





Abstract
The aim of this study was to examine the inflammatory reaction occurring in the pleural space of patients suffering from primary spontaneous pneumothorax (PSP) using pleural lavage, which was performed in patients with PSP and in healthy control subjects (essential hyperhidrosis patients undergoing thoracoscopy for sympathicolysis treatment). Cellular and solute composition of lavage fluid, peripheral blood and parietal pleural biopsies were analysed.
PSP lavage fluid showed an increase in all differentiated leucocytes, but most strikingly eosinophils and neutrophils. In the blood of patients with PSP, the total number of leucocytes and the absolute number of eosinophils, neutrophils and monocytes were also significantly increased. The time in which air was present in the pleural space was positively correlated with the increase of eosinophils in lavage fluid, parietal pleura and blood. Eosinophilic cationic protein was elevated after PSP and strongly correlated with the absolute number of lavage eosinophils. Chemo and cytokine analysis in lavage fluid showed differences in concentrations of interleukin (IL)‐5, IL‐6, IL‐8, IL‐12p40, tumour necrosis factor‐α and RANTES, but not of eotaxin. Surprisingly, high levels of lipopolysaccharide binding protein were also measured.
Primary spontaneous pnumothorax is associated with a substantial pleural inflammatory reaction. The authors hypothesise that mechanical stretch factors, lipopolysaccharide binding protein/lipopolysaccharide complexes or other environmental components trigger pleural inflammation after primary spontaneous pnumothorax.
The Dept of Internal Medicine and the Respiratory Division of the Academic Hospital AZ-VUB supported this work
Primary spontaneous pneumothorax (PSP) is defined as the spontaneous occurrence of air in the pleural cavity in individuals without clinically apparent lung disease 1. PSP occurs most often in male subjects with an asthenic body type. Smoking has also been strongly implicated in the pathogenesis of PSP 2. Previous studies have demonstrated that inflammatory changes in bronchi, lungs and in the pleural cavity may be involved in the pathophysiology of PSP. Anatomical and histological changes in bronchi and lungs, e.g. emphysema-like changes 3 and chronic bronchiolitis 4, 5 have been observed in PSP, and Askin et al. 6 observed a reactive eosinophilic pleuritis in patients with PSP suggesting that air in the pleural space seems to be associated with an eosinophilic inflammatory response in the pleural space. Pleural effusions are rare, but pleural fluid eosinophilia (defined as >10% of the total white cell count in the pleural fluid 7 has been observed in the majority of these cases 8. Smit et al. 9 observed that PSP causes a time-related increase of eosinophil cells in pleural fluid, which seemed to be mediated by interleukin (IL)‐5. Usually, pleural fluid is not observed in patients with PSP. The authors have, therefore, developed a thoracoscopic method (pleural lavage) 10, to access the pleural space in a minimally invasive manner, and to allow analysis of the small volume of pleural fluid which is normally present 10.
The purpose of this study was to characterise the inflammatory changes occurring in the pleural space and the parietal pleura using thoracoscopic pleural lavage and parietal pleural biopsies in patients presenting with PSP, compared with otherwise healthy control subjects undergoing thoracoscopy for treatment of essential hyperhidrosis.
Materials and methods
Patient population
In total, 29 consecutive patients suffering from PSP were studied (21 males and eight females, with a mean±sd age of 36±16 yrs), and 30 healthy controls (nine male, 21 females, mean±sd 30±15 yrs) who were referred for thoracoscopic treatment of severe essential hyperhidrosis. There were 21 smokers in the PSP group (72%) and 10 smokers (33%) in the control group (p=0.006). The time of onset of symptoms of pneumothorax was recorded and considered the start of air entry in the pleural space. A detailed history, physical examination, chest radiography and complete pulmonary function testing confirmed that all control subjects were in perfect health except for the presence of essential hyperhidrosis at the palmar and/or axillary level. All patients with PSP were also tested negative for any other lung disorder besides primary spontaneous pneumothorax before they were included. Verbal informed consent was obtained from every patient and the local ethics committee approved the study.
Pleural lavage technique
The pleural lavage comprised of the injection and retrieval of 150 mL of saline from the pleural space prior to the talcage procedure in the patients with PSP, and prior to the thoracoscopic sympathicolysis procedure in the control population. All procedures were performed under strict aseptic conditions. More details concerning this technique are described elsewhere 10.
Lavage fluid analysis
A drop of well-mixed lavage fluid was introduced into a Bürker chamber for total leukocyte counting. The lavage fluid was centrifuged (10 min, 2,000 rpm) (TJ‐6 Centrifuge, Beckman, Gent, Belgium) and 10 mL of the supernatant was removed and frozen at −70°C for later analysis. The cell pellet was washed with 1 mL phosphate buffered saline (PBS)‐1% bovine serum albumin (BSA; Becton Dickinson, Erembodegem-Aalst, Belgium) and resuspended in PBS‐5% BSA until a suspension of ∼2×106 cells·mL−1 was obtained. Cytospins were made with a cytocentrifuge (Cytospin 3, Shandon Scientific Ltd, Astmoor, UK) and stained with May-Grünwald-Giemsa. Differential cell counts were made on the stained slide, counting 300 cells by light microscopy (×1,150).
The remaining lavage cells were suspended in one volume of PBS and nine volumes RNA-later (Sanbio, Uden, The Netherlands) for RNA preservation and frozen at −70°C for RT-PCR analysis.
Blood analysis
Blood samples were taken on the same day as the pleural lavage. Total and differential counts of the peripheral blood cells were performed with an automatic cell counter (Cell-Dyn 4000, Abott, Louvain-la-Neuve, Belgium).
Parietal pleura
A total of five biopsies of the parietal pleura were obtained during thoracoscopy using 5 mm biopsy forceps. Specimens were fixed with Bouin and imbedded in paraffin. The biopsies were stained with haematoxylin-eosin-saffran and stained for myeloperoxidase and leukocyte cmmon antigen. The cells were counted with light microscopy per high powerfield, i.e. the number of cells on a field at a magnification of ×400.
Solute Analysis
Eosinophilic cationic protein (ECP) concentrations were measured with a radio-immunoassay method (Pharmacia&Upjohn, Brussels, Belgium) in the supernatant of unconcentrated lavage fluid. Commercially available ELISA kits were used for the quantification of: eotaxin (sensitivity test: <2.2 pg·mL−1), interferon‐γ (IFN‐γ; <4 pg·mL−1), tumor necrosis factor−α (TNF−α; 1.7 pg·mL−1), interleukin (IL)‐1β (<1 pg·mL−1), RANTES (<3 pg·mL−1), IL‐2 (0.1 U·mL−1), IL‐5 (<4 pg·mL−1), IL‐6 (5.5 pg·mL−1), IL‐8 (<5 pg·mL−1), bioactive IL‐12 (<0.8 pg·mL−1), IL‐12p70 (<4 pg·mL−1) (Biosource, Nijvel, Belgium) and lypopolysaccharides (LPS)-binding protein (LBP) (1 ng·mL−1; Sanbio, Uden, Holland; LPS from Serratia Marcescens (100 pg·mL−1; Sigma-Aldrich chemie, Schnelldorf, Germany) were measured as described by Peterfi and Kocsis 11.
Microbiological analysis
Samples of the lavage fluid were tested for the presence of bacteria and fungi.
Statistical Analysis
Cellular data are expressed as median and interquartile ranges (IR: P25–P75). Comparison between data for the PSP and the control population were made with the nonparametric two-sided Mann-Whitney test. Correlations between data were analysed with the Spearman-correlation coefficient (r). Significance was accepted at p<0.05.
Results
All lavage procedures were uneventful. Lavage prolonged the thoracoscopy time by only 1–3 mins and no complications were observed.
Cell counts in lavage fluid and peripheral blood
Lavage fluid
The authors observed a significant increase in the absolute number of all nucleated cells after PSP. Relative differential cell counts in patients with PSP versus the controls are shown in figure 1⇓, and absolute cell counts in table 1⇓. Whereas the percentages of lymphocytes and macrophages predominate in normal control subjects 10, neutrophils and eosinophils were increased in PSP at the expense of lymphocytes and macrophages. The percentage of mesothelial cells was not significantly different in PSP as compared with normal controls.
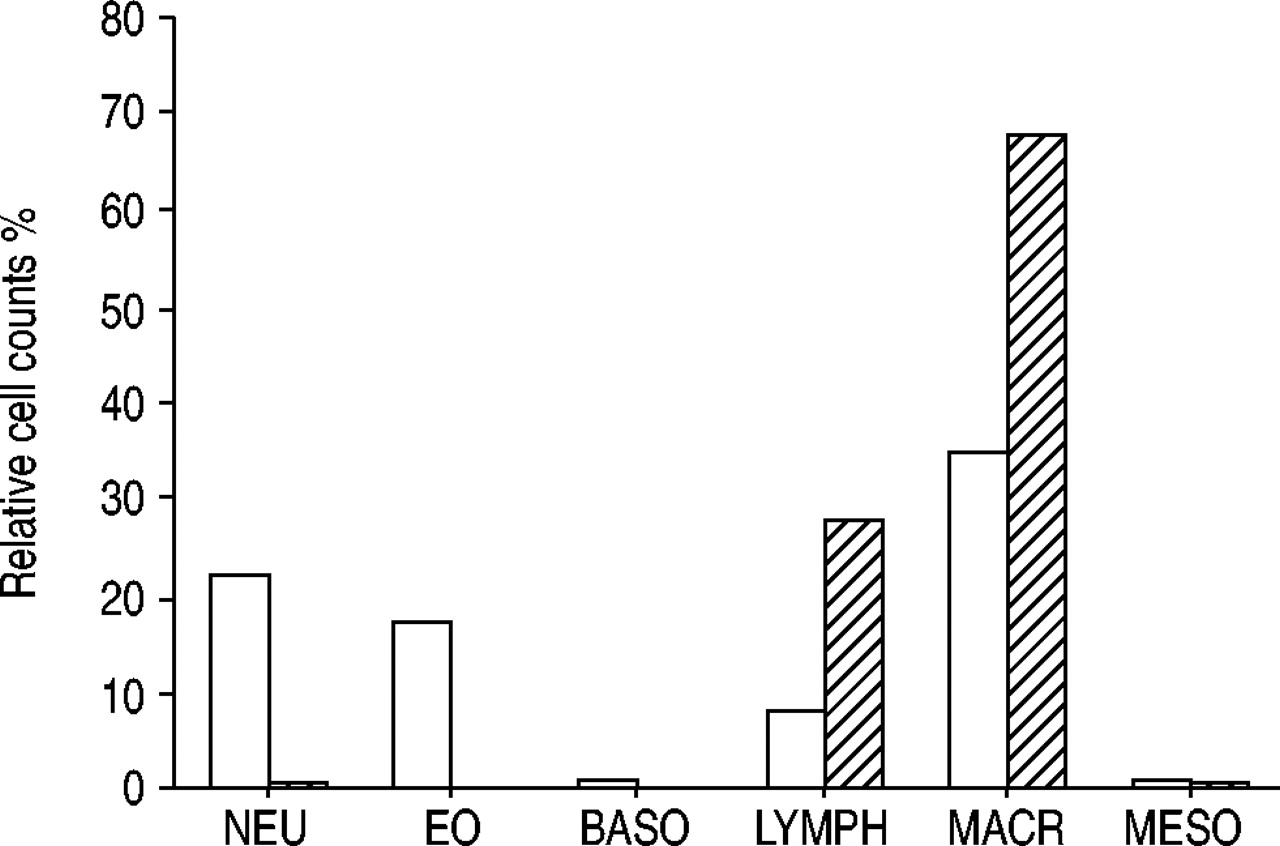
Lavage cell counts. Absolute cell counts per mm3 in lavage fluid of primary spontaneous pneumothorax patients (□) and controls (└) are expressed as median (interquartile range: 25–75). Differential cell counts: distinct neutrophils (NEU), eosinophils (EO), basophils (BASO), lymphocytes (LYMPH), macrophages (MACR) and mesothelial cells (MESO).
Lavage cell counts
Peripheral blood
The white blood cell (WBC) differential counts in the peripheral blood of patients with PSP and healthy controls are presented in table 2⇓. There was a significant increase in total WBC count and in neutrophils, eosinophils and monocytes in patients with PSP. A correlation was found between the absolute number of eosinophils in the lavage fluid and in the blood (r=0.61; p=0.002).
Blood cell counts
Duration of the pneumothorax
The duration of the pneumothorax (expressed as the number of hours between the occurrence of symptoms and the thoracoscopic intervention) correlated with the observed changes in differential cell counts. The relative number of eosinophils correlated with the time of air presence in the pleural space (r=0.85, p<0.001).
Inflammation in the parietal pleura
During the thoracoscopic intervention, blebs were occasionally present in the PSP population. Signs of rupture or bleeding were not found. Inflammatory changes in the parietal pleura of patients with PSP were invariably observed. The haematoxyline-eosine-saffran staining clearly showed the presence of eosinophils, and both mesothelial thickening and proliferation of the pleura. The staining for myeloperoxidase and leukocyte common antigen respectively showed an increase in neutrophils, and all WBC in the parietal pleura. No eosinophils or neutrophils were present in the parietal pleura of healthy controls. In patients with PSP however, there were 1–34 (median 6) eosinophils (p=0.002) and 6–12 (median 7) neutrophils (p<0.001) per high power field. The number of eosinophils in the parietal pleura correlated with the number of eosinophils in the lavage fluid (r=0.76, p=0.002).
Eosinophil activation
The concentration of eosinophilic cationic protein (ECP) in the lavage fluid of patients with PSP was increased (median: 19; IR: 9–43) µg·L−1, whereas in the control group ECP concentrations were not detectable (<2 µg·L−1). The ECP concentration and the absolute number of eosinophils in the lavage fluid were strongly correlated (r=0.96, p<0.001).
Concentration of cytokines, chemokines and other biomolecules in pleural fluid supernatant
The concentration of several chemokines and cytokines was measured in the lavage fluid of patients with PSP and in the control group. The concentrations of IL‐5, IL‐6, IL‐8, TNF‐α and LBP were significantly increased after PSP (fig. 2⇓), whereas RANTES was decreased . A weak, but significant positive correlation was found between TNF‐α/IL‐6 and TNF‐α/IL‐8 (p=0.04; r=0.41 and p=0.03; r=0.43). IL‐12 is a 70 kDa (p70) lymphokine composed of a subunit of 40 kDa (p40) and a subunit of 35 kDa (p35) linked through a disulphide bridge. The concentration of IL‐12 (p40+p70) was increased in the lavage fluid of PSP patients (median: 23.9; IR: 8.3–43.6) in comparison with the control group (median: 8.9; IR: 6.2–9.9), but no increase was found for IL‐12 (p70), suggesting that only the p40 subunit was present. The concentrations of IFN‐γ, IL‐1β , IL‐2, eotaxin and LPS, showed no significant differences (data not shown). However, a significant difference (p=0.03) in LPS concentration was found between the smokers in both populations. The concentration of LBP (ng·mL−1) was higher in the PSP population (median: 97.3; IR: 91.8–101.2) in comparison to the control group (median: 0.7; IR: 0.4–1).

{kind=link}
{kind=link}
Data a) tumour necrosis factor‐α, b) interleukin IL)‐6 and c) IL‐8 concentration in pleural lavage fluids of patients with primary spontaneous pneumothorax and controls, presented as pg·mL−1 as median, (interquartile range 25–75), minimum and maximum. #: extremes; ¶: outliners; *: p<0.05.
Microbiological analysis
All sample cultures of healthy controls and patients with PSP were negative for bacteria and fungi.
Discussion
This is the first prospective study on thoracoscopic pleural lavage, pleural biopsy, and peripheral blood findings in consecutive patients with PSP , compared with healthy control subjects. This study shows a substantial pleural inflammatory reaction in patients with PSP, which is characterised by increases in pleural fluid and parietal pleural tissue eosinophils and neutrophils, and associated with a characteristic cytokine pattern.
Only two reports on pleural cell counts in patients with PSP have previously been published 8, 9 ,showing increases in total and differential cell counts which are comparable with the results in our patients with PSP. The present findings confirm that PSP is associated with a dramatic influx of eosinophils, but also of neutrophils in the pleural space. Our results also confirm the previously demonstrated relationship between the number of eosinophils in the pleural fluid and the duration of the pneumothorax.
Inflammatory cellular changes in the peripheral blood occurring after PSP were also examined for. Two case reports 8 have described the blood cell counts after PSP associated with pleural effusions, yielding 8,200 and 11,300 WBC·mm−3, respectively with 5% and 3% eosinophils, 70% and 80% neutrophils, 23% and 16% lymphocytes and 2% and 1% monocytes, but no comparison with control subjects was made. The authors observed, in comparison with normal subjects, a significant increase of the total number of WBC (9, 750 versus 7,800·mm−3), eosinophils (255 versus 90·mm−3), neutrophils (5,259 versus. 4,032·mm−3) and monocytes (765 versus 430·mm−3) in the peripheral blood of patients wih PSP. A correlation between the absolute number of eosinophils in the blood and lavage fluid was also present.
Increased numbers of eosinophils and neutrophils in the parietal pleura have also been described 6, 7, but no quantitative data are available. The authors observed no eosinophils or neutrophils in the parietal pleura of the control group, whereas these inflammatory cells were abundantly present in the parietal pleura after PSP. Furthermore, the number of eosinophils in the parietal pleura correlated with the increased number of eosinophils in the lavage fluid in patients with PSP.
ECP, a marker for eosinophil activation 12, 13 was not detectable in the control subjects (<2 µg·L−1), whereas in the patients with PSP increased ECP concentrations were observed (median: 19; IR: 9–43 µg·L−1). ECP concentration correlated well with the absolute number of eosinophils in the pleural lavage fluid, suggesting activated eosinophils to be the source of ECP.
The exact mechanism of pleural inflammation occurring after PSP is unclear. IL‐5, an eosinophil-specific cytokine stimulating chemoattraction and activation of eosinophils 12, 13, 14 may play a key role in this inflammatory process [9, 15, present study] whereas other eosinophil-specific cytokines and chemokines (e.g. eotaxin, RANTES) seem not to be involved. The observations from this current study, of increased numbers of neutrophils in the pleural lavage fluid and of an increased IL‐8 concentration, also point to a more nonspecific component of inflammatory reaction. Penido et al. 16 have reported that migration of eosinophils into the pleural space can occur independently of eotaxin, RANTES and IL‐5 after intrapleural stimulation with LPS. LPS, a component of bacterial endotoxin, is a potent inducer of cell activation and induces secretion of a large number of pro-inflammatory cytokines 16, 17. In the presence of LPS-induced inflammation, respiratory epithelial cells produce LBP, an acute phase protein and most important defender against bacterial endotoxins 18. LBP forms complexes with LPS, to which macrophages respond by producing TNF‐α and IL‐1. Following release of these cytokines, an inflammatory cascade is initiated including the production of IL‐6 and IL‐8, in turn resulting in increased LBP production 19. Although LPS concentrations were not different in the lavage fluids of controls and patients with PSP, there was a significant increase after PSP as compared with controls in the actively smoking subjects, and LBP concentrations were also significantly higher in all PSP subjects. The authors therefore hypothesise, in accordance with previous observations, that PSP-induced exposure of the pleural space to environmental air could lead to an inflammatory reaction (either induced by mechanical stretching of the pleura, or by pro-inflammatory effects of one or more contaminants such as LPS or tobacco smoke), which is characterised by the influx of eosinophils 16 and by the production of LBP 18. The former may stimulate IL‐5 production 20, whereas the latter may stimulate the production of TNF‐α , IL‐1, IL‐6, and IL‐8. Alternatively, as all but two patients were treated with chest tube drainage prior to thoracoscopy, the presence of this foreign body in the pleural space may also have contributed to the observed inflammatory changes. In order to exclude this hypothesis, PSP patients should have undergone thoracoscopy without previous aspiration chest tube drainage. However, this occurs only rarely in clinical practice and was performed in only two patients with PSP. Interestingly, pleural and blood analyses in these patients were similar to those in chest-tube treated patients.
Not unexpectedly, there were more smokers in the PSP population. Cigarette smoking undoubtedly is involved in the pathogenesis of PSP 2, however, its role in the pleural inflammation occurring after PSP, the subject of this study, is unclear. The observation that LPS concentrations are higher in the pleural lavage fluid of smoking patients with PSP as compared with smoking, healthy controls, and the fact that cigarette smoke is a known source of LPS 21, may support the hypothesis explained above.
The authors conclude that primary spontaneous pneumothorax is associated with a substantial pleural inflammatory reaction, which is characterised by the influx (and activation) of eosinophils and neutrophils into the pleural space and parietal pleura, and by an increase in the total white blood cell count in the peripheral blood. Interleukin‐5, interleukin‐6, interleukin 8, tumour necrosis factor‐α, interleukin‐12p40 and lipopolysaccharide binding protein are significantly increased in the pleural lavage fluid. This inflammatory pattern may have been induced by a lipopolysaccharide-mediated defense response.
Acknowledgments
The authors would like to thank the personnel of the haematology/immunology and microbiology laboratories.
- Received July 9, 2003.
- Accepted February 11, 2004.
- © ERS Journals Ltd
References









