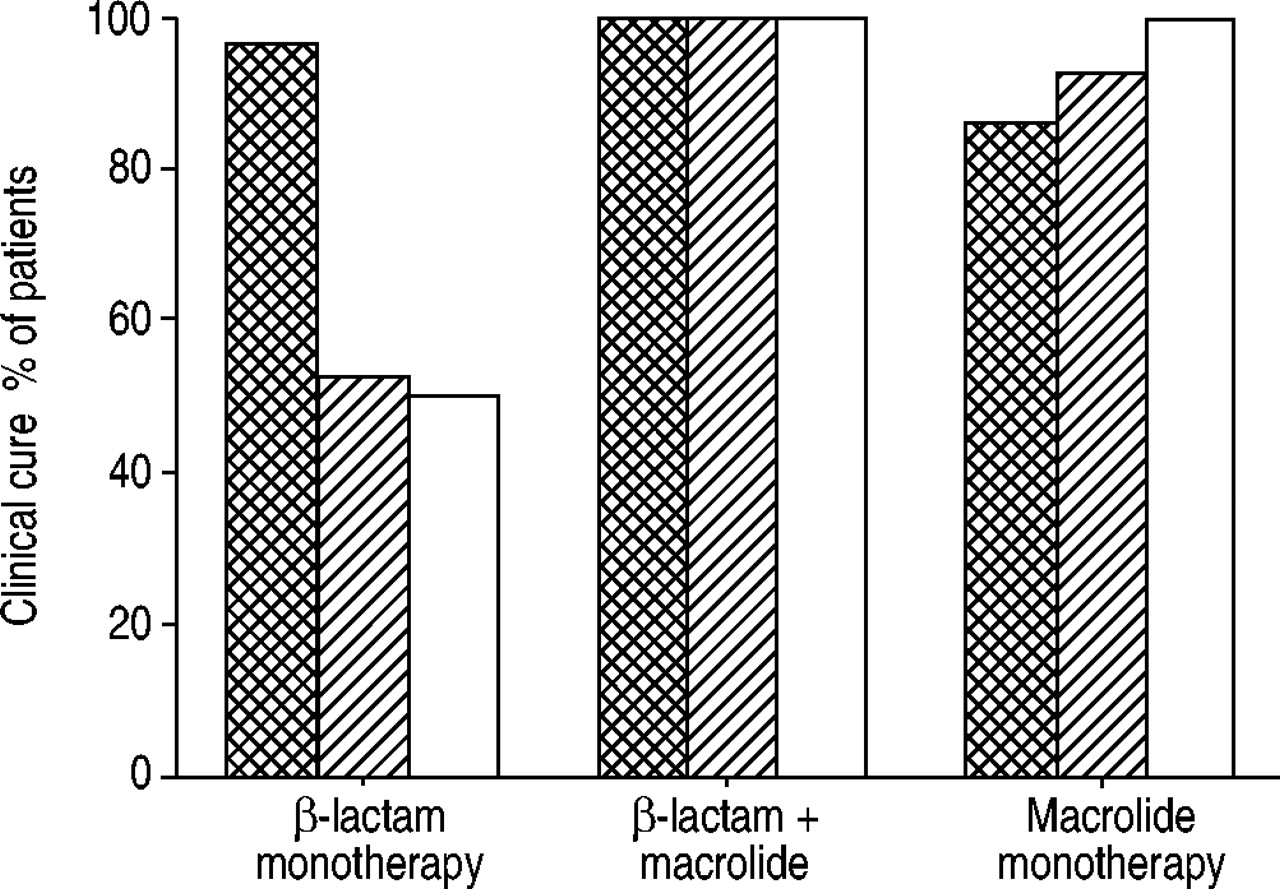
Recently published data have confirmed the prevalence of atypical pathogens in paediatric CAP patients 66, highlighting their significant role in the pathogenesis of the disease and the need to reassess antibiotic therapy with β‐lactam agents. In 196 children with CAP aged 2–5 yrs, S. pneumoniae infections were diagnosed in 24.5% of patients, atypical bacterial infections in 23.5% of patients, and mixed S. pneumoniae and atypical bacterial infections in 8.2% of children. Clinical, laboratory and radiological features were of limited use in predicting the aetiology of CAP. Clinical failures occurred significantly more frequently 4–6 weeks post-treatment, among children with atypical bacterial or mixed infection who were not originally treated with a macrolide (fig. 2⇓).

Comparison of clinical outcome by type of antibiotic therapy adapted from 56. β‐lactam monotherapy: n=53; β‐lactam monotherapy+macrolide: n=22; macrolide monotherapy: n=26.  : Streptococcus pneumoniae (n=44); └: atypical bacteria (n=42); □: mixed S.pneumoniae +atypical bacteria (n=44).
: Streptococcus pneumoniae (n=44); └: atypical bacteria (n=42); □: mixed S.pneumoniae +atypical bacteria (n=44).
COPD
Prevalence of COPD
Chronic obstructive pulmonary disease (COPD) is a chronic, smoking-related inflammatory disorder of the lungs, in which persistent infection with C. pneumoniae is believed to play a significant role in the underlying pathology 2, 72–74. A hypothetical model has been proposed to describe how chronic C. pneumoniae infection in respiratory-tract tissue may amplify smoking associated inflammation in the bronchi and, hence, contribute to the development of irreversible pathological changes characterised by airway obstruction 74. Certainly, there is evidence to show that chronic colonisation with C. pneumoniae, as assessed by PCR, is significantly associated with impaired lung function 75, and that infection appears much more common in COPD patients than in age-matched controls 72, 75, 76. Chronic infection may also predispose to airway colonisation with other pathogens, and so fuel the vicious cycle of chronic airway inflammation 77.
Prevalence of acute exacerbations of chronic bronchitis
Patients with COPD, the majority of whom have chronic bronchitis, are prone to acute exacerbation in which bacteria are estimated to be responsible for approximately half of all cases 78. H. influenzae, M. catarrhalis, S. pneumoniae and C.pneumoniae are the most important causes of acute exacerbation of bacterial origin 78; although, the incidence of C. pneumoniae in patients with acute exacerbations of chronic bronchitis (AECB) appears to vary considerably from as low as 4–5% to >30% (table 2⇓) 72, 75, 79–84.
Incidence of Chlamydia pneumoniae in patients with acute exacerbations of chronic bronchitis
Therapy
The value of antibiotic therapy in the management of AECB was established in a landmark placebo-controlled trial in 1987, in which 173 patients with AECB, graded according to the presence of the three cardinal symptoms of increased dyspnoea, increased sputum and increased purulence, were treated with trimethoprim-sulphamethoxazole, amoxicillin or doxycycline. Results showed that antibiotic therapy achieved significantly greater rates of clinical success than placebo and that it was most effective in the more severely ill patients 78. A subsequent meta-analysis of nine randomised placebo controlled trials of antibiotic therapy in patients with AECB has confirmed these findings 86.
The early antibiotic trials in AECB generally involved treatment with standard antibiotics, such as oxytetracycline, ampicillin, chloramphenicol, tetracycline, amoxicillin and trimethoprim-sulphamethoxazole, which more recent analyses suggest are less effective than many newer agents that are often reserved for second- or third-line use. In a retrospective analysis of antibiotic therapy for AECB, treatment with amoxicillin/clavulanate, second-generation macrolides, such as azithromycin, and fluoroquinolones significantly reduced the rate of clinical failure, the need for hospitalisation and overall costs, as well as extending the interval between exacerbations compared with older agents 87. Against this evidence, one study showed that of the 80–100% of patients who received antibiotics for AECB, 13–25% experienced clinical failure 88.
Evidence based guidelines, analogous to those for CAP, have yet to be fully developed for AECB, although there have been attempts to classify treatment by baseline severity of disease and severity of exacerbation 89, 90. Where they exist, the guidelines focus primarily on antibiotic coverage of H. influenzae, M. catarrhalis and S. pneumoniae, but also include agents effective against atypical respiratory pathogens. The guidelines from the European Respiratory Society, for example, recognise that atypical pathogens, such as M. pneumoniae and C. pneumoniae, may be implicated in COPD exacerbations and that macrolides, fluoroquinolones and tetracyclines are effective in such cases. These aetiologies, in addition to noninfectious causes, should therefore be taken into consideration when patients with AECB fail to respond to initial therapy 90.
Asthma
Aetiology
Asthma, a chronic inflammatory disease of the airways, is characterised by bronchial constriction together with symptoms of cough, wheezing and difficulty breathing. Its aetiology is complex, involving interactions between genetic susceptibility, exposure to allergens and external aggravating factors, such as smoking, air pollution and RTIs 91. A link between asthma and RTIs was first established in the early 1970s, although at the time it was unclear whether respiratory pathogens were involved in either the initiation or promotion of asthma 92. Acute RTIs are now known to worsen asthma, particularly in children, in whom they account for between 14–45% of acute exacerbations 93. Although the incidence of RTIs in adult asthma patients was always believed to be lower, a recent study found that 37% of adults admitted to hospital over a 12‐month period with an acute asthma exacerbation had evidence of recent RTI 93. These findings suggest that RTIs may precipitate a worsening of asthma in adults as well as children.
Role of atypical pathogens
Of nonviral pathogens implicated in asthma, infection with M. pneumoniae and C. pneumoniae has been linked to a worsening of asthma. Evidence from in vitro animal studies indicates that atypical respiratory pathogens may play a role in the pathogenesis of the disease 92. Mice infected with M.pneumoniae, for example, can develop a chronic pulmonary infection characterised by airway hypersensitivity, airway obstruction and histological inflammation, which lends support to the notion that M. pneumoniae infection may cause chronic pulmonary disease with functional airway obstruction, as seen in asthma patients 94.
There is some clinical evidence to suggest that acute infection with C. pneumoniae and M. pneumoniae might initiate asthma in some previously asymptomatic patients, although the quantitative role of these atypical pathogens in this role is unknown 91, 95, 96. Furthermore, infection with C. pneumoniae may interact with allergic inflammation to increase asthma symptoms 97–99. A causal link has been established between repeated or prolonged exposure to C. pneumoniae and wheezing, asthmatic bronchitis and asthma 100, as well as to acute episodes of wheezing in children with asthma 101. C. pneumoniae has also been associated with persistent cough 102–104.
Exacerbations
Evidence currently available supports a role for C. pneumoniae and M. pneumoniae infection as a trigger for 5–30% episodes of wheezing or acute asthma exacerbations 91, 105. In one study of adults with asthma, infection with C. pneumoniae was responsible for 10% of all acute exacerbations 106, similar to rates reported in children aged 5–16 yrs experiencing an acute episode of wheezing 101. The higher prevalence rates of C. pneumoniae among adults with asthma, as compared to age-matched controls, have also been linked to acute exacerbations 107.
Asthmatic children hospitalised for severe asthma attacks tend to have a high incidence of RTIs. In one study, infection with C. pneumoniae and M. pneumoniae occurred with a frequency of 4.5% and 2.2% respectively, in children hospitalised with severe asthma 108. However, a recent study in adults with asthma showed that of C. pneumoniae, Coxiella burnetti, M. pneumoniae and L. pneumophila, only acute infection with M. pneumoniae was associated with the need for hospitalisation for acute exacerbation for bronchial asthma. Furthermore, most patients infected with M. pneumoniae had concomitant respiratory viral infections, making it difficult to determine the precise role of M. pneumoniae in eliciting a severe asthma attack 109.
Chronic asthma
Evidence that C. pneumoniae can induce acute exacerbations and trigger wheezing in patients with asthma has led to suggestions that chronic C. pneumoniae infection may be involved in the natural history of asthma conditioning, by contributing to the chronic inflammation and the airways hyper-responsiveness that is the hallmark of the disease 5. However, whether chronic infection or colonisation with C.pneumoniae or M. pneumoniae plays a role in persistent asthma symptoms or severity remains unclear 91, 95.
The possible role of C. pneumoniae chronic infection in determining asthma severity in adults has been hypothesised by Black et al. 110. The authors described 619 asthmatic subjects screened in a large multinational study of the effect ofantibiotic treatment in asthmatic subjects seropositive for C. pneumoniae. In the screened population, IgG and IgA antibodies to C. pneumoniae were associated with asthma severity markers. A positive association was found between antibodies to C. pneumoniae and the use of high-dose inhaled steroids, higher daytime symptom scores and an inverse association with forced expiratory volume in one second (FEV1) as a percentage of the predicted value. These findings once again raise the possibility that chronic C. pneumoniae infection may lead to an increase in asthma severity.
Both C. pneumoniae and M. pneumoniae are present either alone or together in the airways of significant numbers of patients with chronic, stable asthma 111. Interestingly, patients infected with these pathogens also have significantly more tissue mast cells than uninfected patients. There is alsoevidence to suggest that frequent bacterial infections in infancy may protect against later atopy, which could account for the low rates of atopic asthma in some indigenous populations around the world 105.
Therapy
Although antibiotic therapy is not routinely advocated in the management of acute asthma, there is evidence to suggest that in adult patients with uncontrolled steroid-dependent asthma and recent infection with C. pneumoniae, treatment with macrolides (clarithromycin or azithromycin) can greatly improve symptoms and reduce dependence on steroids 112. In addition to their antimicrobial activity against atypical pathogens, macrolides may also improve symptoms and pulmonary function in patients with asthma by virtue of their anti-inflammatory activities 113.
Two studies have investigated the suppressive effects of macrolides on bronchial hyperresponsiveness in adult patients with asthma. In an 8‐week, randomised, placebo-controlled trial, Amayasu et al. 114 showed that treatment with clarithromycin (200 mg b.i.d.) had bronchial anti-inflammatory effects, which were associated with a significant decrease in eosinophil counts, and hence interleukin‐8 release, compared with placebo in patients with mild or moderate stable asthma. Values for allergen provocative concentration causing a 20% drop in FEV1 (PC20) were also improved. Similarly, Ekici et al. 115 found that administration oflow-dose, intermittent azithromycin (250 mg b.i.w.) to patients with mild asthma resulted in significantly increased values for PC20, although FEV1 values did not differ significantly after 8 weeks of treatment.
Black et al. 116 studied the effect of roxithromycin in subjects with asthma and IgG antibodies to C. pneumoniae ≥1:64 and/or IgA antibodies ≥1:16. In their study, 6 weeks of treatment with roxithromycin 150 mg b.i.d., compared with placebo, led to significant improvement in evening peak expiratory flow at the end of treatment, but the difference between the groups diminished thereafter (fig. 3⇓). Although there was a trend for improvements in the symptom score, this was not significant.

{kind=link}
{kind=link}
{kind=link}
Improvement in evening peak expiratory flow (PEF) for subjects with asthma upon treatment with roxithromycin (□) or placebo (•). EOT: end of therapy. Reproduced with kind permission from Black et al. 116.
In his comment of this paper, Johnston 117 has highlighted that, although C. pneumoniae infection resulted in the clinical benefit observed at the end of treatment, reinfection after cessation of treatment resulted in the loss of benefit during follow-up. In another study, the administration of clarithromycin (500 mg b.i.d.) to patients with chronic stable asthma in a 6‐week randomised, placebo-controlled trial showed that antibiotic therapy was significantly more effective than placebo in improving lung function where patients were PCR‐positive for M. pneumoniae or C. pneumoniae 118. These and other studies should help to determine whether antibiotic therapy can contribute to an improvement in asthma control in individual patients, as well as alter the natural course of the disease 92.
Upper respiratory tract infections
Acute sinusitis
In contrast to infections of the lower respiratory tract, upper RTIs, such as acute bacterial sinusitis, rarely involve infection with atypical respiratory pathogens 2, 119, 120. Even among HIV patients with AIDS, in whom the incidence of acute sinusitis is high, there is little evidence to suggest that atypical bacterial pathogens are involved in infections 120, 121.
Acute sinusitis, characterised by sinus pain and nasal congestion/discharge, usually develops secondary to an upper RTI, such as a cold, and is especially common in children 122. While some studies show antibiotic therapy is effective in relieving symptoms of persistent purulent nasal discharge and cough, others show no significant clinical benefit over placebo 122, 123.
In patients with persistent symptoms, and in whom an aetiological diagnosis cannot be established, treatment options include amoxicillin, high-dose amoxicillin, trimethoprim-sulphamethoxazole or amoxicillin/clavulanate if there is a high risk of resistant pathogens 122, 123. Several clinical studies have shown that newer antibiotics are as effective as older standard agents in treating acute sinusitis in adults and children 124–126; although, for patients with acute uncomplicated sinusitis, the cost of care is significantly higher with newer, second-line agents 127.
Paediatric acute otitis media
Acute otitis media is one of the most common childhood infections, the incidence of which has increased steadily during the past 15 yrs, largely due to increased use of child daycare centres 128. Recent surveys indicate that the typical respiratory pathogens S. pneumoniae, H. influenzae and M. catarrhalis remain the predominant cause of acute otitis media, but their respective prevalence and age distribution show marked age and geographical variation 129, 130. Among younger children, C. pneumoniae has been identified as a cause of acute otitis media. In one study, C. pneumoniae was recovered following tympanocentesis from 8% of children with acute otitis media 129.
The value of antibiotic therapy in the treatment of acute otitis media is controversial, some physicians advocate withholding antibiotics until absolutely necessary. However, complications and adverse clinical sequelae of otitis media, such as perforation of the tympanic membrane, facial paralysis, otorrhoea and mastoiditis, are still prevalent and, although rare, can be life-threatening 131. Physicians are frequently under great pressure from parents to prescribe antibiotics for upper RTIs whether appropriate or not. A recent survey found that 48% of the physicians interviewed had been pressurised by parents to prescribe antibiotics for their children, and that a third had complied in the face of such pressure, even when such therapy was not indicated 132.
The Netherlands, in contrast to most industrialised countries, is among the few not to routinely treat acute otitis media with antibiotics. Instead, physicians prefer to provide only symptomatic treatment initially, and to wait for improvement for 24 h in patients under 2 yrs, or 3 days in those over 2 yrs, before prescribing antibiotics 133. Elsewhere, antibiotic therapy is usually prescribed coincident with a clinical diagnosis of acute otitis media 132. Meta-analyses of randomised controlled trials of antibiotic therapy in acute otitis media show that, compared with placebo, such therapy speeds the resolution of symptoms 134. Short-course therapy over 3–5 days with azithromycin, which covers atypical respiratory pathogens, indicates equal effectiveness as longer courses of standard β‐lactams in acute uncomplicated otitismedia 124.
Tonsillopharyngitis
Pharyngitis is another common upper RTI, especially among children. It ranges from a mild self-limiting illness characterised by sore throat, to one with severe and potentially life-threatening complications such as acute rheumatic fever and glomerulonephritis. Infection with Group A β‐haemolytic streptococcus (GAS) is the most common bacterial cause of pharyngitis. Other bacterial aetiologies include other haemolytic streptococci, staphylococci, pneumococci, H. influenzae, Arcanobacterium haemolyticum, Mycoplasma spp., Chlamydia spp. and anaerobes 125. M. pneumoniae and C. pneumoniae are generally considered infrequent causes of acute pharyngitis 135.
Antibiotic therapy focuses primarily on the eradication of GAS from the upper respiratory tract, for which the IDSA recommends penicillin for first-line use 135, an approach consistent with other guidelines 136, 137. Other effective treatments include macrolides, aminopenicillins, first- and second-generation cephalosporins and clindamycin 135. In patients allergic to penicillin, erythromycin is advocated as a suitable alternative 135 or newer macrolides, such as azithromycin, which have similar activity to erythromycin against GAS, but are better tolerated, should be prescribed 136, 137. There is no evidence to suggest that atypical pathogens should be covered by antibiotic treatment.
Conclusions
As this review illustrates, the atypical respiratory pathogens, C. pneumoniae, M. pneumoniae and Legionella spp., have an important and broad role in acute infections of the lower and, to a lesser extent, upper respiratory tract. The true prevalence of these pathogens in acute RTIs remains unclear, as it relies on the sensitivity and specificity of currently available diagnostic methods. Nonetheless, they are clearly significant contributors in acute RTIs, either as primary pathogens or co-pathogens. C. pneumoniae is also implicated in a number of chronic infectious conditions, both as a trigger and as an exacerbating factor. There is a clear requirement for standardisation in detection methods for atypical pathogens. Wider use of PCR to accurately determine the presence of atypical pathogens in respiratory secretions requires further development work to produce a rapid, reproducible and cost-effective test.
Given the increasingly important role of atypical pathogens in respiratory-tract infections, the balance of opinion at present supports the use of antibiotics that includes activity against these pathogens whenever they are suspected. In vitro studies demonstrate that macrolides, tetracyclines, fluoroquinolones and ketolides possess activity against atypical pathogens, and these findings are supported by clinical studies that have included patients with infections due to Chlamydia pneumoniae, Mycoplasma pneumoniae or Legionella spp. Macrolides have proven efficacy against atypical respiratory pathogens and are advocated for first-line use in most guidelines for treatment of community-acquired pneumonia, where they are indicated either alone or in combination with other antibiotics. The fluoroquinolones are also active against these pathogens. Recognition of the clinical importance of the atypical respiratory pathogens makes it important to monitor the emergence of antibiotic resistance strains, especially to commonly used antibiotics such as macrolides.
- Received December 8, 2003.
- Accepted February 23, 2004.
- © ERS Journals Ltd
References









