





Abstract
“Cyst-like” structures within the ciliary shafts were considered in four adults as a primary defect involved in the development of bronchiectasis. In this study, the presence and the primary or secondary nature of this abnormality were assessed in children with bronchiectasis.
High resolution computed tomography (HRCT) and nasal biopsies for motion analysis and transmission electron microscopy (TEM) evaluation of cilia were obtained in 45 children with recurrent lower airway infections and abnormal chest radiography.
HRCT disclosed bronchiectasis in 35 out of 45 (77.8%) children and cyst-like structures were demonstrated with TEM in 29 out of 45 (64.4%) patients. Cyst-like structures were constantly associated with other ultrastructural abnormalities commonly observed in chronic inflammation, and were found both in subjects with primary and with secondary ciliary dyskinesia. When considering only patients with bronchiectasis, a significant correlation between prevalence of cyst-like structures and the severity of bronchiectasis was demonstrated. Follow-up (2–22 months) of seven patients demonstrated that in the five children with secondary dyskinesia, the ultrastructural defect completely disappeared and there was a small reduction in the abnormality in the two patients with primary dyskinesia.
In contrast to one previous report, the reversibility of the defect suggests its secondary origin, which is most likely related to chronic airway inflammation.
- Bronchiectasis
- children
- cyst-like structures
- high resolution computed tomography
- transmission electron microscopy
Impairment of mucociliary transport in patients with ciliary ultrastructural abnormalities, such as in primary ciliary dyskinesia (PCD), usually results in the development of early-onset bronchiectasis due to recurrent respiratory tract infections 1–5. Occasionally, patients with PCD show a normal ciliary ultrastrucural pattern with abnormal ciliary function, which may also lead to airway remodelling 6, 7. Recently, a new ciliary ultrastructural defect was identified in four adults with severe idiopathic bronchiectasis 8. The abnormality consisted of “cyst-like” structures located at the base of the cilia with the association of a small defect in function 8.
The absence of other ultrastructural defects of the cilia, and of other possible causes for bronchiectasis, allowed the authors to consider the newly described abnormality as a primary defect possibly involved in the development of bronchiectasis 8. However, adult patients may not be ideal to evaluate early-onset bronchiectasis and its association with an underlying genetic condition.
The aims of this study were to assess the correlation of cyst-like ciliary defects with the presence and severity of bronchiectasis, and to ascertain the primary or secondary nature of this ultrastructural defect in a prospectively recruited paediatric cohort.
Materials and methods
A total of 45 consecutive patients (22 males, 23 females) aged 0.6–18.0 yrs (mean±sd 7.6±4.5), suffering from recurrent lower airways infections and with chest radiographs with features of bronchiectasis, were enrolled between June 2000 and February 2003.
Seven patients had primary cilia dyskinesia (three with Kartagener's Syndrome), one had cystic fibrosis and 37 had recurrent bronchopneumonia (four of them were also asthmatic and nine also had recurrent otitis media and sinusitis).
High resolution computed tomography
In all patients a high resolution computed tomography (HRCT) was performed using a third-generation scanner (Sytech 3000; General Electric Medical Systems, Milwaukee, MI, USA). Slices (1‐mm thick) were obtained with 10‐mm spacing, in the supine position, at full inspiration 9. No intravenous contrast was injected and anaesthesia was needed in three patients. All images were reviewed by the same radiologist who was blinded to the clinical data. Bronchiectasis was scored from: 1) mild bronchial dilatation found in limited parenchymal areas; to 3) severe and diffuse bronchiectatic changes (fig. 1⇓ a, b, c), according to the extent of disease. Subjects with HRCT score 0 (no bronchiectasis) were used as controls.

Score of bronchiectasis: a) mild bronchial dilatation found in limited parenchymal areas (score 1); b) intermediate bronchiectasis (score 2); c) severe and diffuse bronchiectatic changes (score 3).
Cilia evaluation
In all patients, both ciliary motion analysis and transmission electron microscopy (TEM) evaluation of cilia were performed. Biopsies were obtained on nasal ciliated epithelium from two or more sites of the inferior turbinate. No patient reported respiratory infections or exacerbations of the chronic disease in the previous month, and medication was not taken in the 48 h prior to the study. Samples obtained using a cytology brush (Microvasive, Milford, MA, USA), were suspended in 2 mL Medium 199 fluid cell culture and in 2 mL normal saline for immediate light‐microscopic and TEM evaluation, respectively 10. Samples for ciliary motion analysis were kept at 37°C and transferred to a variable‐thickness culture chamber 11. Ciliary morphology, motion pattern and beat frequency were evaluated according to standardised methodology 2, 3, 7, 12.
Samples for ultrastructural studies were also prepared according to standardised methodology 13. Cilia were studied at a final magnification of ×103,000–207,000. For each specimen, an average of 14 ciliated cells and 120 random sections of cilia were examined to assess the presence of cyst-like structures within the ciliary shafts and any other structural defects. Ciliary motion analysis and ultrastructural evaluation were independently performed by two different experts.
In seven patients, it was possible to re-evaluate ciliary beat frequency and ciliary ultrastructure after a follow-up period of 2–22 months of aggressive treatment according to a standardised protocol 3.
Other analyses
To evaluate possible causes of bronchiectasis, additional tests were performed 5: the sweat test; α1‐antitrypsin; quantitative immunoglobulin (Ig); IgG subclasses; total IgE; leukocyte counts with differential cell counts; neutrophil chemotaxis; phagocytosis; neutrophil killing; T-lymphocyte subclasses, C3, C4 and CH50. Finally, congenital malformations (i.e. Williams-Campbell syndrome, cystic adenomatoid or hamartomatous malformations, etc.) were studied by analysis of the HRCT images acquired for the evaluation of the bronchiectasis.
Informed parental consent was obtained before enrolling the children and the study protocol was approved by the local hospital ethical committee.
Statistical analyses
Baseline variables are described as group mean±sd. Sensitivity, specificity, positive predictive value and negative predictive value of cyst-like structures within the ciliary shafts, as indicators of HRCT-proven bronchiectasis, were calculated. The statistical significance of correlations between the results obtained with TEM and HRCT were examined using Spearman's Rank Signed test. A p-value <0.05 was considered statistically significant.
Results
Ciliary motion analysis (abnormal motion patterns, including immotile cilia and/or ciliary beat frequency <6 Hz) and TEM evaluation of cilia (alterations of the central pair and dynein arms deficiencies, associated with a small proportion of swollen cilia and compound cilia) confirmed the diagnosis of PCD in seven children (15.5%). According to the clinical phenotype, three of them had Kartagener's syndrome 3, 6. In the remaining 38 patients (84.5%), ciliary motion analysis demonstrated abnormal patterns in a small proportion of cilia, prevalence of thick cilia and low ciliary beat frequency, although >6 Hz (7.9±1.6 Hz), compatible with secondary ciliary dyskinesia (SCD) 2–4, 7. In these subjects, TEM evaluation showed nonspecific abnormalities compatible with chronic inflammation (prevalence of swollen cilia and compound cilia).
Cyst-like structures within the ciliary shafts were demonstrated in 29 out of 45 patients (64.4%) and ultrastructural analysis showed that 0.7–37.5% of cilia displayed such a defect with variable size (fig. 2⇓). The defect was present both in patients with primary and secondary ciliary dyskinesia, and also in one patient with no documented bronchiectasis.

Cyst-like structures within the ciliary shafts.
In 10 subjects, no bronchiectasis (HRCT score of 0) could be demonstrated. All the children had recurrent bronchopneumonia, three also had asthma and one also had sinusitis. The clinical phenotypes of these patients were not different from the 35 (77.8%) patients with bronchiectasis, obviously excluding the three patients with situs inversus viscerum. The bronchiectasis scores for HRCT in these 35 patients were 1, 2 and 3, in 14, 13, and eight patients, respectively.
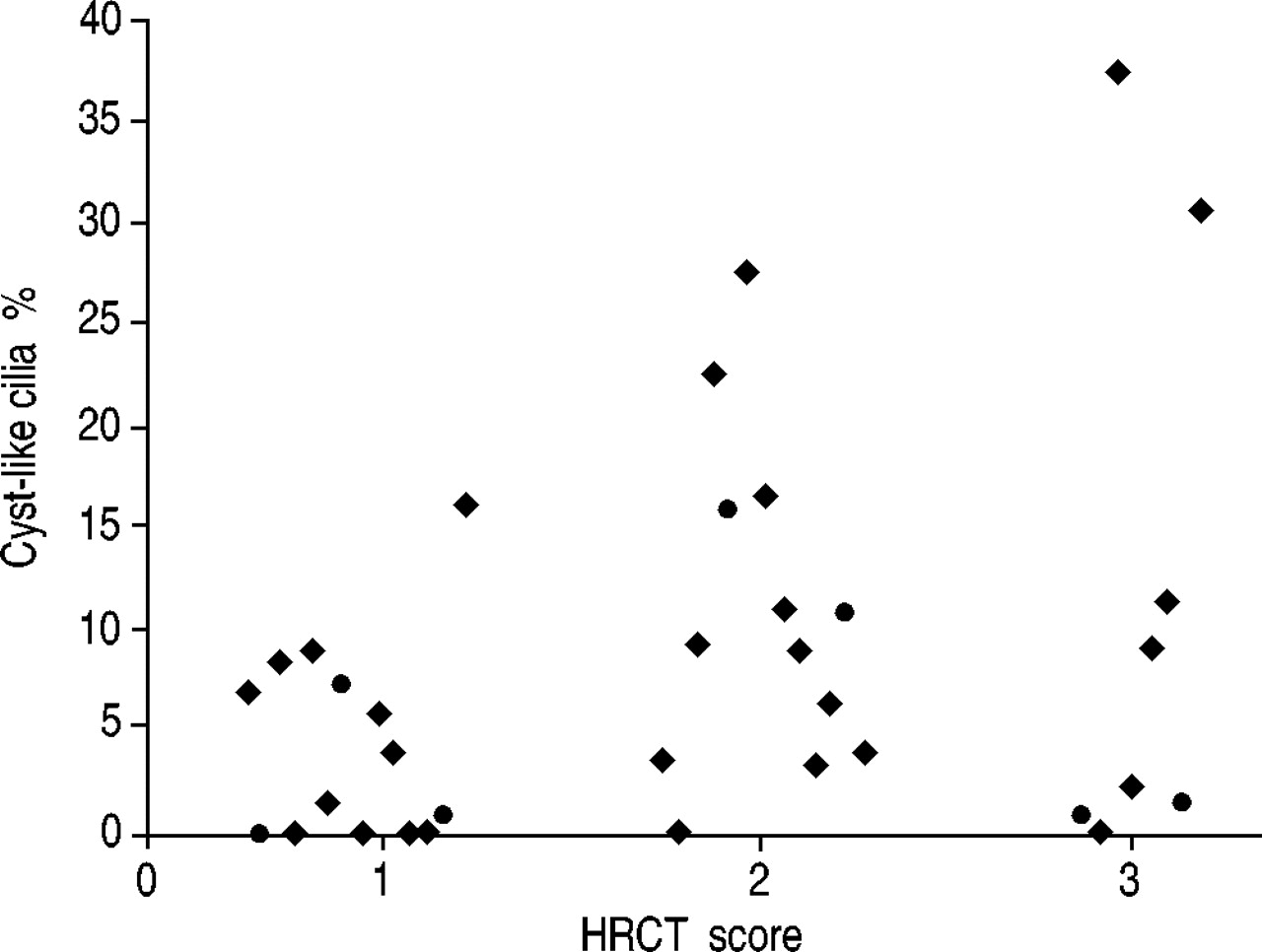
Individual percentages of cilia with a cyst-like lesion in relation to bronchiectasis HRCT score are reported in figure 3⇓. This figure depicts the subjects with PCD (seven patients) and the subjects with SCD (28 patients).

{kind=link}
{kind=link}
{kind=link}
Percentage of cilia with cyst-like lesions in relation to high resolution computed tomography (HRCT) score for bronchiectasis (35 subjects). •: primary ciliary dyskinesia; ♦: secondary ciliary dyskinesia.
The presence of cyst-like structures, as an indicator of HRCT-proven bronchiectasis in all patients together (PCD and SCD), had a sensitivity of 80% and a specificity of 90%. The positive predictive value was 96.6% and negative predictive value 56.2%. In subjects with SCD, sensitivity was 78.6% and specificity 90%. Positive predictive value was 95.6% and negative predictive value 60%. Spearman Rank Signed correlation test demonstrated a significant correlation between the per cent of cyst-like structures within the ciliary shafts and the HRCT score (p=0.039). No immunological defects, including functional assessment (response to anti-polio vaccine), nor α1‐antitrypsin deficiency were found in the present study population. Furthermore, no congenital malformation was observed at HRCT.
Seven patients were re-evaluated 2–22 months after the initial examination. During this period they received antibiotic treatment and chest physiotherapy. In five cases, the cyst-like structures disappeared. These five patients had SCD and the HRCT scores were: 1 in two patients, 2 in one child and 3 in two subjects. In the remaining two patients with PCD and a HRCT score of 2, the defect persisted although with a reduced intensity (from 15.8 to 6.8% and from 10.8 to 7.3% of the cilia). In these two patients the follow-up was 3 months for one patient and 2 months for the other.
Discussion
Cyst-like structures within the ciliary shafts were described for the first time in four adult patients with otherwise normal microtubular ultrastructure by Tsang et al. 8. The authors attributed a pathogenetic role to this defect in the development of bronchiectasis and hypothesised that these cyst-like structures were a primary defect on the basis of their persistence in the 3–12 months follow-up 8.
In the children in the current study, cyst-like structures were demonstrated both in subjects with idiopathic bronchiectasis and in patients with bronchiectasis related to PCD. Furthermore, after antibiotic therapy given during the follow-up, the defect completely disappeared in the five children with SCD and was reduced in the two patients with PCD. Although the follow-up was only performed in seven patients, the disappearance of the defect suggest that these cyst-like structures are an expression of the chronic airway inflammation that often occurs with other ultrastructural abnormalities 7, 14. Data on sputum microbiology was not obtained in the current study, so no specific bacterial infection can be related to the detected abnormalities. It is also unlikely that the cyst-like appearance is due to an artefact of tissue specimen processing, since if this was the case it should have occurred both at the beginning and at the follow-up evaluation. Furthermore, the possibility of an error in the evaluation of biopsies of cilia was reduced by the use of two independent observers looking at 120 random sections of cilia. In addition, the functional abnormalities found in all patients with different conditions other than PCD are most probably related to chronic inflammation and are classified as SCD 7, 15–17. Cyst-like structures may effectively be a consequence of deciliation by harmful agents, as previously reported for different abnormalities in humans and experimental animals 18, 19. Therefore, the meaning of these alterations might be nonspecific, comparable to that of compound cilia, of membrane‐deficient cilia and of giant cilia 17, 20. In fact, even in the absence of PCD, some viral infections can cause a transient but severe impairment of mucociliary clearance for up to 4 months 21. Moreover, some bacterial infections (Pseudomonas sp., Haemophylus, Pneumococci, Chlamydiae and Mycoplasma) are ciliotoxic and cause reversible ciliostasis, which may impair mucociliary clearance for months 22–24.
To further support the authors' hypothesis, a reduction in the percentage of defected cilia was also observed in the two patients with PCD. In those patients where it was not completely reversed, a follow-up of 2–3 months is probably too short a period to show a significant reduction in the structural defect in the presence of a disease usually associated with severe airway inflammation. Equally, disease duration and severity in patients described by Tsang et al. 8 may explain the persistence of cilia abnormalities.
Although it may be suggested that these basally situated cyst-like structures could affect, primarily, the beating of the cilia itself and secondarily that of the neighbouring cilia 8, it is also possible that the functional impairment is a global consequence of inflammation. This was previously observed for swollen and compound cilia 7, 14, 15. This also seems to be the case for cyst-like lesions in consideration of the complete or partial reversibility of the ultrastructural defect in SCD and PCD, respectively. Furthermore, the high specificity and high positive predictive value of cyst-like cilia structures as an indicator of the presence of bronchiectasis in children with both PCD and SCD represent a strong argument in favour of its inflammatory origin. However, the significant correlation between TEM cilia dysfunction and HRCT score suggests that the percentage of the affected cilia, even though not pathogenetic, might have a prognostic impact on the clinical conditions. As a consequence, their identification requires an appropriate aggressive management plan to prevent and possibly reverse airways damage 3, 7.
In conclusion, in children, ultrastructural changes of the cilia are secondary to chronic infection and can be resolved after appropriate long-term treatment.
- Received July 24, 2003.
- Accepted January 21, 2004.
- © ERS Journals Ltd
References









