





Abstract
The aim of this study was to correlate daily use of nasal continuous positive airway pressure (nCPAP) with total sleep time (TST) evaluated by home actigraphy.
Actigraphy was validated by comparing TST determined by actigraphy (aTST) and polysomnography (pTST) in 24 untreated patients with suspected sleep apnoea. The % sleep time spent under nCPAP was estimated on 3 consecutive days in 28 patients receiving long-term nCPAP, by comparing machine-use periods with sleep periods identified by home actigraphy.
The mean difference between pTST and aTST was 2.5 min. The correlation coefficient between aTST and pTST was 0.90. Daily use of nCPAP over the 3 study days was 388±114 min. nCPAP was used 41–100% (82±17% (mean±sd)) of sleep time detected by actigraphy. Some patients used nCPAP during nonsleep periods.
In conclusion, comparison of nasal continuous positive airway pressure use with sleep time estimated by home actigraphy shows marked individual differences in the % sleep time under nasal continuous positive airway pressure. These results suggest that actigraphic estimation of sleep time under nasal continuous positive airway pressure could provide a better index than simple daily use of the device to evaluate the impact of treatment in sleep apnoea.
- Compliance
- nasal continuous positive airway pressure
- obstructive sleep apnoea
- treatment
- wrist-actigraphy
Obstructive sleep apnoea syndrome (OSAS) is a common disease 1, usually inducing excessive daytime sleepiness, which is responsible for an increased risk of car or work-related accidents 2, 3. OSAS is now recognised to be an independent risk factor for hypertension, cerebrovascular accidents and coronary insufficiency 4–6. Nasal continuous positive airway pressure (nCPAP) 7 constitutes the reference treatment for OSAS. Its beneficial effects on quality of life, daytime alertness and systemic blood pressure have been demonstrated by controlled studies 8–11. The amplitude of this benefit appears to be related to the duration of nCPAP use 10, but nCPAP is a constraining treatment associated with frequent local adverse effects that can constitute an obstacle to regular and prolonged use of the apparatus 12, 13. Compliance with treatment, therefore, constitutes an essential component of evaluation of the results of nCPAP therapy. Compliance was initially evaluated subjectively by clinical interview of the patients 14 and then, more objectively, by introducing an in-built counter into the nCPAP machine, which indicates the number of hours of machine-run time, but which does not necessarily correspond to real use. The patient's compliance with treatment can now be evaluated more precisely by counting the number of hours during which the prescribed pressure is delivered by the machine, which requires the machine to be effectively connected to the patient. According to various studies, this effective compliance ranges between 4–7 h·day−1 15–19. The percentage of regular nCPAP users (>4 h for at least two out of three nights) ranges from 46–80%, according to various authors 15, 18. This assessment of compliance is based on the hypothesis of equivalence between nCPAP-run time and sleep time, and does not take into account the patient's total sleep time (TST). By definition, the physiological sleep requirement varies from one individual to another. An equivalent daily compliance can, therefore, correspond to variable effectiveness of nCPAP treatment according to the patients' sleep time. It would, therefore, be very useful to determine the actual sleep time spent under nCPAP. Clinical interview may be helpful, but remains very imprecise. Actigraphy could be adapted to this objective. It is a simple and compact tool, allowing outpatient identification and quantification of sleep. Validation studies comparing polysomnography (PSG) and actigraphy, performed simultaneously, have reported a good level of concordance for determination of TST; although these results were for nonclinical samples and used different devices and algorithm 20–22. The American Academy of Sleep Medicine has recognised actigraphy as a useful adjunct in the clinical assessment of sleep disorders 23.
This study aimed to correlate daily nCPAP compliance with sleep time evaluated by home actigraphy. It consisted of two steps. The first step (In-Lab study) aimed to validate the actigraph used in the study (Actiwatch®; Cambridge Neurotechnology Ltd, Cambridge, UK), by comparing the TST determined simultaneously by actigraphy (aTST) and PSG in the laboratory (pTST) in patients investigated for suspected OSAS. The second step (Home study) determined the percentage sleep time spent under nCPAP, by comparing machine-use periods with sleep periods identified by home actigraphy, in sleep apnoea patients receiving long-term nCPAP.
Patients and methods
Actigraphy
The Actiwatch is a compact (27×26×9 mm), light-weight (16 g) wrist accelerometer, in which an internal piezoelectric sensor monitors the occurrence and extent of motion. The accelerometer flexes when the Actiwatch is moved, producing a voltage in the sensor. The degree and force of flexing influence the voltage, which is translated into activity counts. The maximum frequency is 32 Hz. Actigraphic data were analysed by using the algorithm supplied by Sleepwatch sleep analysis software (Cambridge Neurotechnology Ltd). Using the default medium sensitivity that was chosen for this study, an integrated activity count ≥40 within a 1‐min epoch designates the epoch as being “awake”. For automatic determination of sleep start, the algorithm searches for a period of at least 10 min of consecutively recorded immobile data, with no more than 1 epoch of movement within this period, following the lights-off time. The start of this defined period is classified as sleep start. For sleep end, the algorithm searches for a 10‐min consecutive period of activity around the lights-on time, and then works back to find the last epoch of immobility before the start of such a sequence and classifies that as sleep end. The aTST is calculated by the Sleepwatch software from sleep start to sleep end, after excluding the epochs designated as being awake.
In-Lab study
This study was conducted in consecutive patients in whom PSG was prescribed for clinical suspicion of OSAS, due to a combination of snoring, apnoeas described by the family and excessive daytime sleepiness. Each patient agreed to wear the actigraph during the PSG night and the study was approved by the institutional review board. PSG measurements included sleep stage (electroencephalogram, electro-oculogram, and submental electromyogram); nasal (nasal cannulae) and oral airflow (oral thermistance); rib cage and abdominal wall motion (respiratory inductance plethysmography); and arterial oxygen saturation (Sa,O2). Actigraphy was performed simultaneously to PSG. Both recordings were started at the same time and were carefully synchronised. Lights off and lights on were indicated on the activity monitor by pressing a button. PSG and actigraphic data were analysed independently by two different scorers. All PSG data were scored manually. Sleep staging was performed according to standard criteria 24. TST was measured from the moment the patient fell asleep until final awakening, excluding wake time during sleep. Apnoea was defined as cessation of airflow for >10 s. Hypopnoea was defined as a reduction of airflow, regardless of its amplitude, with >3% fall in Sa,O2 or arousal 25. pTST and aTST were compared.
Home study
Patients with OSAS, diagnosed by PSG and receiving long-term nCPAP treatment, were recruited consecutively at treatment follow-up visits. All the patients were treated with an nCPAP device (Sullivan S6 EliteTM; Resmed, Sydney, Australia), which was equipped with a microprocessor and pressure monitor that provided a precise index of nCPAP use by measuring time spent with the mask on for every 24‐h day 15–19. Patients who consented to participate in the study completed an individual questionnaire, comprising anthropometric data and Epworth sleepiness scale 26. Then, patients were invited to wear an actigraph in order to evaluate the quality of their sleep at home. The actigraph had to be worn on the nondominant wrist for 72 h; during this time, the patients indicated lights off and lights on by pressing a button on the activity monitor. The actigraph installation visit was also used to calculate daily compliance with nCPAP over the previous 30 days. Daily compliance during this period was calculated by dividing the number of hours of nCPAP (delivered at the prescribed pressure derived from pressure recording) by 30. At a second home visit, 3 days later, the actigraph was collected and nCPAP use data were extracted from the memory of the device. Sleep periods were identified from the Sleepwatch software and aTST was calculated for the three consecutive 24‐h periods (D1, D2, D3). nCPAP-use periods, at the prescribed pressure (which requires the machine to be effectively connected to the patient) for each 24‐h period (D1, D2, D3), were extracted from the memory of the device (in-built manometer) to be compared to the actigraph records. For each consecutive 24‐h day, the periods of nCPAP use at the prescribed pressure were aligned to the sleep periods identified by the actigraph, in order to calculate the sleep time spent under nCPAP for D1, D2 and D3. Then, the number of hours of sleep under nCPAP was divided by aTST, to determine the percentage sleep time spent under effective nCPAP treatment for each study day. The study was approved by the institutional review board.
Statistics
All values were summarised by descriptive statistics and expressed as mean±sd. Paired-samples t‐test was used to compare the means of continuous variables. The current authors used Pearson's linear regression test to correlate between aTST and pTST, and between nCPAP compliance and the estimated percentage sleep time under nCPAP. Significance was imparted at p<0.05. Agreement between actigraphy and PSG for TST measurement was evaluated according to the Bland and Altman method 27.
Results
In-Lab study
The study was conducted in 24 patients (nine females) with a mean±sd age 50±16 yrs and body mass index (BMI) 28.2±5.2 kg·m−2 in whom apnoea/hypopnoea index (AHI) was on average 38.4±32.2 h−1 of sleep on PSG. The mean (range) pTST was 328±82 min (114–407) and the aTST was 325±88 min (69–407). The Pearson correlation coefficient between aTST and pTST was 0.90, p<0.0001. Agreement between actigraphy and PSG for TST measurement according to the method of Bland and Altman is shown in figure 1⇓. The mean (95% confidence interval) TST difference between PSG and actigraphy was 2.5 min (−73.1–78.1). The difference between pTST and aTST exceeded 1 h in three patients, for whom TST was underestimated by actigraphy in two cases and overestimated in one case.

Bland and Altman plot showing difference versus mean total sleep time determined by polysomnography (pTST) and actigraphy (aTST). Data are presented as mean (––) ±2sd (---).
Home study
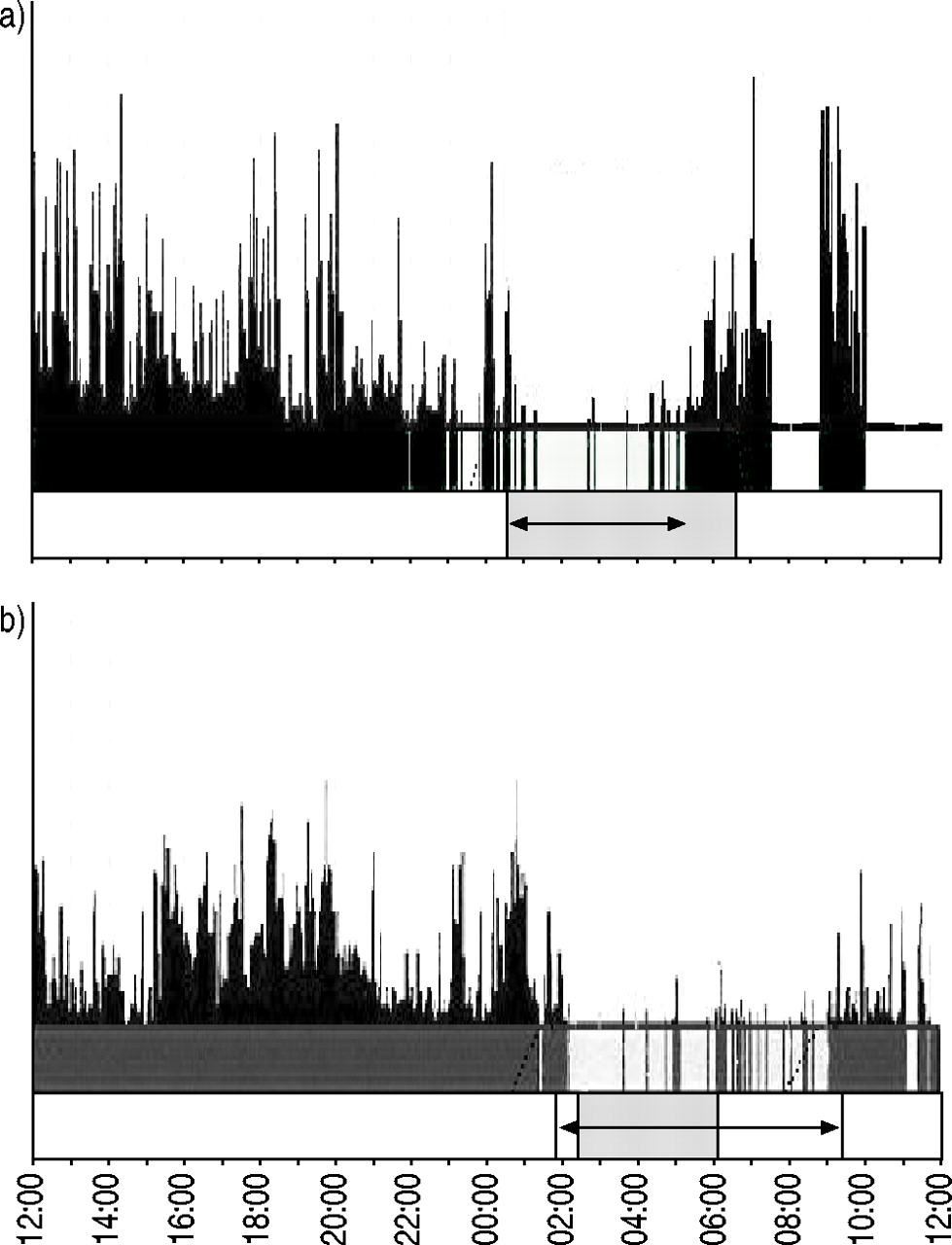
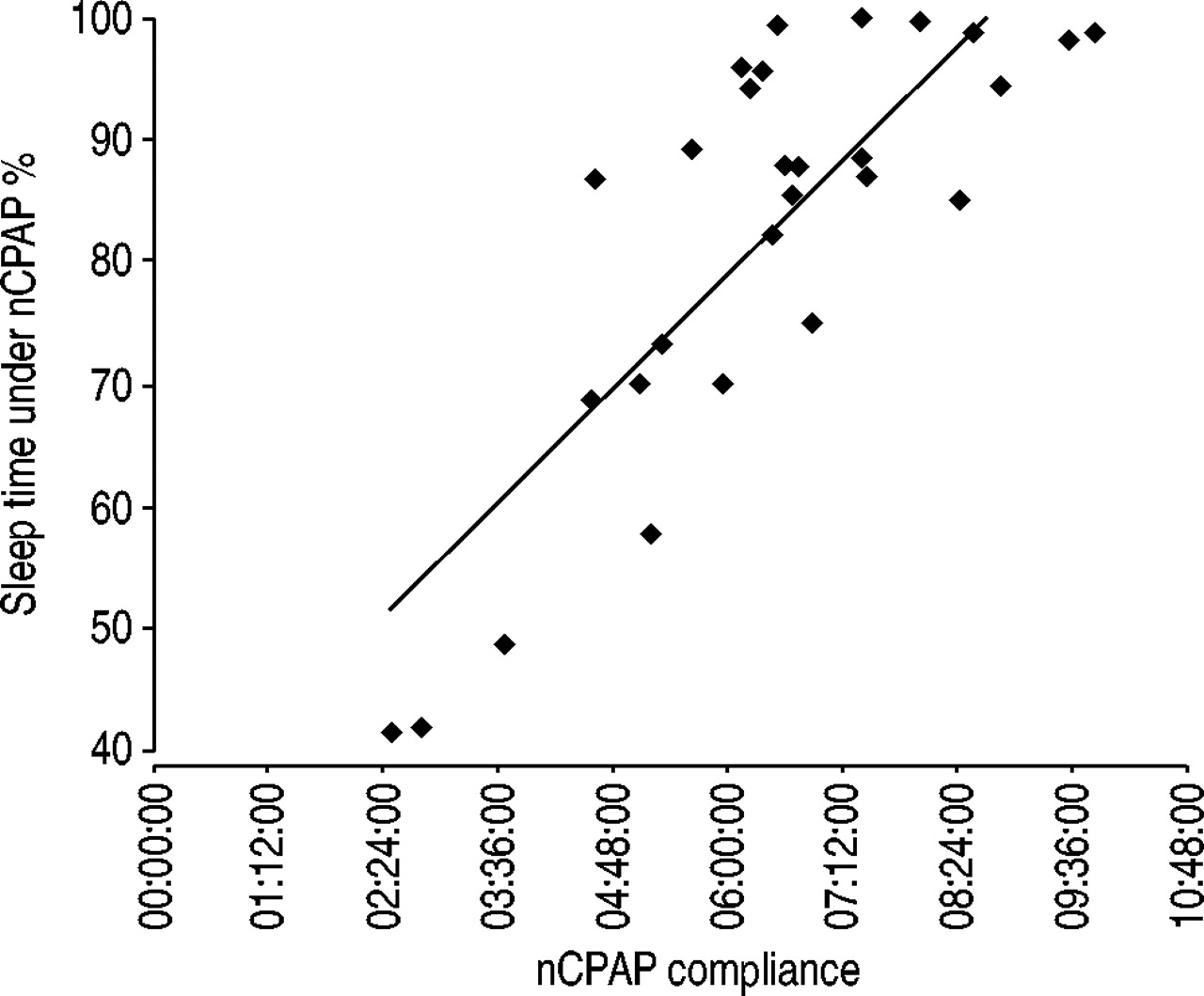
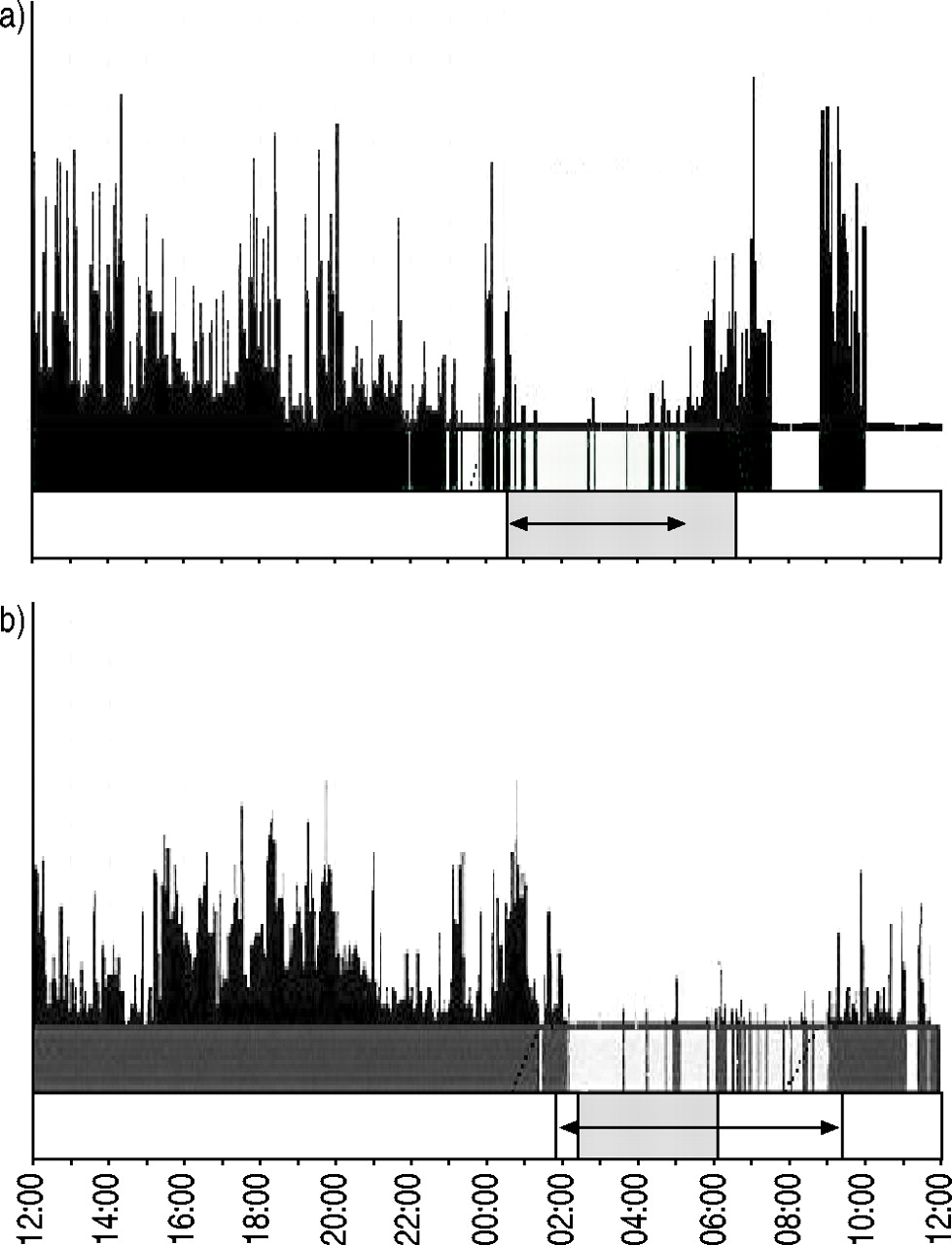
The study was conducted in 28 patients (two females) of 56±11 yrs and BMI 28.3±4.4 kg·m−2. All were treated with nCPAP at a mean (range) pressure of 10±1.5 cmH2O (6–12) for a duration of 158±100 days (36–352) for an OSAS diagnosed by PSG (AHI: 51.6±20.3). The score on the Epworth sleepiness scale was 6.37±3.9 with nCPAP at the inclusion visit versus 10.07±4.67 at the time of diagnosis (p<0.001). The compliance with nCPAP was not higher during the study (388±114 min (150–590)) than during the previous 30 days (384±97 min (147–582)). Actigraphic data were analysed for the three study-nights in the 28 patients. In two cases, patients had forgotten to press the event button for lights off and/or lights on. For these two study-nights, bedtime and get-up time were obtained by questioning the patients. Table 1⇓ shows the comparison of nCPAP compliance, aTST and the estimated sleep time under nCPAP over the 3 days of the study. nCPAP compliance and aTST were very similar when analysed separately. Conversely, sleep time under nCPAP, estimated by superimposing the sleep periods detected by the actigraph onto periods of nCPAP use, was about 60 min lower than aTST and nCPAP compliance (p<0.05). On average, the estimated sleep time (range) under nCPAP was 82±17% (41–100). Three patients used nCPAP for <50% of their sleep time and five used nCPAP for <70% of their sleep time. nCPAP compliance and sleep time under nCPAP were significantly correlated but showed remarkable individual differences (fig. 2⇓). Some patients turned off the nCPAP machine in the middle of the night and continued to sleep without treatment. Conversely, some patients continued to use their nCPAP machine during nonsleep periods at the end of the night (fig. 3⇓).

Comparison of nasal continuous positive airway pressure (nCPAP) compliance and the estimated sleep time under nCPAP. y=1.8676x+0.3213; R=0.80 (p<0.001).
{kind=link}
{kind=link}
{kind=link}
Comparison of sleep periods detected by the actiwatch with nasal continuous positive airway pressure (nCPAP)-use periods extracted from the memory of the device over 24 h in two different patients. Bedtime and get-up time are indicated by black vertical bars, arrows indicate sleep period and ▓ indicates CPAP-use period. a) nCPAP use exceeds sleep time detected by the actiwatch. b) nCPAP use is lower than sleep time detected by the actiwatch.
Comparison of nasal continuous positive airway pressure (nCPAP) compliance, actigraphy derived total sleep time (aTST) and estimated sleep time under nCPAP treatment in 28 patients
Discussion
Compliance with treatment is one of the main endpoints of follow-up in patients receiving long-term nCPAP therapy for OSAS. Considerable efforts have been made to measure compliance as accurately as possible. Most of the currently available nCPAP machines indicate the daily duration of nCPAP use at an effective pressure which, according to various studies, ranges from 4–7 h·day−1 15–19. This evaluation of compliance does not take into account the patient's usual sleep time which, by definition, varies from one individual to another. Regular use of nCPAP for at least 5 h per night is generally considered to be satisfactory 28. However, the benefit provided by this duration of use can vary considerably between two patients whose usual sleep time is 5 h and 8 h per night, respectively. An objective measurement of the sleep time of the patients seems necessary for an individual evaluation of nCPAP compliance. The American Academy of Sleep Medicine has recognised actigraphy as a useful adjunct in the clinical assessment of sleep disorders 23. It provides a low-cost, noninvasive method to estimate sleep-wake schedules in the ambulatory setting. The validity of actigraphic assessment of sleep has been supported by the highly significant correlations between actigraph- and PSG-based whole-night sleep measures such as sleep efficiency, sleep duration or sleep latency (above 0.80 for most samples in various studies) 29.
To the present authors' knowledge, the current study is the first to correlate daily nCPAP compliance with sleep time evaluated by actigraphy. A commercially available algorithm (Sleepwatch) was used, with the arousal threshold set at 40 activity counts within a 1‐min epoch. The first step of this study consisted of comparing actigraphy and PSG in 24 patients investigated for suspected OSAS. A strong correlation between actigraphy and PSG for TST measurement was found. On average, the TST estimated by the actigraph was very close to that simultaneously determined by PSG (325±88 versus 328±82 min). The current results are in agreement with those reported by Elbaz et al. 30, who used the same actigraph adjusted according to the same parameters in a similar population, in terms of age, BMI and sleep apnoea severity. The difference between pTST and aTST exceeded 1 h in three of the current authors' patients. In two of these three patients, TST was underestimated by actigraphy. One of them had a highly disturbed sleep and a short duration of sleep; the second one, a high sleep fragmentation due to severe sleep apnoea syndrome (AHI: 87 event·h−1). Periods of immobility, due to the discomfort from recording instrumentation (“first-night effect”), may explain TST overestimation in some patients. The accuracy of actigraphy has been recognised to decline as the quality and quantity of sleep diminishes 23. Several factors, such as sleep fragmentation due to sleep apnoea and first-night effect, may explain the discrepant results that were observed between actigraphy and PSG in some of the in-lab study patients. A potential limitation of this validation study is that it was performed in patients who were not under nCPAP treatment; whereas, the home-study sample used patients receiving nCPAP. Actigraphy is more accurate when used to differentiate major periods of sleep and waking in good sleepers as compared to patients with disturbed sleep 23. nCPAP has been shown to reduce the sleep fragmentation associated with sleeping upper airway collapse, and improve sleep quality in sleep apnoea patients 31. Thus, it can be speculated that actigraphy provided an accurate assessment of the sleep-wake patterns in the home-study patients, who received long-term nCPAP treatment for sleep apnoea and were recorded in their home environment.
The second step of this study aimed to correlate daily compliance with sleep time evaluated by actigraphy on 3 consecutive days, in 28 patients receiving long-term nCPAP. The patients had been treated for an average of 5 months. Most of them had, therefore, completed the initial treatment acceptance and habituation phase. nCPAP compliance, during the study and the previous 30 days (∼6.5 h), was comparable to that reported in a French multicentre study based on 3,225 patients treated by nCPAP for >6 months 32. On average, the estimated sleep time under nCPAP was 82% and varied from 41–100%. nCPAP compliance and % sleep time under nCPAP were significantly correlated but showed remarkable individual differences. Comparison of sleep periods detected by actigraphy, with nCPAP-use periods extracted from the memory of the device, revealed that some patients turned off their machine in the middle of the night; whereas, some other patients used their machine during nonsleep periods. Taking into account the short duration of follow-up, the current authors' did not use diary or sleep log for the home study. For two study nights, when patients had forgotten to press the event marker, bedtime and get-up time were obtained by questioning the patients. However, the use of sleep log should be recommended to obtain documentation on bedtime, rise-time or artefacts (actigraph-off times) when using actigraphy for a longer duration of follow-up. Several previous studies had correlated nCPAP compliance with usual sleep time evaluated by questionnaire. Over a 28‐day follow-up period, Reeves-HochÉ et al. 16 evaluated daily compliance to represent 66% of the sleep time reported by the patients. Another study, concerning patients with mild-to-moderate OSAS, reported a daily use of 3.1 h corresponding to 44±34% of declared sleep time 33. In a more recent study concerning 74 patients with AHI of 35±31 treated with nCPAP for 9 months, a daily compliance of 3.6±2.5 h corresponded to 56±33% of declared sleep time 34. These studies were based on the hypothesis of equivalence between nCPAP run time and sleep time. The current authors' data clearly show that discrepancies can exist between these two variables.
Sleep apnoea has been shown to be an independent risk factor for cardiovascular disease 4–6. A large population-based study showed that each additional apnoeic event per hour of sleep increased the odds of hypertension by ∼1% 35. The effect of nCPAP on blood pressure depends on the duration of daily use 10 and the percentage of respiratory events effectively eliminated by treatment 11. The fact that a 50% reduction in the AHI did not result in a decrease of blood pressure in the study of Becker et al. 11 emphasises the importance of highly effective treatment. The % sleep time under nCPAP (estimated by actigraphy) could constitute a better index than simple daily compliance, in order to evaluate nCPAP treatment effectiveness. Actigraphic estimation of % sleep under nCPAP could be useful in patients presenting a low clinical benefit, despite an apparently correct nCPAP daily use.
In conclusion, home actigraphic estimation of sleep time demonstrates that % sleep time under nasal continuous positive airway pressure is potentially high, but shows remarkable individual differences. This study, which may be limited by its small sample size and its short duration of follow-up, suggests that actigraphic estimation of % sleep under nasal continuous positive airway pressure could provide a better index than simple daily compliance, in order to evaluate the impact of treatment in obstructive sleep apnoea syndrome.
- Received August 4, 2003.
- Accepted February 11, 2004.
- © ERS Journals Ltd
References









