





Abstract
The objective of this study was to describe a nosocomial outbreak of influenza during a period without influenza epidemic activity in the community.
Outbreak investigation was carried out in an infectious diseases ward of a tertiary hospital. Presence of two or more of the following symptoms were used to define influenza: cough, sore throat, myalgia and fever. Epidemiological survey, direct immunofluorescence, viral culture, polymerase chain reaction, haemagglutination-inhibition test in throat swabs and serology for respiratory viruses were performed.
Twenty-nine of 57 healthcare workers (HCW) (51%) and eight of 23 hospitalised patients (34%) fulfilled the case definition. Sixteen HCW (55%) and three inpatients (37%) had a definitive diagnosis of influenza A virus infection (subtype H1N1). Among the symptomatic HCW, 93% had not been vaccinated against influenza that season. Affected inpatients were isolated and admissions in the ward were cancelled for 2 weeks. Symptomatic HCW were sent home for 1 week. On the seventeenth day of the outbreak the last case was declared.
The incidence of cases in this outbreak of influenza, which occurred during a period without influenza epidemic activity in the community, was notably high. Epidemiological data suggest transmission from healthcare workers to inpatients. Most healthcare workers were not vaccinated against influenza. Vaccination programmes should be reinforced among healthcare workers.
Influenza can be transmitted between patients and healthcare workers (HCW) in the hospital setting resulting in increased morbidity and mortality, especially in immunocompromised patients 1, 2. Recently, it has been recognised that acquired immune deficiency syndrome (AIDS) patients have a significantly higher mortality due to pneumonia or influenza during influenza seasons 3. Persons in contact with high-risk individuals are an important potential source of influenza exposure. It has been demonstrated that vaccination of HCW is associated with a lower mortality rate among nursing home patients 1, 4, 5. The World Health Organization and the Center for Diseases Control recommend vaccination for HCW, with particular emphasis on persons who care for members of high-risk groups 6, 7. However, compliance with vaccination is usually poor among HCW 8, 9, a fact that is mainly due to several misconceptions concerning vaccine-related adverse reactions.
Generally, special precautions for the prevention of nosocomial spread of influenza are only undertaken when an epidemic is identified in the community. This study reports an outbreak of respiratory illness (RI) among HCW and inpatients in the infectious diseases and AIDS hospitalisation ward of a tertiary care hospital during a nonepidemic influenza period in the community. The results of the investigation to determine the causes and characteristics of the outbreak, as well as the measures implemented in order to control it are described.
Methods
The affected infectious diseases and AIDS hospitalisation ward is a 23-bed ward in an 800-bed tertiary care hospital with a mixed population of AIDS (45%) and infectious diseases non-AIDS patients (55%), with 57 active HCW. Close to the hospitalisation ward, there is an AIDS daycare hospital. The ward and daycare hospital comprise an area of 500 m2.
Epidemiological survey
For the purpose of the epidemiological investigation, a case is defined as any person who during the outbreak period had an acute respiratory illness with two or more of the following symptoms: cough, sore throat, myalgia and fever (>37.7°C). A survey was conducted, recording demographic data (name, sex, age and professional HCW category), date of first symptoms, recent travels, current therapy and major symptoms (fever, cough, sore throat, myalgia and headache). A chest radiograph was performed in HCW with high-grade fever (>38.5°C) and in all symptomatic inpatients. All cases underwent blood analysis and biochemistry including C-reactive protein.
Data concerning HCW influenza vaccination were obtained from the Employee Health Service records. Influenza vaccination status in patients was obtained by interview.
An assessment was conducted in order to know whether there was an influenza epidemic in the rest of the hospital and in the community. These data were obtained from the laboratory of Microbiology of the hospital, which is a World Health Organization Regional Influenza Center. RI and influenza rates were calculated as cases per 100.
Microbiological studies
A throat swab was obtained from all RI patients and immediately sent to the laboratory in viral transport medium (Hank's balanced salt solution with 1% bovine albumin fraction V supplemented with penicillin, streptomycin and gentamycin).
The following studies were performed in all samples: 1) direct immunofluorescence for influenza A and B viruses, adenovirus, respiratory syncytial virus and parainfluenza 1, 2 and 3 viruses (Respiratory Panel 1; Chemicon International Inc., Temecula, CA, USA); 2) isolation of these viruses was attempted by using three different cellular lines (MDCK, A-549 and Hep-2; Vircell SL, Granada, Spain); and 3) subtyping of the influenza virus A haemagglutinin was done by reverse transcriptase polymerase chain reaction 10 and confirmed by haemagglutination-inhibition test at the National Institute for Medical Research (Mill Hill, London, UK). In addition, all cases underwent detection of complement fixation antibodies for influenza A and B viruses, adenovirus, respiratory syncytial virus and parainfluenza 1, 2 and 3 viruses in two paired samples (Virion-Serion, Würzburg, Germany), and immunoglobulin (Ig)M and IgG antibodies to Chlamydia pneumoniae (Chlamydia pneumoniae IgG and IgM Micro IF Test; Labsystems, Helsinki, Finland), Mycoplasma pneumoniae (Mycoplasma pneumoniae, Genzyme Virotech ELISA; Virotech, Rüsselsheim, Germany) and Legionella pneumophila (Legionella pneumophila, Micro IF-line; Vitaltech, Barcelona, Spain). A definitive diagnosis of influenza was made when a RI patient had one or more positive test for influenza A virus.
Statistical analysis
Continuous variables are expressed as mean±sd. Frequencies are expressed as percentages. The Chi-squared test was used in order to compare frequencies.
Results
Susceptible population
When the outbreak was first detected there were 57 active HCW in the hospitalisation ward and daycare hospital, of which only four (7%) had been vaccinated for the current season. At that time, there were 23 inpatients in the hospitalisation ward, 11 of them (47.8%) with AIDS. According to data from the Regional Influenza Surveillance System, during the 2000–2001 season there had been no epidemic influenza activity in terms of local or regional outbreaks in the geographic area of this study. Only sporadic cases were detected 11.
Outbreak description
From February 10 to 26 2001, 29 out of 57 HCW (51%) and eight out of 23 inpatients (34%) complained of a RI that met the case definition. Four of the symptomatic patients had AIDS. Sixteen out of the 29 symptomatic HCW (51%) and three of the eight symptomatic inpatients (37%) had a definitive influenza diagnosis. The incidence rate of confirmed influenza among human immunodeficiency virus (HIV)and non-HIV patients in this outbreak was 9% and 16%, respectively (p=0.53). One AIDS patient with negative influenza tests had positive complement fixation antibodies for parainfluenza 2 virus and one HCW with confirmed influenza by culture of throat swab also had positive complement fixation antibodies for syncytial respiratory virus. The remaining diagnostic tests for other respiratory pathogens were negative.
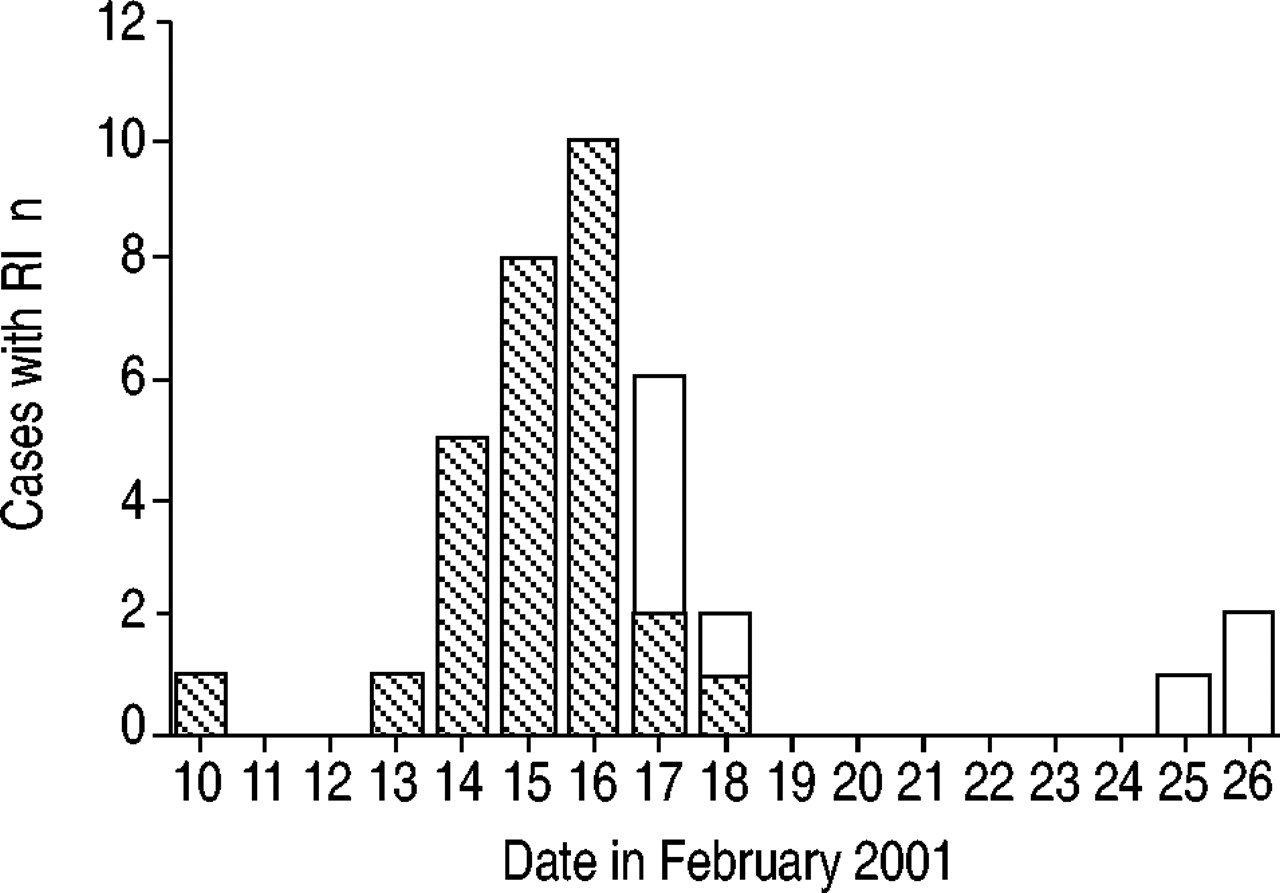
Apparently, the index case was a nurse aide, who was on a sick leave due to a RI at the time the outbreak was detected. She was evaluated 8 days after the onset of RI, and laboratory confirmation of influenza was not obtained. She had not been travelling in areas with documented epidemic influenza activity. No new cases were detected after day 17 since the onset of the outbreak. The epidemic curve is shown in figure 1⇓.
{kind=link}
Epidemic curve of the respiratory illness (RI) outbreak in the infectious diseases ward in February 2001. (□): inpatients; (┘): healthcare workers.
Distribution of professional categories of affected HCW was as follows: 12 physicians (41.3%); eight nurses (27.5%); five nurses' aides (17.2%); two housekeepers (6.8%); one student (3.4%) and one social worker (3.4%). Two of the 29 affected HCW (6.8%) had been vaccinated in the current vaccination campaign. They had a slight and short course of the RI without fever and influenza was not confirmed. None of the 11 admitted AIDS patients had been vaccinated in the current campaign due to different reasons, as follows: active injection drug use, advanced HIV infection, terminal situation and/or social problems. Clinical data in HCW and hospitalised patients are shown in table 1⇓. Eighty per cent of the admitted patients were receiving anti-inflammatory therapy or pain relievers during the study period.
Clinical data among symptomatic healthcare workers (HCW) and inpatients
Among HCW, the nine chest radiographs performed were normal. Among inpatients, only one had new bilateral pulmonary infiltrates (the one fatal case) and the others had no changes as compared with recent chest radiographs. The mean±sd leukocyte count was 5783±1737×109·L−1 with a normal distribution of white cells.
The only fatal case was a 30-yr-old female with AIDS, CD4+ cell count <50·mL−1 and viral load of 122,000 HIV-ribonucleic acid copies·mL−1 who was under antineoplasic therapy for a non-Hodgkin lymphoma. The patient was admitted 15 days before the onset of the outbreak. On day nine of the outbreak, fever, myalgia, cough and new bilateral pulmonary infiltrates, with a positive direct immunofluorescence and culture for influenza A virus in a bronchial aspirate, developed. Oral amantadine (100 mg orally b.i.d.) was started, as well as parenteral broad spectrum antibiotics and trimethoprim-sulfamethoxazole, but respiratory distress ensued and finally the patient died. Autopsy findings were those of an acute distress respiratory syndrome.
Control measures (see below) were implemented on day seven of the outbreak. During subsequent days, three HCW and eight inpatients complained of RI. On the seventeenth day of the outbreak two additional inpatients became symptomatic, but afterwards no new cases were observed (fig. 1⇑).
All of the thirteen influenza A virus isolates were identified as subtype (H1N1), antigenically closely related to A/New Caledonia/20/99 and A/Madagascar/57794/00 (as the majority of H1N1 viruses recently isolated in Spain).
Control measures
Symptomatic HCW were sent home for 1 week. Inpatients with RI were isolated under respiratory precautions (single room, gloves, mask). The number of staff and visitors entering rooms of patients with influenza was minimised. Admissions in the ward were cancelled for 2 weeks. Amantadine (100 mg orally b.i.d., adjusted by renal clearance) was administered to symptomatic inpatients and recommended to symptomatic HCW. Influenza vaccine (A/New Caledonia/20/99 (H1N1), A/Moscow/10/99 (H3N2) and B/Beijing/184/93-like virus) 12 was administered to nonvaccinated asymptomatic inpatients and offered to all nonvaccinated HCW from the infectious diseases and AIDS hospitalisation ward and daycare hospital.
A surveillance and prevention protocol, including vaccination and amantadine were offered to inpatients and HCW of all other wards in the hospital. Implementation of this protocol was promoted via staff meetings, with particular emphasis on haematology, oncology and transplant facilities. Thirty-one of the 3,500 HCW from other wards had a RI during the epidemic period (incidence rate of RI among HCW=0.88%), but none of them had any relationship with the affected ward. Influenza vaccine was administered to 141 nonvaccinated HCW and 90 inpatients, without remarkable adverse effects. Thirty-two inpatients received prophylactic amantadine over 2 weeks, without remarkable side-effects. The occurrence of adverse effects was recorded by means of warning physicians to notify the Service of Pharmacy of any clinically relevant systemic, neurological, digestive or cutaneous adverse effects attributable to the vaccine or to amantadine.
Discussion
This report emphasises the need to consider the diagnosis of influenza in RI nosocomial outbreaks with a high attack rate even during nonepidemic influenza periods, the efficacy of the adopted control measures and the urgent need for efficient vaccination programmes among HCWs, especially those in contact with immunocompromised patients.
Viral subtyping demonstrated that all the influenza viruses recovered from case patients and HCW were antigenically similar, which confirms the relatedness of the isolates and their probable common source.
It is of note that this outbreak took place in a nonepidemic influenza period. Although the time of the outbreak was February, i.e. during the normal influenza season in the Northern hemisphere, according to data from the regional surveillance system, there was no regional or local epidemic activity of influenza in Spain during the 2000–2001 season; only sporadic cases were detected. This is quite unusual since nosocomial outbreaks of influenza usually occur at the time of epidemics, when the prevalence of asymptomatic carriage of influenza virus in the general nonimmunised population is high 2, 13. Factors that probably contributed to the present outbreak could be the absence of vaccination among HCW and overcrowding. The latter has been shown to be a risk factor for the spreading of virus in healthcare settings 14. The immunisation status of HCWs and patients in healthcare settings is probably one of the most important factors that can contribute to the development of outbreaks. In this case, even with a good antigenic match between the vaccine viruses and the viruses isolated during the outbreak, two of the four vaccinated HCW experienced an illness that fitted the case definition of RI. However, they experienced a slight and short course of RI without fever and influenza was not confirmed. Some authors have noted the different spread patterns of influenza depending on the immunisation status of the population. In partially immunised people, such as those living in nursing homes, the spread can be slow and prolonged during several months. That is in contrast to the explosive nature of the outbreaks described in nonimmunised populations, such as patients hospitalised in acute care facilities 15, 16. A feature of influenza in immunocompromised persons, including HIV patients, is the prolonged virus shedding 17. This may be another factor to take into account in this outbreak since the first case could have been an HIV outpatient infected by influenza who attended the daycare clinic, although it was not detected. The apparent index case was a nurse aide that had not been travelling in areas with documented epidemic influenza activity. She was evaluated 8 days after the onset of RI and laboratory confirmation of influenza was not obtained. It is known that the sensitivity of the influenza tests decreases 4 or 5 days after the onset of the illness.
According to table 1⇑, symptomatic inpatients had significantly less myalgia and headache than HCW. This could be explained by the fact that the majority of these patients were receiving anti-inflammatory therapy and pain relievers for other symptoms during the outbreak.
Epidemiological data suggest that in this outbreak influenza was transmitted from HCW to inpatients. HCW have been occasionally identified as index cases in nursing-home outbreaks 18, 19. Up to 23% of HCW might present clinical or subclinical influenza infections at the time of epidemics 13. The current report confirms that nosocomial influenza is of high risk in acute healthcare centres where the vaccination compliance rate among HCW is low, even in nonepidemic influenza periods in the community. Moreover, the risk can be high in patients who are old or have any kind of immunodeficiency even if they are vaccinated, since the efficacy of vaccination among these patients can be lower 18, 20. Therefore, the best way of protecting inpatients from influenza is by vaccinating HCW and household members who have contact with them 6.
Influenza vaccine is effective in preventing influenza infection in HCW and may reduce days of absence 21. Interestingly, in the Northern hemisphere the trivalent vaccine for the 2000–2001 season included the A/New Caledonia/20/99 (H1N1)-like virus, similar to the subtype isolated in the outbreak. Therefore, if compliance with influenza vaccination among HCWs had been achieved in this season the outbreak could have been avoided. It has been demonstrated that the attack rate of influenza outbreaks in nursing homes and chronic care facilities depend to some extent on vaccination status of residents and staff members 22, 23. In fact, immunisation of HCW results in significantly reduced morbidity and mortality among patients in long-term facilities 1, 4, 5, although it is unclear whether the reduction in mortality of patients associated with vaccination of HCWs is directly due to prevention of influenza 24. Although there an influenza vaccination programme exists in the authors hospital, this outbreak demonstrates that the compliance rate among HCWs is extremely low, even in a country were the vaccine compliance in the community is the highest in Europe 25, 26. Infection control teams have used a variety of tactics to improve HCW compliance with influenza vaccination 27, 28, however, important barriers exist between current rates of compliance and the goal of universal HCW vaccination. A recent study demonstrated that more intensive promotion of influenza vaccine among HCW had a minimal impact on uptake rates 29. More studies concerning the reasons for this resistance are necessary.
It is accepted that the detection and control of a nosocomial influenza outbreak is difficult to perform in large institutions. Moreover, the value of the recommended infection control procedures for influenza has not been proved, probably due to the fact that it is difficult to estimate the benefit of a single infection control measure, as all of them are implemented at the same time. In contrast with other nosocomial influenza outbreaks, which have important numbers of cases and a longer duration 1, and considering the high attack rate of this outbreak, the timely clinical, epidemiological and microbiological diagnosis and the quick institution of infection control measures prevented its spread to the rest of the hospital and shortened its duration. Given the prolonged shedding of the virus from infected persons, sending home the affected HCW was probably one of the most effective measures adopted, especially in the current authors setting, since HCW usually report to work even when they experience a febrile respiratory illness 21.
In contrast with other publications, no clinically relevant adverse reactions to amantadine were detected among patients and staff 8. However the authors protocol was designed to detect clinically relevant adverse effects and slight side-effects were probably undetected. Although new agents, such as the neuraminidase inhibitors zanamivir and oseltamivir, are being introduced to clinical practice and probably will be useful for an easier control of outbreaks 30, 31, there is still little information about their efficacy in control of outbreaks and so they cannot be recommended for general use. This is why the authors did not use them as prophylactic agents during the outbreak.
Previous reports suggest that HIV-infected patients do not have an increased risk of influenza, although influenza may be more severe and have more complications among HIV-infected persons and other immunocompromised patients 3, 32, 33, 34. This is confirmed in the current report as the incidence of confirmed influenza among AIDS patients was similar to that of non-AIDS patients, but the one fatal case was a woman with AIDS and a non-Hodgkin lymphoma.
In conclusion, this nosocomial influenza outbreak occurred in a nonepidemic influenza period among nonvaccinated healthcare workers, who probably transmitted it to inpatients causing increased morbidity and mortality. The measures implemented allowed a rapid control of the outbreak avoiding its spread to the rest of the hospital. There is an urgent need for efficient influenza vaccination programs among healthcare workers, especially those in contact with immunocompromised patients.
- Received May 16, 2002.
- Accepted August 9, 2002.
- © ERS Journals Ltd
References









